Abstract
When the volume of tissue loss due to trauma is too great for surgical reconstruction alone, a prosthesis may be indicated to complete the rehabilitation of the patient. Maxillofacial prosthodontists can be valuable members of the surgical and restorative team to ensure the successful treatment following severe trauma. It is important to note that, besides the ability to provide support with the fabrication of a prosthesis, the maxillofacial prosthodontist can also help with the planning of the surgical reconstruction to ensure proper function, esthetics, and phonetics are achieved. This chapter will present an overview of maxillofacial prosthetics, with the considerations for a successful prosthetic rehabilitation.
Keywords
maxillofacial prosthodontics, prosthesis, prosthodontic rehabilitation
Background
The replacement of missing structures in the head and neck region has been a concern for many centuries, with the fabrication of maxillofacial prosthetic restorations being mentioned since the 16th century, with the first mention often credited to Ambroise Paré in 1541. Although the concern was often the restoration of a pleasing appearance, addressing the functional disruption was also part of the treatment, with clinicians being able to achieve the desired outcome with varying degrees of success.
Maxillofacial prosthetics is often described as “the art and science of anatomic, functional, or cosmetic reconstruction by means of non-living substitutes of those regions in the maxilla, mandible, and the face that are missing or defective because of surgical intervention, trauma, pathology, developmental or congenital malformation.”
Maxillofacial prosthetic rehabilitation is best understood when the treatment is put in context with the overall patient care. In order to achieve the desired outcome, head and neck surgeons, plastic surgeons, oral surgeons, and the maxillofacial prosthodontist should all be involved in the treatment plan process, so proper site preparation in anticipation of prosthetic reconstruction can be successful. The concept of multidisciplinary care is very evident in the management of patients who will require maxillofacial prosthetic rehabilitation, as this interaction will facilitate the fabrication of a prosthesis, which can restore the patient to near normal function and esthetics in many cases.
The general goals when dealing with maxillofacial patients should be to restore form, function, and esthetics. Prosthodontic rehabilitation aims to create maintainable health for the total masticatory system. This means freedom from disease in all masticatory structures, a healthy maintainable periodontium, stable temporomandibular joints, stable occlusion, healthy maintainable teeth, comfortable function, and of course, optimum esthetics. Practicing without a clear and comprehensive understanding of these goals exacts a costly penalty in missed diagnosis, unpredictable treatment results, and lost productive time.
Prosthetic reconstruction of the trauma patient can be difficult due to the deformity created and the loss of vital structures. Oftentimes the construction may not be accomplished without several revisions on the site. Initial treatment will always involve closing the wound and stabilizing the patient, so prosthetic reconstruction does not become a relevant aspect of treatment until several months after the initial incident.
Oral and Dental Anatomy Evaluation
It is important for the medical personnel treating head and neck patients (otolaryngologists, plastic surgeons, and speech pathologists, among others) to understand the oral cavity and dental anatomy, so they can identify and accurately communicate findings with their dental colleagues, as teeth and anatomical landmarks of the jaws are usually used as reference for the prosthetic planning before and after the surgery. In general terms, the most commonly used scheme for identification of adult teeth involves the sequential numbering (from 1 to 32) starting from the right maxillary third molar (tooth number 1), and moving across to the contralateral third molar (tooth 16), starting again from the lower left third molar (tooth 17) across to the right mandibular third molar (tooth 32). All missing and impacted teeth should be counted in this system. Anatomical structures of importance for retention and support of prostheses include the tuberosity, alveolar ridge, the hard palate on the maxilla, the alveolar ridge, the retromolar pad, and buccal shelf on the mandible.
An essential principle in prosthodontics is the determination of the correct physiologic maxillo-to-mandibular position. This relationship must always be determined before we can determine the correct alignment and occlusal position of a prosthesis. The maxilla is affixed to the skull and the mandible can be considered a moving entity. As such, the functional movements of the mandible constitute the most fundamental basis for ideal prosthesis design. Therefore, we must consider the envelope of function as it is not merely an academic exercise. The range and limits of mandibular movement are indirectly related to the limits imposed by the postsurgical anatomy. Surgery affects the maxillomandibular ligaments, bone, muscle, and the temporomandibular joints. How much or how little varies from person to person and is affected by the surgery.
It is also important for those involved in treatment to be able to recognize the oral pathology resulting from poor oral health status. For example, advanced periodontal disease, gross dental caries, and excessive plaque and calculus formation are indicators of poor oral hygiene. These findings should be noted when referring the patient to the clinician who will perform a thorough radiographic and dental examination. Commonly in trauma patients previous dental casts are not available, so this examination may include acquisition of impressions from dental and facial structures as needed. The casts fabricated from these impressions can be used as aids in the treatment planning and posttreatment rehabilitation. Furthermore, the identification of hopeless teeth (i.e., severely decayed, extensive fractures) that need to be extracted will be made as well as weighing the need for any restorative treatments. Assessment of available soft and hard tissue can also be done at this appointment and, if possible, further advance imaging is obtained to evaluate available bone for future placement of osseointegrated dental implants.
Preservation of tissue at the time of surgery should be carefully examined, as it may require further revisions of the surgical site, as the remaining tissue can create challenges during prosthetic reconstruction. It is important for the surgeon and the prosthodontist to understand the limitations of each case to better prepare the site for future prosthetic reconstruction.
Assaults, motor vehicle collisions, falls, and gunshot wounds are the major causes of fractures in the head and neck area. The resultant defect can significantly impact the patient functions, as the separation between the oral and nasal cavity can be compromised, causing air leakage during normal functions.
Ideally, the defect created can be reconstructed with primary closure. This is the best outcome for the patient, as little to no disruption will occur. However, the defect created can be too big for primary closure to occur, and hard and soft tissue transfers to reconstruct the area are not possible due to concerns regarding morbidity of the donor site, cost of the procedure and hospitalization time, patient desire to avoid further surgery, or other health problems. In these situations, reconstruction with a prosthesis is indicated.
During the initial fracture reductions and reconstruction, it is important to preserve as much as possible of the existing structures. For instance, if the patient is edentulous, the hard palate is responsible for primary retention, support, and stability of a prosthesis. Without compromising the surgical outcome, surgeons should be encouraged to preserve as much of the hard palate and alveolar bone as possible. On a dentate patient, besides the preservation of bone, maintaining key teeth can dramatically improve prosthetic outcome, as the remaining dentition can be used for retention and stability.
As is often the case, a revision surgery may be required to further improve the reconstruction or address some common problems (i.e., excessive tissue scarring and contractures) to help the patient regain normal or close to normal function. During this revision procedure, if prosthetic reconstruction is going to be recommended, the consideration for lining the surgical site with keratinized tissue should be made, as a split-thickness skin graft placed during the surgical procedure – after a few weeks of maturation – can be easily maintained by the patient, in addition to being a stable area for the prosthesis. Also, during closure of the wound, the surgeon should remove any tissue tags or redundant tissue, as these structures can prevent proper prosthetic extension.
If reconstruction using free tissue flaps is planned, an attempt should be made to keep the flap from being too bulky, as this extra tissue will require subsequent surgical revisions to allow proper space for the fabrication of a prosthesis ( Figs. 3.11.1 and 3.11.2 ).


It is important also to emphasize that in an ideal situation, a team approach will be used from the beginning of treatment. This will result in the best outcome for patient rehabilitation.
Intraoral Prosthetic Rehabilitation
The maxillofacial prosthetic rehabilitation is usually achieved in three different phases: surgical, interim, and definitive. This process usually is completed within a year, depending on the clinical situation and treatment needs.
The surgical phase occurs at the time of surgery; in the case of the maxilla, when a surgical obturator is placed to reestablish the separation between the oral and nasal cavities, while restoring proper palatal contour. This is a very important procedure, as the prosthesis will help maintain proper speech and swallowing function immediately after surgery, thus decreasing the need for a nasogastric tube, and speed recovery and discharge from the hospital. The surgical obturator will also serve to maintain proper lip and cheek support during the initial healing, and decrease the facial contracture that can happen due to scarring of the tissues. Finally, this prosthesis will serve to maintain a split-thickness skin graft in place, which is part of site preparation for prosthetic reconstruction. In the case of traumatic injury, this step is usually not possible as the fabrication of the surgical prosthesis cannot be accomplished prior to the surgery.
After initial healing has taken place (10–14 days), the surgical obturator is replaced with an interim obturator. While a surgical obturator may not have replaced any missing teeth as a result of the surgery, the interim obturator will most likely have teeth so the patient can slowly attempt to return to normal function. This prosthesis will be adjusted constantly as the surgical site heals, and the defect created will be changing in size and shape. The adjustments will require addition or removal of material accordingly, so optimal separation between oral and nasal cavity is maintained.
Once the healing of the surgical site has been completed, the fabrication of the definitive obturator begins. This prosthesis will further enhance esthetics and function.
In cases of mandibular involvement, the initial evaluation is very similar to that of the maxilla. However, it is important to emphasize that proper maintenance of the alignment of the remaining segments after the fracture reduction is a crucial step for subsequent prosthetic rehabilitation. If the alignment of the remaining mandible to the glenoid fossa and the temporomandibular joint is disrupted, damage to the surrounding areas will occur and the patient’s normal mandibular motions will be affected, resulting in an improper occlusion. As a consequence, the prosthetic reconstruction will be less than ideal, if not impossible.
To maintain proper alignment of the mandibular segments during mandibular surgery, the utilization of fixation plates and screws is a commonly available technique. If no mandibular reconstruction is being planned due to the amount of tissue loss, the removal of the condyle and the remaining ramus on the affected side should be completed, to prevent the medial migration towards the maxilla, and decrease the chances of complications due to compromised function and prosthetic rehabilitation.
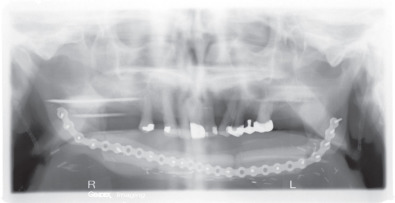
Reconstructive surgery using free flaps and bone transplantation has greatly improved the surgical outcome for patients requiring a surgical procedure, which will affect the continuity of the mandible ( Fig. 3.11.3 ). Virtual surgical planning utilizing CT scans can also allow the members of the surgical and reconstructive team to rehearse the procedures to be done, and evaluate the outcome. This has become an invaluable tool, allowing for the fabrication of individualized reconstruction plates, cutting guides for the harvesting of bone grafts, and stents for the placement of osseointegrated dental implants.