Abstract
The chapter describes the workup and management of nasal fractures. Contemporary literature related to nasal fractures is reviewed, including anatomy, pathophysiology, radiography, surgical indications, techniques, follow-up care, and potential complications. Nasal fractures are common, although not all fractures require intervention. Those that meet criteria for reduction can be effectively managed with minimal complications by adhering to established principles.
Keywords
nasal fracture, septoplasty, trauma, facial trauma
Background
Nasal bone fractures are the most common type of facial bone fracture, accounting for at least half of all adult facial fractures. The annual incidence of nasal bone fracture ranges from 0.053% to 0.37%, with peak incidence in adolescence or early adulthood. Most nasal fractures are due to accidents (41%), with assault (31%) and sports (29%) also prominent etiologies. Nasal bone fractures are frequently associated with cartilaginous and soft tissue injuries. Fractures of nearby facial bones may also occur, with orbital blowout and zygomaticomaxillary complex (ZMC) fractures being most common.
Surgical Anatomy
The nasal bones are paired, and attach to the nasal process of the frontal bone superiorly, frontal process of the maxilla laterally, upper lateral cartilages inferiorly, contralateral nasal bone medially, and septum internally. The septum is made up of the quadrangular cartilage anteriorly, perpendicular plate of the ethmoid superiorly, the vomer posteroinferiorly, and the crest of the maxillary and palatine bones inferiorly.
The blood supply of the external nose is robust and receives contributions from the internal carotid artery via the dorsal nasal branch of the ophthalmic artery and the external carotid artery via the lateral nasal and septal branches of the facial artery.
Sensation of the nasal dorsum is derived from the ophthalmic branch of the trigeminal nerve, while the nasal sidewalls are innervated by the maxillary branch of the trigeminal nerve.
Clinical Presentation
History
Upon encountering a patient with nasal trauma, it is important to first establish the timing and mechanism of injury. The history is likely to provide clues to the pattern and severity of the fractures. A lateral blow to the nose, such as from an assault or being elbowed during a sports game, tends to result in lateral displacement of the nasal pyramid. On the other hand, a frontal blow, such as from a fall or from steering wheel impact in a motor vehicle crash, is more likely to result in frontal depression of the nasal bones with potential impaction of the nasal bones and nasal septum.
It is important to inquire about associated symptoms such as nasal airway obstruction, change in external appearance of nose, and epistaxis. Trauma resulting from a high force of impact or the presence of unusual symptoms including clear rhinorrhea, vision changes, diplopia, facial numbness, trismus, and/or change in occlusion should prompt investigation for other concomitant fractures. It is also important to establish any prior history of nasal trauma or nasal surgery as these patients are more likely to require secondary reconstruction after initial management of their fracture.
Physical Examination
The goal of the physical examination is to determine the extent and severity of the injury in order to counsel the patient appropriately regarding optimal management and outcome expectations. Examination should begin with a visual inspection for nasal deformity or deviation and noting any soft tissue injuries. Photo documentation of the external appearance of the nose is important for preoperative and postoperative counseling of the patient ( Fig. 1.10.1 ). It is often helpful to compare the external appearance to a photograph from prior to the injury.

Gentle palpation of the nasal dorsum should be performed in order to evaluate for the extent of displacement, depression, or lateralization of the nasal bones. The keystone region, the junction between the nasal bones and upper lateral cartilages, should also be palpated as trauma may result in disruption of this critical support region, leading to middle vault collapse. The nasal tip should be palpated to assess for potential loss of septal support.
An internal nasal examination with anterior rhinoscopy and nasal endoscopy should be performed to evaluate for septal fracture, septal hematoma, epistaxis, and clear rhinorrhea. A septal hematoma, if identified, must be drained as quickly as possible to avoid septal cartilage loss. Severe epistaxis may require additional management such as nasal packing. The presence of clear rhinorrhea necessitates further evaluation for a cerebrospinal fluid leak, such as with a beta-2 transferrin assay and high-resolution facial computed tomography (CT) scan to assess for a skull base fracture.
A complete physical examination must include investigation for physical signs of other facial bone fractures. A thorough examination of the head and neck should include palpation of the entire facial skeleton, assessment of extraocular motility, visual acuity, facial movements and sensation, and thorough evaluation for dental injury or pain, trismus, and malocclusion. The presence of any of these associated injuries should prompt further investigation with imaging.
Radiological Evaluation
Isolated nasal fractures are primarily diagnosed through history and physical examination; therefore, the role of radiology in the diagnosis and management of nasal bone fractures is controversial. Plain radiographs are not helpful in the management of routine nasal bone fractures and should not be ordered. Plain films are unable to distinguish between acute and old fractures and there is often poor correlation between the radiological findings and the presence of external deformity.
Facial CT has been shown to demonstrate superior diagnostic accuracy when compared to conventional radiography in the detection of nasal bone fractures. In a review of 503 cases, only 82% of nasal bone fractures were correctly identified by plain films taken in both lateral and Waters views versus 100% by facial CT. Despite the high positive predictive value of CT in detecting nasal bone fractures, the presence of a nasal bone fracture on CT scan has not been shown to reliably predict the need for surgical management. The use of a CT, however, does document the direction and degree of bone and septal displacement.
Although CT is described as the gold standard modality of imaging for nasal bone fractures, some studies have suggested that high-resolution ultrasonography is as sensitive and specific, and may be particularly beneficial in pregnant women and children due to its absence of ionizing radiation. However, the main disadvantage of ultrasonography is that it is operator-dependent.
Imaging, in general, may be beneficial in cases with equivocal physical exam findings or suspected associated injuries such as naso-orbito-ethmoid (NOE), orbital, and/or zygomaticomaxillary complex (ZMC) fractures. However, experienced clinical assessment remains the gold standard in determining the need for surgery.
Classification
Most clinical classification schemes are based on the degree and direction of force suspected to result in nasal injuries. Nasal fractures can be broadly divided into two types: those that result from a lateral blow and those that result from frontal impact. Lateral impact injuries are more common than frontal injuries, as greater force is typically required to cause the latter.
The lateral force fracture may range from a slight depression of a unilateral nasal bone to full lateral deviation of the nasal bridge due to bilateral nasal bone fractures (medial displacement of the ipsilateral nasal bone and lateral displacement of the contralateral nasal bone) with or without accompanying septal fracture. Disruption of the keystone region is less common. Treatment tends to be relatively simple, requiring centralization of the deviated nasal bones and septum.
According to Stranc and Robertson, frontal impact injuries can be divided into three categories depending on the depth of the injury in the coronal plane. Plane 1 injuries do not extend a line joining the lower end of the nasal bones to the anterior nasal spine. The force is predominantly transmitted to the cartilaginous framework and the inferior tip of the nasal bones, leading to deviations in the nasal septum and injury to the upper lateral cartilages while the nasal bones remain largely central. Plane 2 injuries are more extensive but still limited to the nose. Flattening or splaying apart of the nasal bones as well as mucoperichondrial tears, more extensive overriding fractures of the septum, and loss of central support can be seen. Plane 3 injuries are essentially NOE fractures; increased comminution of the nasal bones with fracture extension into adjacent bony structures is seen. Injuries to the nasal septum are often severe, with associated telescoping of septal fragments and structural collapse.
Murray et al. describe an alternate classification scheme based on seven pathological types of fractures that resulted when various weights were dropped on cadavers’ noses. Their study demonstrates that nasal fracture patterns are not consistently predicted by the amount and vector of the applied force. This system emphasizes that if the nose is deviated more than one-half its width from the midline, then the bony septum is involved; therefore, mere manipulation of the nasal bones alone will likely lead to recurrent deformation and need for secondary reconstruction.
Many other clinical classification schemes have since been proposed, most of which attempt to categorize trauma based on the extent of injury to the nasal bones and septum: simple vs. comminuted, unilateral vs. bilateral, degree of deviation, and degree of septal injury. Most emphasize the importance of adequate septal repair in optimizing nasal fracture management and in minimizing the need for secondary surgery.
Surgical Indications
Surgical intervention following nasal trauma is warranted only if there is a change to the appearance and/or function of the nose after injury. Nasal fracture repair is typically elective, and may be deferred based on patient preference or condition.
Pediatric nasal trauma warrants special consideration. The pediatric nasal skeleton is more cartilaginous and flexible, and less prone to bony comminution. However, the pediatric nasal septum – which plays a crucial role as a growth center for nose and midface – is more vulnerable to injury. In general, conservative treatment of nasal fractures in the pediatric population is recommended, with close observation and closed treatment of fractures as the mainstay. Although many surgeons favor delaying septoplasty and open reduction methods until after the adolescent growth spurt, early intervention may be indicated if there is severe nasal airway obstruction or external deformity that may result in adverse facial growth and/or problems with sleep disturbance and quality of life.
Surgical Techniques
Timing of Repair
The timing of nasal fracture repair is dependent on the degree of injury and the amount of associated soft tissue edema. In the uncommon circumstance that a patient presents with an acute fracture within hours of injury with minimal associated edema, immediate fracture reduction might be performed. More typically, patients present with significant edema that obscures underlying nasal landmarks. In these instances, patients should be reassessed 3–5 days later after severe swelling subsides to determine need for reduction.
Fracture reduction is ideally performed 1–2 weeks following the injury, in order to obtain maximal accuracy and stability. Pediatric patients should be managed within 7–10 days given their tendency to heal more rapidly. After about 2–3 weeks it becomes more difficult to manipulate the healing nasal bones, although some report successful outcomes with manipulation up to 5 weeks following injury, particularly in patients with thinner bones or more comminuted fractures.
Considerations for Anesthesia
The use of local versus general anesthesia for acute nasal bone fracture reduction is somewhat controversial. Benefits of local anesthesia include avoidance of the risks of general anesthesia and decreased associated costs and resources. General anesthesia is particularly advantageous in children and less cooperative or anxious adults, and for fractures that may require more extensive or open manipulation. However, the timing of treatment is often dependent on operating room and personnel availability.
A number of studies have compared the outcomes of local versus general anesthesia for the closed treatment of nasal fractures. Current literature suggests that 79–90% of patients are satisfied after closed manipulation overall. Several studies demonstrate equivalent functional and cosmetic results from both patient and surgeon perspectives as well as equivalent reoperation rates after closed reduction. However, at least one study demonstrates higher rates of reoperation with septoplasty, septorhinoplasty, or rhinoplasty in patients treated under local anesthesia (17%) versus general anesthesia (3%). A recent systematic review with meta-analysis of the limited literature suggests that although there is a trend towards better outcomes with general anesthesia, there are no significant differences between anesthesia modalities for nasal airway outcome, anesthetic experience, or number of revision procedures.
The literature is relatively inconclusive and considerations for anesthesia are ultimately dependent on surgeon and patient preferences. It is the authors’ preference to perform surgical intervention in an ambulatory surgical center under brief general anesthesia as it optimizes airway control and allows for unhindered nasal examination and more accurate and complete manipulation.
Local anesthesia, in either setting, may be provided by both topical and infiltrative agents. A 1 : 1 mixture of 4% topical lidocaine and oxymetazoline can be applied intranasally via pledgets for mucosal decongestion, vasoconstriction, and topical anesthesia. Infiltrative anesthesia with 1% lidocaine with 1 : 100,000 epinephrine can be administered both externally and internally. Infiltrative blocks can also be applied to the infraorbital and dorsal nasal nerves although generalized infiltration of the external dorsum has been found to be significantly less painful for patients.
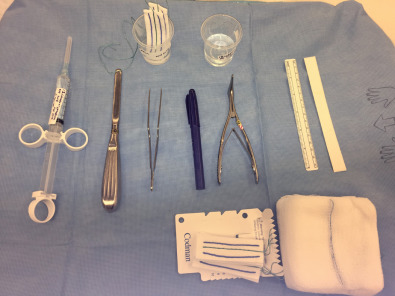
The operative set-up is shown in Fig. 1.10.2 .
Related posts:
 Assessment of the Patient With Traumatic Facial Injury
Assessment of the Patient With Traumatic Facial Injury
 Frontal Bone and Frontal Sinus Injuries
Frontal Bone and Frontal Sinus Injuries
 Le Fort Fractures
Le Fort Fractures
 Secondary Reconstruction of Facial Soft Tissue Injury and Defects
Secondary Reconstruction of Facial Soft Tissue Injury and Defects
 Geriatric and Edentulous Maxillary and Mandibular Fractures
Geriatric and Edentulous Maxillary and Mandibular Fractures
 Secondary Microvascular Reconstruction of the Traumatic Facial Injury
Secondary Microvascular Reconstruction of the Traumatic Facial Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


