Preservation rhinoplasty has been a trending topic in the rhinoplasty literature. There is no single technique that can correct all structures; therefore, patient analysis is paramount. This article focuses on the anatomy of the keystone area and the dynamics of the dorsum explained through the biotensegrity concept. Differences between push-down and let-down techniques are addressed from a nasal valve physiology point of view. The let-down technique maintains the tensegrity of the nasal pyramid. Preservation should be preferred, in most cases, over resection, as well as reposition over manipulation.
Key points
- •
The keystone area is the osseocartilaginous structure formed by the nasal bones and the upper lateral cartilages that constitutes a nonrigid structure beneath the nasal dorsum.
- •
The nasal dorsum is one that has rigid struts that bear tension and compression and a structure forms by the upper lateral cartilages that bear prestress.
- •
The differences between push-down and let-down maneuvers are how they can affect the nasal valve and hump removal.
- •
The push-down technique pushes the bones inside the nasal cavity, whereas the let-down technique preserves the nasal cavity area and the nasal valve.
Introduction
Management of the dorsum has always been a challenge in rhinoplasty. In most Caucasian noses, and even for those considered mestizo noses, reduction of the dorsum implies the resection of bone and cartilage, with the resulting disruption of the keystone area and the cartilages, requiring the placement of spreader grafts.
Experience with rhinoplasty over time has shown that detailed anatomic analysis of the nose is an essential first step in achieving a successful outcome. Failure to recognize a particular anatomic feature preoperatively will often lead to a less than ideal long-term result.
The analysis of a patient undergoing nasal surgery should not only be of the nose; it is important to consider race, perform an integral facial analysis, and determine the positive and negative facial characteristics to adequately diagnose the condition and take into account the technique to be used, which in addition to correcting the main problem, will give additional contributions to optimize the results.
In addition to considering the anatomic and functional concepts, the nose should be viewed as a comprehensive structure both functionally and aesthetically. It is important to consider that the concepts of form and function must not be separated; an esthetically pleasant nose is most likely to have an adequate functional state.
Anatomic and dynamic considerations of the nasal dorsum
Approaching the nasal dorsum, in particular, has become a very precise maneuver that requires a comprehensive knowledge of the anatomy as well as a properly trained surgeon to minimize complications.
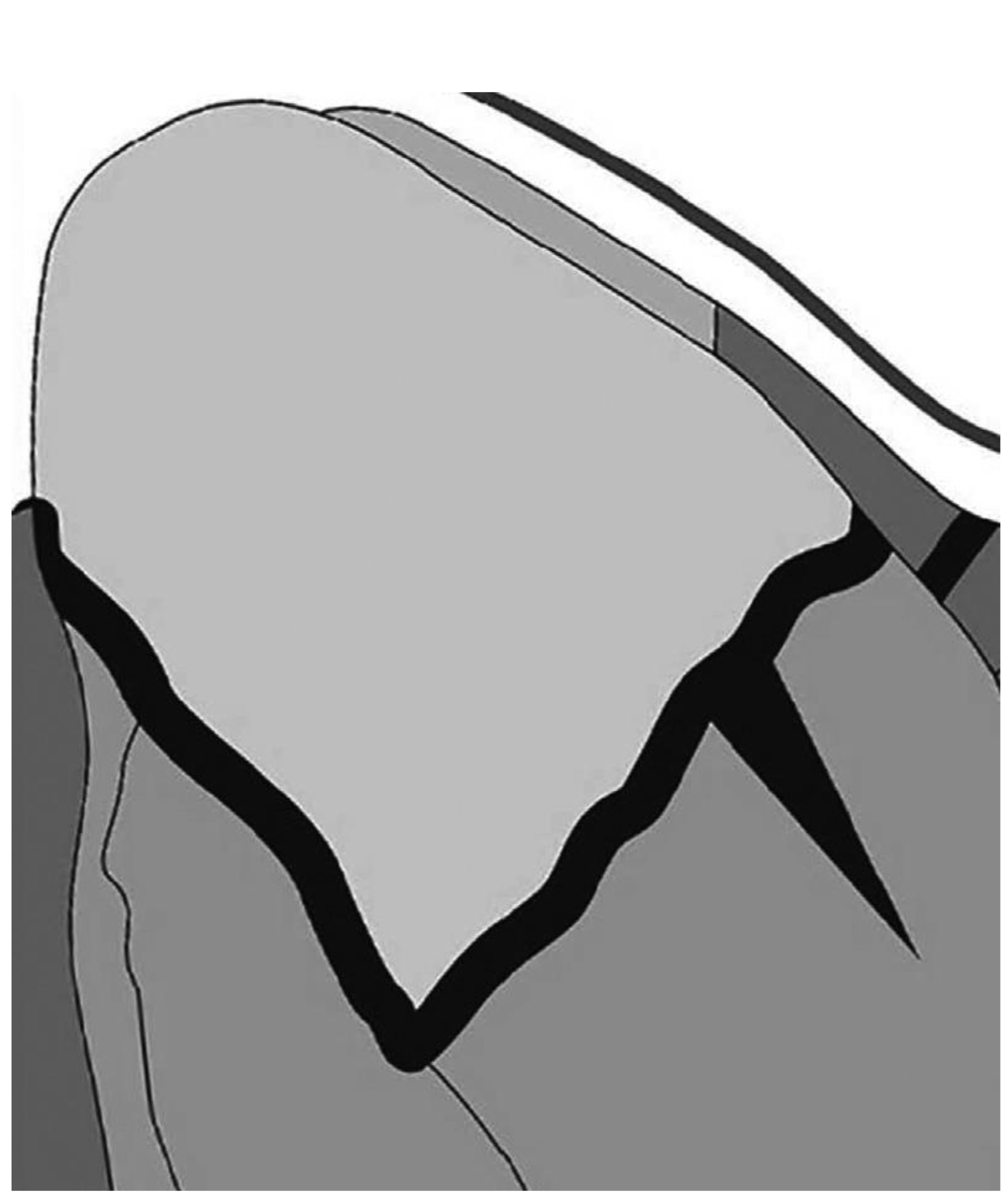
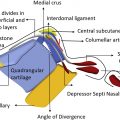
To better understand the complexity of the dorsal structure of the nose, one must start by understanding the anatomy of the K-area. It is an osseocartilaginous structure formed by the nasal bones, the upper lateral cartilages, and the nasal septum beneath. Theses structures are not rigidly fused, they are joined together by a chondro-osseous joint.
There is a portion of the cartilaginous septum that extends high cephalically to the K-area and almost no bony septum along this area, leaving the support of the bony cap to the quadrangular septum at his ventral portion and at the joint with the perpendicular plate of the ethmoid ( Fig. 1 ). Taking this anatomic feature into consideration, one can understand that the nasal valve, a dynamic structure claimed to be the primary inflow regulator of air to the nose, can be affected by a rhinologic surgery aimed to modify the dorsum. In fact, it is claimed to be the second most common cause of nasal valve abnormalities only after anterior deviation of the septum.
Many investigators have pointed out the differences between push-down and let-down maneuvers with regards to how they can affect the nasal valve, as well as comparisons to hump removal. The only study to date measuring the effect of the 3 techniques on the nasal valve is that of Most and colleagues where they conclude after computed tomography measurements, that hump removal and let-down techniques do not impact the physiology of the nasal valve, whereas the push-down techniques does.
The biotensegrity concept applied to the nasal dorsum
In 1998, Dr Donald E. Ingber described that tensegrity structures are mechanically stable not because of the strength of individual members, but because of the way the entire structure distributes and balances mechanical stress. He emphasizes that there are 2 categories of structures: one is basically a framework made up of rigid struts that can bear compression or tension, and another stabilizes itself through a phenomenon known as prestress. These counteracting forces equilibrate throughout the structure, enabling it to stabilize itself. Furthermore, as has been described by Dyer, nasal tip support is a spring-loaded structure. He states that the difficulty of performing nasal tip surgery is the complex mechanism of support and the fact that surgeons are not used to think as engineers or architects while doing surgery in complex structures.
The structure of the nasal dorsum is one that has rigid struts that bear tension and compression (nasal bones) and a structure forms by the upper lateral cartilages that bear prestress, the 2 categories previously described, and they should be addressed separately during surgery. The 2 most common procedures performed in the nasal dorsum, hump removal and preservative surgery, should be analyzed regarding the anatomy and the dynamics of the structure that are to be modified. Although in hump removal the cartilaginous dorsum and the bony dorsum are addressed separately, the integrity of the two is compromised because the cap of bone is removed, and the structure formed by the upper lateral cartilages and the septum is removed and reconstructed, affecting the function of the nasal bones as struts, and the resistance of the nasal valve.
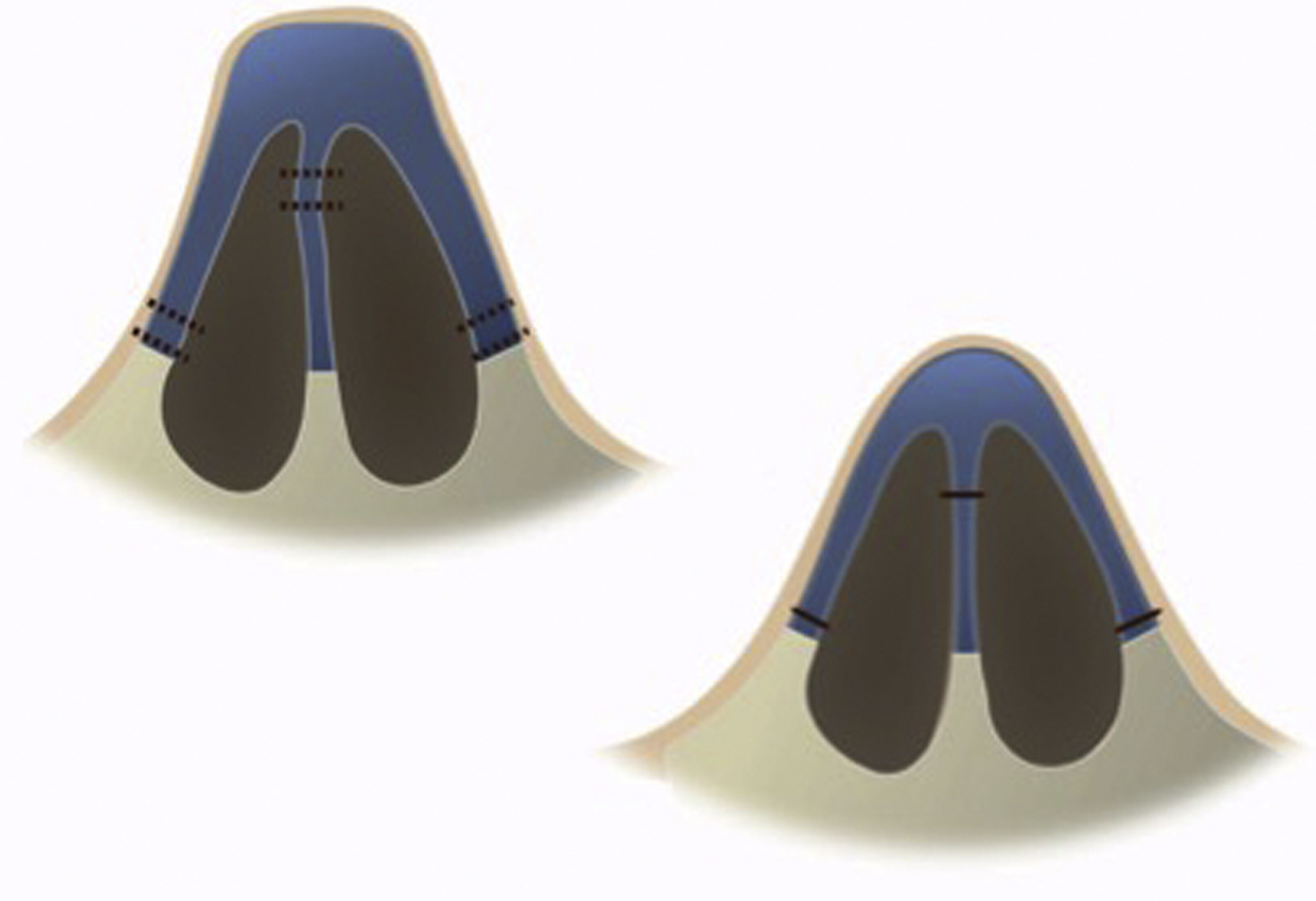
With the preservation technique, more precisely, with the let-down technique, the principle is to remove a portion of the cartilaginous septum below the Keystone area and of the nasal bones crating a gap that will be closed by letting the whole structure to come down preserving the support both internally and externally, while the cartilaginous dorsum suffers no disruption because the septum is repositioned at the nasal spine ( Fig. 2 ).
Surgical technique
Dorsal preservation techniques are especially indicated in the following noses:
- 1.
The straight nose with a moderate kyphotic hump.
- 2.
The deviated nose with high dorsum.
- 3.
The tension nose that often has elongated vertical nostrils and narrow internal nasal valves that tend to collapse.
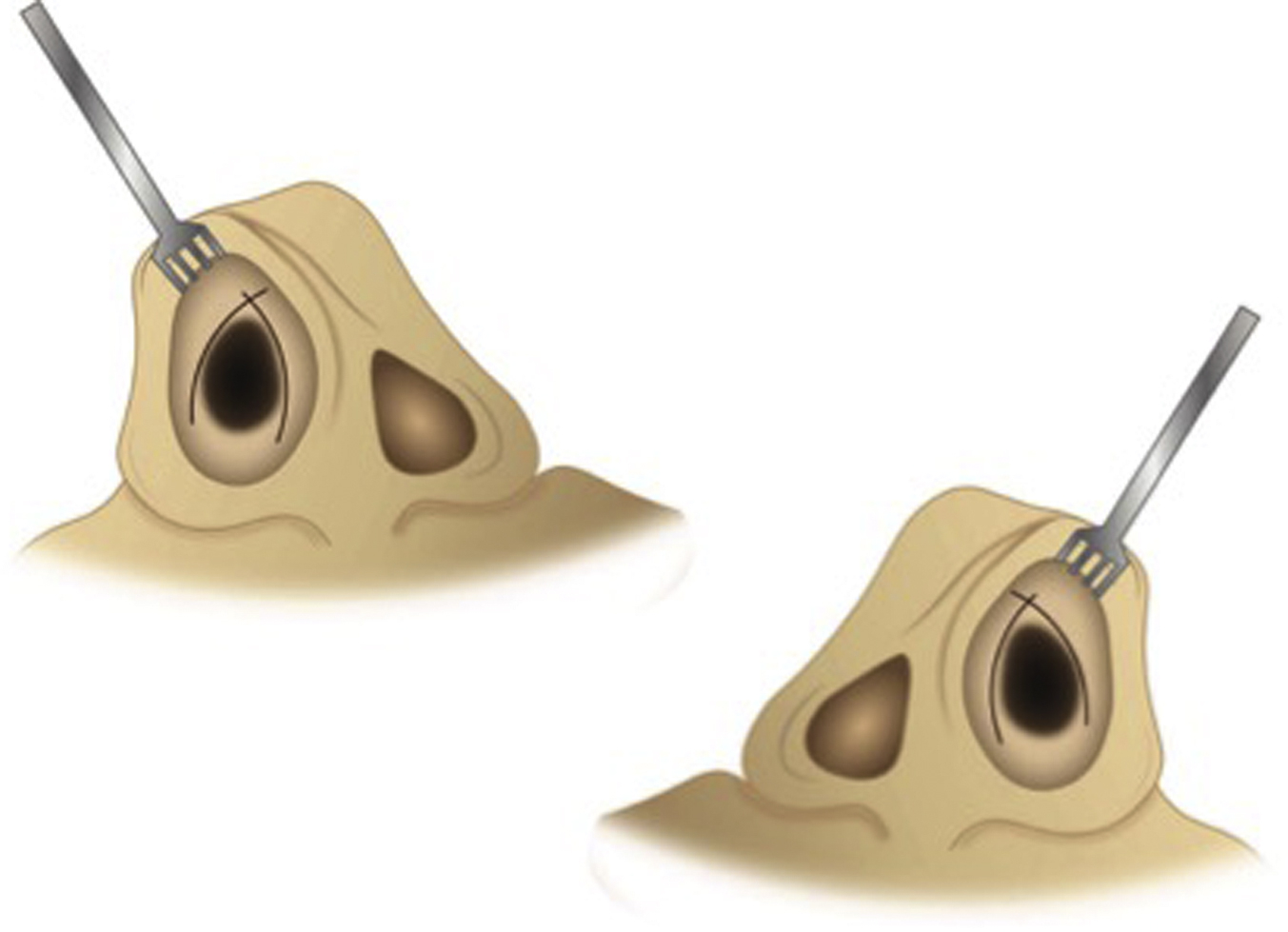
The area is infiltrated with 3 to 5 mL of lidocaine 2% + epinephrine (1:100,000), in the conventional areas (nerves: external nasal, infraorbital, supratrochlear, supraorbital and nasopalatine) as well as the intercartilaginous (IC) area, cul-de-sac, and the transition from columellar skin to nasal mucosa. The caudal border of the upper lateral cartilage is identified and its scroll, with the help of a 4-prong retractor, and the application of digital pressure upon the lateral crus of the inferior lateral cartilage, to identify the cephalic border. A simple skin hook is placed in the cul-de-sac, applying medial traction to give the appropriate tension to the tissues, and perform its dissection. A left IC incision is made, followed by a hemitransfixion incision, and the incisions are replicated on the right side. The IC incision is situated on a horizontal plane, having first located the site where the caudal border of the upper lateral cartilage and the cephalic border of the inferior lateral cartilage where they meet. The IC incision of the skin is performed from a lateral to medial direction, beginning on the external border of the upper lateral cartilage, and upon reaching the cul-de-sac, the scalpel is inserted by applying pressure toward the nasal midline, with 2 objectives: deepening the incision so as to reach the dorsal cartilaginous plane and avoid the risk of continuing to cut and injuring the skin of the columella, maintaining absolute control of the length of the IC incision.
The hemitransfixion incision is performed from below upward, joining both incisions (hemitransfixion and IC) in a T-shaped incision ( Fig. 3 ). The same procedure is performed on the right side.
Related posts:
 Preservation Rhinoplasty
Preservation Rhinoplasty
 Incorporating Dorsal Preservation Rhinoplasty into Your Practice
Incorporating Dorsal Preservation Rhinoplasty into Your Practice
 Key Points in Subperichondrial-Subperiosteal Dissection
Key Points in Subperichondrial-Subperiosteal Dissection
 Dorsal Preservation Rhinoplasty
Dorsal Preservation Rhinoplasty
 Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
 Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


