INTRODUCTION
Venous disease encompasses a wide spectrum of clinical manifestations, from asymptomatic spider veins on the legs to intermittently bulging branches of the greater saphenous vein extending across the knee to dull achy pain in the posterior calf after prolonged standing. The science of treating venous disease, phlebology, has roots dating to the ancient Greeks in 400 BCE, at which time venous disease was recognized as undesirable and unsightly. Procedures involving the use of instrumentation to traumatize veins were described by Hippocrates in the fourth century BCE, and procedures such as vein stripping were routinely practiced in the years to follow.
In modern days, diagnosing and treating venous disease still presents a formidable challenge. Venous insufficiency, which is caused by valvular incompetence in the deep or superficial venous system, is the most common form of venous disease. Venous disease affects 40% to 55% of the population, with the common symptoms of leg pain, swelling, and skin changes. Superficial venous insufficiency occurs when a high-pressure leakage develops between the deep and superficial systems or within the superficial system itself, followed by sequential failure of the venous valves in superficial veins. The two major divisions of the superficial system are the great saphenous vein (GSV) and the small saphenous vein (SSV). Venous insufficiency in this system allows venous blood to escape from its normal flow path to flow in a retrograde fashion down an already-congested leg. Over time, incompetent superficial veins acquire the typical dilated and tortuous appearance of varicosities. Furthermore, insufficiency can lead to chronic morbidity in the form of ulcerative and edematous skin changes in the lower extremities.
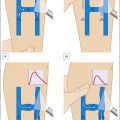
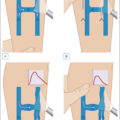
Further “downstream,” changes involving the smaller branching vessels, such as unsightly or symptomatic venulectasias and/or telangiectasias, are major consequences of superficial venous valvular insufficiency. To optimize the treatment of varicosities and telangiectasias, pattern recognition of common clinical manifestations is highly recommended. For a regional consideration of the anatomy that gives rise to varices, it is helpful to divide the thigh and calf into four quadrants: lateral, medial, anterior, and posterior ( Figs. 2.1 and 2.2 ). A regional approach can lead to some unavoidable repetition because many veins extend through many regions or have tributaries that cross many boundaries. Clinical photographs accompanied by simplified diagrams are helpful for identifying the root causes of an unfamiliar pattern of reflux. An understanding of normal venous anatomy is essential for a thorough understanding of venous disease ( Figs. 2.3 and 2.4 ). Knowledge of the location of the major perforator veins, which connect the deep venous system to the superficial system, is also important for determining the etiology of patterns of varicosities ( Fig. 2.5 ).
Thigh compartments. GSV , Great saphenous vein; LSVS , lateral subdermic venous system; PTPV , posterior lateral thigh perforating vein.
Calf compartments. GSV , Great saphenous vein; LSVS , lateral subdermic venous system; SSV , small saphenous vein.
Anterior view of the leg, showing the great saphenous vein and its major branches.
Posterior view of the leg showing the small saphenous vein and its major branches.
Clinically important perforating veins in the lower extremities.
TREATMENT APPROACH
It is best to approach the clinical examination of venous disease by visualizing the lower extremities while the patient is in the standing position from superior to inferior, starting from the upper thigh to the calf and concluding with the ankle. Above and below the knee, a division of four compartments can be made in the anterior and posterior planes. When considering the thigh, the presence of reflux in the GSV can manifest in the appearance of varicosities in the medial thigh compartment ( Box 2.1 ).
Box 2.1
Thigh Quadrants
| Medial thigh | |
| Incompetent saphenofemoral junction | Hidden reflux at saphenofemoral junction (only palpable on standing) |
| Superficial axial branch veins (medial tributaries) of GSV | Resistant telangiectatic matting (just above knee) due to GSV reflux |
| Distal saccular saphenous vein dilation (just above knee) | |
| Pudendal vein | Mid-thigh perforators |
| Posterior thigh | |
| Superficial gluteal | S-shaped reticular vein of the posterior thigh |
| Posterior thigh perforators emptying into LSVS | S-shaped reticular vein of the posterior thigh |
| Vein of Giacomini | |
| Lateral thigh | |
| Lateral subdermic venous system (Albanese)—most common cosmetic pattern | Anterolateral tributary of the GSV |
| Branch varicosity of small saphenous vein | |
| Anterior thigh | |
| Anterolateral tributary of GSV | |
| Inguinal fold reticulars | Incompetent saphenofemoral junction |
| Superficial axial branch veins (lateral tributaries) of GSV | Small anterior branches of the LSVS |
| Patellar | |
GSV , Great saphenous vein; LSVS , lateral subdermic venous system.
Pudendal veins are 3- to 4 mm blue reticular varicosities that can be seen extending from the external genitalia. These indicate reflux in the pudendal tributary of the GSV, and when they become engorged, as may happen during sexual activity or menses, pain can occur. Treatment of these varicosities by sclerotherapy is easily accomplished in the absence of saphenofemoral junction incompetence.
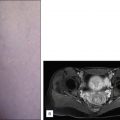
Because the GSV typically lies deep and is surrounded by fascial layers, it may be difficult to clinically appreciate the prominence that accompanies reflux in this anatomic compartment. In the case of saphenofemoral junction reflux, duplex ultrasound (DUS) is usually necessary to confirm the reflux. Prolonged standing may facilitate visualization of the GSV ( Fig. 2.6 ). As the GSV courses distally, superficial tributaries can become varicose as they accept reflux from above and below. In the most distal aspect of the thigh medially, just above the knee, the GSV can emerge from the fascial layers and may become apparent as an enlarged bulbous segment ( Fig. 2.7 ). Clinical manifestations of a refluxing GSV can vary based on the degree of reflux and branch involvement ( Fig. 2.8 ).