Premaxillary Segment Setback
Omri Emodi
DEFINITION
Orofacial clefts (OFCs) are the most common birth defect with a prevalence of 17 in every 10 000 live births.1
OFCs are most common in Amerindian and Asian populations (15-36/10 000) and least common among African populations (5/10 000).2,3
OFCs involving the lip have a male-to-female ratio of 2:1.
Bilateral cleft lip and palate (BLCP) is the most severe of the common OFC subtypes and represents 1 in 10 patients with clefts of the lip.
Subjects with BCLP usually present with maxillary retrognathism, a smaller mandible with an obtuse gonial angle, greater anterior upper and lower facial heights, and retroclined maxillary incisors.
The premaxilla associated with BCLP may present in multiple positions, including severe protrusion (FIG 1).
ANATOMY
The nasomaxillary process (including the nose and premaxilla) is separated from the lateral maxillary segments.
There is significant variation in the position of the premaxilla in patients with BCLP.4
It may be in correct position in relation to the lateral maxillary segments.
The premaxilla may also project anteriorly or rotate up under the nose, with significant deviation to either side.
Severe protrusion of the premaxilla is possible.

FIG 1 • A child with protruded premaxilla.
The prolabium (soft tissue on the premaxilla) is composed of skin, subcutaneous tissue, and fat and is without a muscle layer.
Vascular and neural findings include the following:
The pterygopalatine portion of the maxillary artery provides major branches to the maxilla, teeth, palate, and linings of the nose and sinuses.
The posterior septal artery alone cannot fully meet the needs of the premaxilla and requires a complementary supply from the prolabial circulation (FIG 2).
PATHOGENESIS
The embryological development of the upper lip and nose requires a sequence of complex, genetically programmed events:
Fusion of the five major facial prominences occurs between the 3rd and 8th weeks of gestation.
Lip development occurs between the 3rd and 7th weeks.
PATIENT HISTORY AND PHYSICAL FINDINGS
BLCP patients with protrusive premaxillae may present at several time points where treatment can be initiated.
Prior to lip repair, presurgical orthodontics may be used to retrocline the premaxilla.5
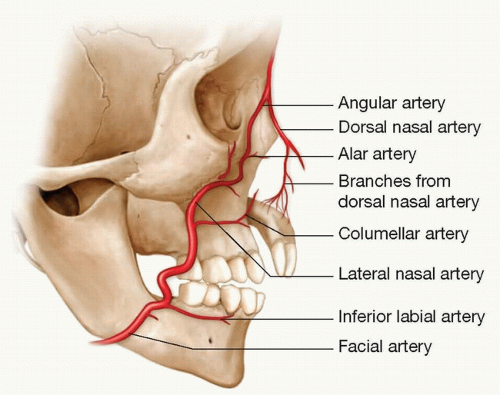
FIG 2 • Anatomical description of the blood supply to the premaxilla in patients with bilateral cleft lip and palate. Branches from the dorsal nasal artery and the columellar artery contribute to the blood supply of the premaxilla.
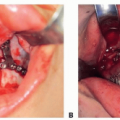
After lip repair, when the patient may require surgical setback of the premaxilla as an isolated procedure.
During mixed dentition (6-8 years of age), when the premaxillary setback can be performed with a bone grafting procedure.6Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree