Posterior Fusion for Idiopathic Scoliosis
Craig M. Birch
Operative Indications
Primary indication: Progressive thoracic curve greater than 50° or thoracolumbar/lumbar curve greater than 40°
Pain is not an indication for surgical intervention without further evaluation and treatment related to pain
Preoperative Imaging
Typical adolescent idiopathic curve pattern is right thoracic with left lumbar and potential left upper thoracic curve (Figure 3.1)
Typical curves: Right thoracic, left lumbar
Preoperative imaging should consist of standing posteroanterior (PA) and lateral full spine radiographs or EOS imaging
Right and left bending films to adequately determine flexibility and Lenke criteria (Figure 3.2)
Atypical curves: Left thoracic, kyphosis, severe coronal decompensation
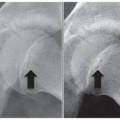
Additional preoperative imaging is required and should include magnetic resonance imaging (MRI) of the entire spine to evaluate for neurologic anomaly, specifically tethered spinal cord, Chiari malformation, and syrinx (Figure 3.3)
Computed tomography (CT) is typically not used unless preoperative templating is required for navigation or for robotic assisted surgery
Equipment
Jackson frame
Spinal instrumentation set of choice with standard selection pedicle screws, hooks, sublaminar bands or wires, and rods
Standard spine kit consisting of retractors, Cobb elevators, curettes, rongeurs, Capener gouges, osteotomes, and Penfields
Imaging modalities of choice including C-arm fluoroscopy and/or O-arm
Optional additional equipment
Aquamantys tissue sealant
Bone scalpel
Navigation equipment with navigation statin
Robotic system
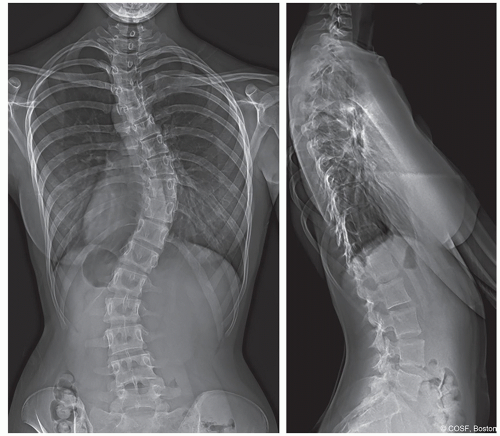 Figure 3-1 ▪ Posteroanterior (PA) and lateral radiographs of a typical curve pattern with right thoracic and left lumbar curves. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Positioning
Patient is intubated with bite block, orogastric (OG) tube, arterial line, and multiple large bore intravenous access established per anesthesia protocol. Foley is placed for urinary output measurement. Neuromonitoring leads attached for motor evoked potentials (MEPs), somatosensory evoked potentials (SSEPs), and electromyography (EMG)
Patient is flipped prone on the Jackson frame
Neck position should be checked to ensure in a neutral position. No additional flexion or extension
Arms positioned with shoulders abducted to 90°, elbows flexed to 90°, and wrists in neutral position
Arms padded with no pressure on the ulnar nerve
Back is then widely draped with 1000 drapes
Most surgeons have preferred prescrub of either alcohol followed by hydrogen peroxide or chlorhexidine which should include the periphery of the 1000 drapes
Wide prep consisting of chlorhexidine unless allergic and then Betadine. Border of the 1000 drapes should be included in both the prescrub and the prep
Spinous processes are then palpated, typically counting from most prominent C7 down to anticipate levels of fusion. Incision is drawn based on palpated landmarks. Ioban sticky drape is laid directly onto skin as last step
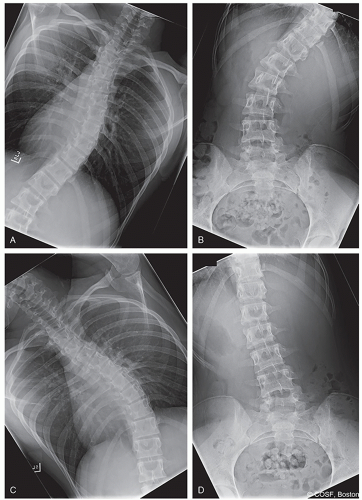 Figure 3-2 ▪ A-D, Right (A, B) and left (C, D) bending films to assess the flexibility of upper thoracic, main thoracic, and lumbar curves. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Surgical Approach
Posterior Exposure
Incision over the spinous processes of anticipated levels of fusion
Some surgeons scratch the skin followed by dilute epinephrine injection into the skin and subcutaneous tissue followed by sharp dissection down to the level of the posterior fascia. Others prefer incision to dermis and immediate use of electrocautery dissection down to posterior fascia. Effort should be made to minimize soft tissue dissection to avoid creating large dead space
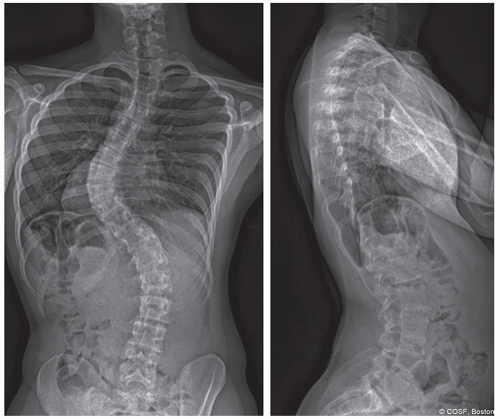 Figure 3-3 ▪ Posteroanterior (PA) and lateral radiographs showing an atypical curve pattern, here a left thoracic curve. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Bony Dissection (Figure 3.4)
Spinous processes are identified and split using electrocautery
Cobb and electrocautery dissection down the spinous processes to lamina and then out to the transverse process
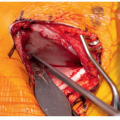
Interspinous ligament of the most cephalad level should be left intact. The fascia should be split off to each side so as to not disrupt the ligamentous attachment (Figure 3.5)
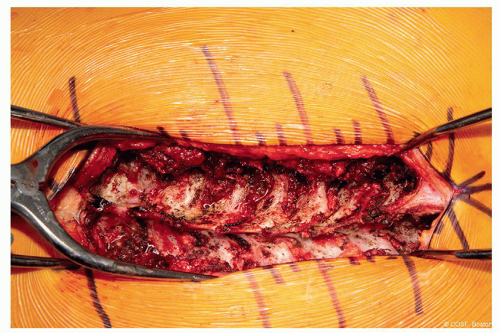 Figure 3-4 ▪ Intraoperative image after subperiosteal dissection and bony exposure. Caudal to the left, cranial to the right. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
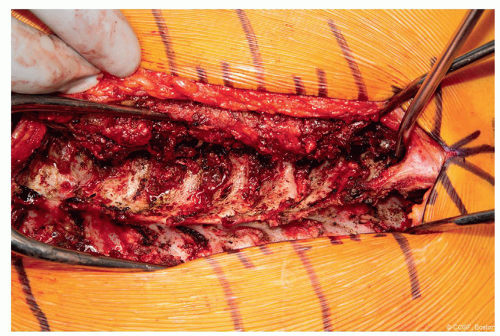 Figure 3-5 ▪ Intraoperative image highlighting the fascial split at the cranial aspect of the exposure. Suction tip located in the apex of the fascial incision. This allows the interspinous ligament to be kept intact at the cranial most level. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Technique in Steps
Facetectomy (Figure 3.6)
Facet joints are identified, and the capsule is removed using Cobb and electrocautery
Capener gauge or bone scalpel is used to remove the inferior articular facet exposing the underlying cartilage of the superior articular facet of the distal vertebral body
Facet joints will be more overlapped, and bone will be more dense on the concavity
Capener, curette, or burr is used to remove the articular cartilage
Screw Placement
Starting point is selected using anatomic landmarks (Figure 3.7)
Burr is used to make starting hole for screw starting pointRelated posts:
 Surgical Decision-Making in Pediatric Hand and Arm
Surgical Decision-Making in Pediatric Hand and Arm
 Decision-Making in Pediatric and Adolescent Hip Disorders
Decision-Making in Pediatric and Adolescent Hip Disorders
 Clubfoot Casting and Heel Cord Lengthening
Clubfoot Casting and Heel Cord Lengthening
 Radioulnar Synostosis Derotation Osteotomy
Radioulnar Synostosis Derotation Osteotomy
 Neuromuscular Hip Surgery: Prevention to Reconstruction
Neuromuscular Hip Surgery: Prevention to Reconstruction
 Minimally Invasive Techniques for Foot Deformity Correction
Minimally Invasive Techniques for Foot Deformity Correction

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


