Revision breast augmentation to treat implant malposition is fraught with challenges. This article focuses on treatment of implant malposition by using acellular dermal matrices (ADMs) with the intent of creating more reliable and accurate results. The article discusses the use of ADMs in patients with breast implant complications such as bottoming out, lateral implant displacement, or synmastia. ADM is a foreign material, thereby adding potential complications to consider.
In 2010, close to 300,000 breast augmentations were performed in the United States, making this the most commonly performed cosmetic surgery. By virtue of the sheer numbers of annual breast augmentations performed, a large market for revisionary augmentation procedures exists. The two most frequently encountered complications of primary breast augmentation are capsular contracture and implant malposition. This article focuses on treatment of implant malposition, excluding capsular contracture, by using acellular dermal matrices (ADMs).
- 1.
The two most frequently encountered complications of primary breast augmentation are capsular contracture and implant malposition.
- 2.
Each successive surgical revision is incrementally more challenging, thus each revision attempt must be planned thoroughly; understanding the anatomy of the primary augmentation failure is essential to properly diagnose and treat the unsatisfactory outcome.
- 3.
Treatment of breast implant malposition depends largely on the patient’s anatomy, presenting complaints, desired outcome, and anatomic limitations.
Implant malposition may occur in any one (or a combination) of the four breast quadrants.
- 1.
Superior
- 2.
Medial
- 3.
Inferior
- 4.
Lateral.
Superior displacement (high-riding implants) may result from inadequate pocket creation, insufficient release of the pectoralis major muscle, or secondarily as a presentation of capsular contracture ( Fig. 1 A).
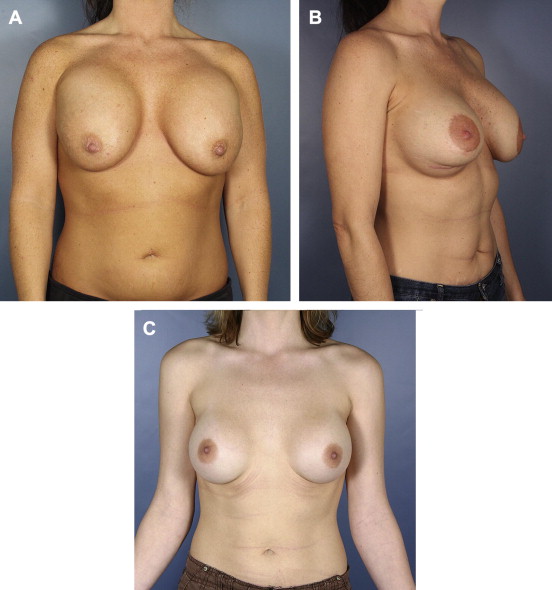
Medial displacement (synmastia) is almost always an iatrogenic consequence resulting from overdissection of the pocket or selection of implants that are too large.
Inferior displacement (bottoming out) is the most common malposition and presents as an elongation between the nipple areolar complex (NAC) and neoinframammary fold. This malposition may lead to stretching of the inferior breast pole skin, compromise of the integrity of the inframammary fold (IMF) structure, or a combination of the two (see Fig. 1 B).
Lateral displacement of the implant is, to some degree, normal with submuscular implants, but excessive lateralization (telemastia) can create a wide separation between breasts (see Fig. 1 C). Each of these deformities needs to be understood anatomically to institute proper revisionary surgery.
Anatomic considerations of secondary breast augmentation
Many challenges face the plastic surgeon when considering revisionary augmentation mammaplasty. Patient dissatisfaction with the result of the initial procedure and secondary procedures creates unexpected costs and stress for patients who expected acceptable results with a single procedure. Each successive revision is incrementally more challenging, therefore it is crucial that each attempt at revision is done with as much forethought and planning as possible.
It is important to fully understand the anatomy of the primary augmentation failure to properly diagnose and treat the unsatisfactory outcome. Considerations include ( Table 1 ):
- •
Nipple to sternal notch distance
- •
NAC to IMF distance
- •
Location of the current and original IMF
- •
Breast base width
- •
Potential presence of capsular contracture
- •
Plane location of the implants
- •
Approach location.
| Measurement | Normal Dimension | Abnormality |
|---|---|---|
| Nipple to sternal notch | 17–20 cm | Too long indicates the need for superior repositioning of the NAC |
| NAC to IMF | 4–6 cm | Too long indicates the need for a mastopexy to reduce the bottom pole skin or repositioning of the IMF superiorly (for double-bubble deformity) |
| Location of IMF | Sixth rib | Too low indicates need to reposition the IMF |
| Base width | Variable | Assists with the selection of implants |
The following characteristics of the implants should be evaluated:
- •
Volume
- •
Surface texture
- •
Shape
- •
Type of implants.
When considering revision surgery, it is good practice to review the prior operative reports to learn as much as possible about the initial augmentation (or previous revisions) before undertaking further procedures.
Prevention of deformity following primary augmentation
Before discussing treatment options and strategy for revision breast augmentation, it is important to understand how to prevent the unsatisfactory result. There are important anatomic considerations that the plastic surgeon must recognize and carefully manage during primary augmentation:
- •
Short NAC to IMF distance. In cases in which there is insufficient inferior breast pole skin, it is important to educate patients about the limitations this anatomic variation presents ( Fig. 2 A). After augmentation, the inferior pole expands, although it is typically not sufficient for the nipple to be positioned at the midportion of the breast mound. High-profile implants place the point of maximum projection lower on the breast and create more projection for the relative volume. It does this at the expense of sacrificing medial and upper pole fullness, although the trade-off usually leads to a better aesthetic result. Selection of modest-size implants is wise in these challenging cases, and although some surgeons are comfortable with lowering the IMF surgically, I find it perilous (see Fig. 2 B).
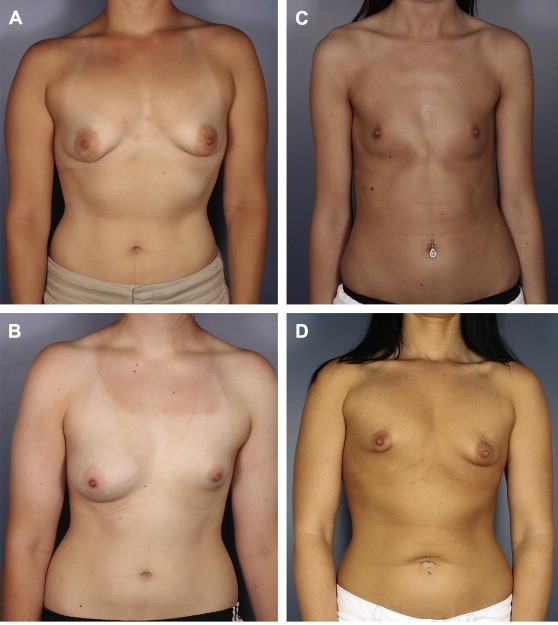
Fig. 2
( A ) Short distance between NAC and IMF. ( B ) Marked volume asymmetry with vertical height difference between left and right IMF. ( C ) Round rib cage and widely spaced breasts. ( D ) Tuberous breast deformity with volume and IMF height asymmetry.
- •
Round rib cage. A patient’s skeletal anatomy has a significant role in the outcome of breast enhancement. Implants rest against the chest wall and their projection is perpendicular to a line tangent to the rib cage. Thus, women with round chests (see Fig. 2 C) have implants that point radially outward, leading to a widened gap between the breasts and less projection of the implants. In this instance, patient education is again crucial, because patients are more accepting of the outcome when this anatomic variation and its limitations are discussed beforehand. It is harder to satisfy a patient when this is explained after surgery. Wider-based implants are preferred in these patients because they create more medial fullness. Limiting lateral dissection, and even leaving a slip of pectoralis muscle laterally, can help with limiting the lateral shift of the implants.
- •
Long nipple to sternal notch distance. Many patients with long nipple to notch distances present seeking breast augmentation when they would benefit from a mastopexy. These patients (and some surgeons) think that placing large implants will fill the skin envelop adequately and avoid the increased scarring associated with breast lifting. It is crucial to have a frank discussion with patients who possess long nipple to notch distances, or nipples below the IMF, regarding the outcome without undergoing a breast lift. In these cases, some patients may achieve results that are satisfactory, although this is usually an exception. For borderline cases, sometimes a circumareolar mastopexy is considered. This approach may lead to early revision instead of a revolumized and lifted breast, because patients are left with larger, more droopy breasts. In addition, I have found that patients are uniformly disappointed by the poor cosmetic appearance of the resulting enlarged, distorted, and scarred areolas.
- •
Pectus excavatum. Just as round rib cages present challenges to the plastic surgeon, so too does pectus excavatum. Pectus excavatum results in a radially inward-oriented breast. In this instance, moderately sized implants are a better choice, because they lessen the kissing-breasts deformity.
- •
Tuberous breasts, radiation damage, Poland syndrome, and severe asymmetry. Discussing each of these presentations is beyond the scope of this article, but recognition of the deformity, patient education, and creating the proper expectations of outcome are the keys to a satisfied patient (see Fig. 2 D).
Prevention of deformity following primary augmentation
Before discussing treatment options and strategy for revision breast augmentation, it is important to understand how to prevent the unsatisfactory result. There are important anatomic considerations that the plastic surgeon must recognize and carefully manage during primary augmentation:
- •
Short NAC to IMF distance. In cases in which there is insufficient inferior breast pole skin, it is important to educate patients about the limitations this anatomic variation presents ( Fig. 2 A). After augmentation, the inferior pole expands, although it is typically not sufficient for the nipple to be positioned at the midportion of the breast mound. High-profile implants place the point of maximum projection lower on the breast and create more projection for the relative volume. It does this at the expense of sacrificing medial and upper pole fullness, although the trade-off usually leads to a better aesthetic result. Selection of modest-size implants is wise in these challenging cases, and although some surgeons are comfortable with lowering the IMF surgically, I find it perilous (see Fig. 2 B).
Fig. 2
( A ) Short distance between NAC and IMF. ( B ) Marked volume asymmetry with vertical height difference between left and right IMF. ( C ) Round rib cage and widely spaced breasts. ( D ) Tuberous breast deformity with volume and IMF height asymmetry.
- •
Round rib cage. A patient’s skeletal anatomy has a significant role in the outcome of breast enhancement. Implants rest against the chest wall and their projection is perpendicular to a line tangent to the rib cage. Thus, women with round chests (see Fig. 2 C) have implants that point radially outward, leading to a widened gap between the breasts and less projection of the implants. In this instance, patient education is again crucial, because patients are more accepting of the outcome when this anatomic variation and its limitations are discussed beforehand. It is harder to satisfy a patient when this is explained after surgery. Wider-based implants are preferred in these patients because they create more medial fullness. Limiting lateral dissection, and even leaving a slip of pectoralis muscle laterally, can help with limiting the lateral shift of the implants.
- •
Long nipple to sternal notch distance. Many patients with long nipple to notch distances present seeking breast augmentation when they would benefit from a mastopexy. These patients (and some surgeons) think that placing large implants will fill the skin envelop adequately and avoid the increased scarring associated with breast lifting. It is crucial to have a frank discussion with patients who possess long nipple to notch distances, or nipples below the IMF, regarding the outcome without undergoing a breast lift. In these cases, some patients may achieve results that are satisfactory, although this is usually an exception. For borderline cases, sometimes a circumareolar mastopexy is considered. This approach may lead to early revision instead of a revolumized and lifted breast, because patients are left with larger, more droopy breasts. In addition, I have found that patients are uniformly disappointed by the poor cosmetic appearance of the resulting enlarged, distorted, and scarred areolas.
- •
Pectus excavatum. Just as round rib cages present challenges to the plastic surgeon, so too does pectus excavatum. Pectus excavatum results in a radially inward-oriented breast. In this instance, moderately sized implants are a better choice, because they lessen the kissing-breasts deformity.
- •
Tuberous breasts, radiation damage, Poland syndrome, and severe asymmetry. Discussing each of these presentations is beyond the scope of this article, but recognition of the deformity, patient education, and creating the proper expectations of outcome are the keys to a satisfied patient (see Fig. 2 D).
Current treatment options without the use of ADM
Revision breast augmentation for deformity has a long history, although ADMs have only been in widespread use in plastic surgery during the last decade. The treatment of breast implant malposition depends largely on the patient’s anatomy, presenting complaints, desired outcome, and anatomic limitations. This article reviews some of the tools available to help surgeons in the treatment of these deformities. The use of ADM is often complimentary.
- •
Plane exchange. Subglandular implants are prone to inferior displacement. There is little soft tissue for support and, as breast volume decreases, these implants are more likely to exhibit rippling and unacceptable palpability. Implants in the subglandular plane are also more susceptible to capsular contracture. Removal and replacement to a submuscular pocket may improve a great deal of the presenting complaints. It is debatable whether the prepectoral capsule needs to be removed. However, I find it is necessary to at least score the posterior wall, allowing the pectoralis muscle to expand. It is often necessary to use the inferior capsular wall to extend the reach of the pectoralis muscle and provide additional implant coverage in the lower outer quadrant.
- •
Capsular flaps. Following primary augmentation, especially in the setting of small breasts with large implants, there is often little soft tissue to work with during secondary procedures. Investigators have described using capsular flaps to reinforce pocket repair. Although some have found success with these techniques, the use of capsular tissue cannot always be relied upon in the case of diseased capsule because the strength and longevity of capsular tissue are inconsistent.
- •
Muscle-splitting biplane. In cases of animation deformity, or subglandular bottoming out, a muscle-splitting biplane placement has been advocated. This technique divides the pectoralis major muscle along its fibers and places the new implant in a partial subpectoral pocket. Superior pole coverage is provided and multiple-layer capsulorrhaphy is used to support the inferior and lateral implant pockets. A great deal of reliance is placed on the inferior capsulorrhaphy, and many investigators find that capsular repairs result in a high rates of recurrence.
- •
Capsulorrhaphy. Because there is often a paucity of manipulable tissue in the augmented breast, capsulorrhaphy remains a mainstay of revisionary strategy, especially in the setting of full or partially submuscular implants. Although capsular repair is generally technically easy, long-term results may be poor because the deforming forces that created the original deformity remain present and stretch the capsulorraphy, leading to recurrence.
- •
Neosubpectoral pockets. In the case of implants already in the submuscular plane, creation of a new submuscular pocket above the already present capsule provides the surgeon a fresh opportunity to create a better pocket for the implants. If the capsule is thin or wispy, it is technically challenging to keep the pockets separated.
- •
Fat grafting. Much interest has developed recently in fat grafting to the breast, and the topic of stem cells is often included in such discussions. There remains a great deal of confusion regarding the safety, efficacy, retention, and regenerative potential in this modality. Fat grafting is espoused by some to provide permanent volume augmentation, to reduce capsular contracture, and to smooth contour irregularities. However, all these are debated on many levels and additional studies are required to provide guidance for community practitioners.
- •
Mastopexy. If the nipple to notch distance is too long or there is too much inferior breast pole skin, a mastopexy is indicated to lift the nipple to the appropriate position on the breast mound or to redrape the skin as necessary. It is important to assess the implant position during these procedures because the implant can be bottomed out, the breast parenchyma may become ptotic, or both.
Related posts:
 Current State of the Art for Acellular Dermal Matrices in Breast Surgery
Current State of the Art for Acellular Dermal Matrices in Breast Surgery
 Acellular Dermal Matrices in Breast Implant Surgery: Defining the Problem and Proof of Concept
Acellular Dermal Matrices in Breast Implant Surgery: Defining the Problem and Proof of Concept
 The Role of Acellular Dermal Matrix in the Treatment of Capsular Contracture
The Role of Acellular Dermal Matrix in the Treatment of Capsular Contracture
 The Use of Human Acellular Dermal Matrices in Irradiated Breast Reconstruction
The Use of Human Acellular Dermal Matrices in Irradiated Breast Reconstruction
 Emerging Applications for Acellular Dermal Matrices in Mastopexy
Comparison of Different ADM Materials in Breast Surgery
Emerging Applications for Acellular Dermal Matrices in Mastopexy
Comparison of Different ADM Materials in Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


