Key points
• The patient’s perspective and desire must be understood and discussed in detail because they might be different from that of the surgeon’s.
• Dental evaluation is crucially important in the evaluation of facial aesthetics.
• Psychologic consideration is paramount to final patient satisfaction.
• Standardized and life-size photographic and radiographic documentation helps with thorough analysis and planning.
• Systematic entire facial analysis is essential to precise and comprehensive surgical planning.
Introduction
Aesthetic surgery of the face, especially when the focus is to alter the facial skeleton, requires a thorough facial analysis before devising an operative plan. Surgical intervention alongside orthodontic treatment helps achieve an optimal and predictable result. In this chapter, we have incorporated an overview of facial aesthetics into facial analysis to make it more useful for surgical planning.
History
First, the patient’s perspective and desires should be sought and clarified during the initial evaluation. Not uncommonly, the patient’s perceptions differ from that of the surgeon’s. In addition, detailed information about the patient’s current and prior medical problems should be gathered. Family history is also pertinent because family members may have similar facial abnormalities. History of speech problems or congenital craniofacial abnormalities is important to consider and monitor postoperatively.
Comorbidities, such as preexisting cardiac or renal dysfunction, require consultation with a specialist to secure clearance for surgical management. Patients with diabetes or immunocompromised patients are at a greater risk for infection and may have difficulty with wound healing. Last, patients with bleeding tendencies or those who bruise easily should be evaluated for any coagulation disorders, such as Von Willebrand’s disease. , Patients with coagulation disorders may not be aware of their condition and might require treatment intraoperatively for adequate hemostasis. Controlling blood pressure, whether it is high after surgery or low during surgery, is also key to preventing postoperative complications associated with bleeding, such as hematomas. As for any surgical procedure, patients should discontinue the use of nonsteroidal antiinflammatory medications and aspirin-containing products 3 weeks before the procedure.
Dental history and examination
A more detailed dental history is important for patients who are considering maxillofacial surgery. Any history of periodontal disease, tooth extractions, or prior dental interventions should be recorded. An up-to-date evaluation by a dentist is also essential. Patients who have had prolonged orthodontic treatment could have root resorption, which may render further orthodontic work prohibitive. Occasionally patients undergo orthodontic treatment for what is, in fact, a skeletal abnormality. It would be optimal to identify and reverse this course at an early stage. Otherwise, the changes induced by the orthodontic treatments should be reversed before surgical intervention.
The alignment of teeth, position of the palatal vault, and the shape of the dental arch should also be assessed. Crowding indicates the inability of the dental arch to accommodate teeth. Assessment of hygiene and periodontal disease should be evaluated because the presence of disease precludes orthodontic treatment. The most important part of the intraoral examination is assessing the patient’s occlusion. Any overbite, overjet, or crossbite should be noted, and the Angle classification stage should be determined. Details regarding the Angle classification and occlusion can be found in other sections of this text. Placing a tongue blade and asking the patient to bite down is a simple maneuver to assess the patient’s occlusal canting and to determine whether there is any asymmetry.
Any history of temporomandibular joint dysfunction should be explored. Patients with this condition may experience such symptoms as clicking, pain, locking, ear pain, bruxism, and headaches. Preoperative imaging can assist with determining the severity of the problem. The masticatory function and tenderness of the muscles can be evaluated on physical examination. The interincisal dimension, lateral excursion, and protrusive excursion should all be measured. Normal mandibular opening is 40 to 56 mm, and normal range of lateral movement at 1 cm opening is 9 to 13 mm.
Psychologic assessment
It is important to understand the patient’s underlying motive for seeking surgery. It is critical to ensure that the patient’s expectations are realistic. A detailed discussion of the surgical plan and the potential risks and outcomes with the patient is necessary, and one has to make sure that the patient understands the physical changes that will occur so that there are no surprises. Significant alterations in facial appearance are to be expected, and it may take time for the patient to adjust to these changes. The treatment plan and the expected outcome should ultimately be based on the patient’s desires. Even though the postoperative changes may be anatomically or “cephalometrically” correct, the patient may still be dissatisfied with the results if the patient’s and surgeon’s goals do not match or are not clear to the patient. Any signs of body dysmorphic disorder should be investigated in depth.
Photographic analysis
An important part of the preoperative assessment is taking photographs of the patient from the frontal, lateral, and oblique views. A digital camera or 35 mm single-lens reflex (SLR) camera (with a 60–100 mm lens), along with dual lighting, is recommended. A blue or black background should be used, and the patient should remove any jewelry, glasses, or makeup. The head should be in the standard anatomic position, and the patient should have a relaxed look. The photograph is taken from the top of the hair to the sternal notch, and a 1:1 reproduction ratio photo should be created. Life-size photographs can prove very helpful in planning orthognathic surgery and rhinoplasty.
Radiologic examination
Images ordered to screen for abnormalities include the following: a lateral and anterior/posterior cephalogram and panoramic radiographs. Traces of the cephalogram allow the surgeon to evaluate the bony and soft tissue anatomy, and this helps objectively determine the cephalometric relationships. A more detailed description of cephalometric analysis and imaging can be found in other chapters of this text. Panoramic radiographs demonstrate any pathology associated with the temporomandibular joints, in addition to any dental abnormalities.
Facial analysis
A systematic approach to the face, concentrating on the relationships among craniofacial, skeletal, and soft tissue components, is crucial to proper surgical planning. The patient’s skin is examined first to assess for thickness, color, and consistency and is evaluated for its susceptibility to form hypertrophic scars or keloids. Patients with lighter or freckled skin, blue eye color, and red hair are more susceptible to excessive bleeding and development of hypertrophic scars.
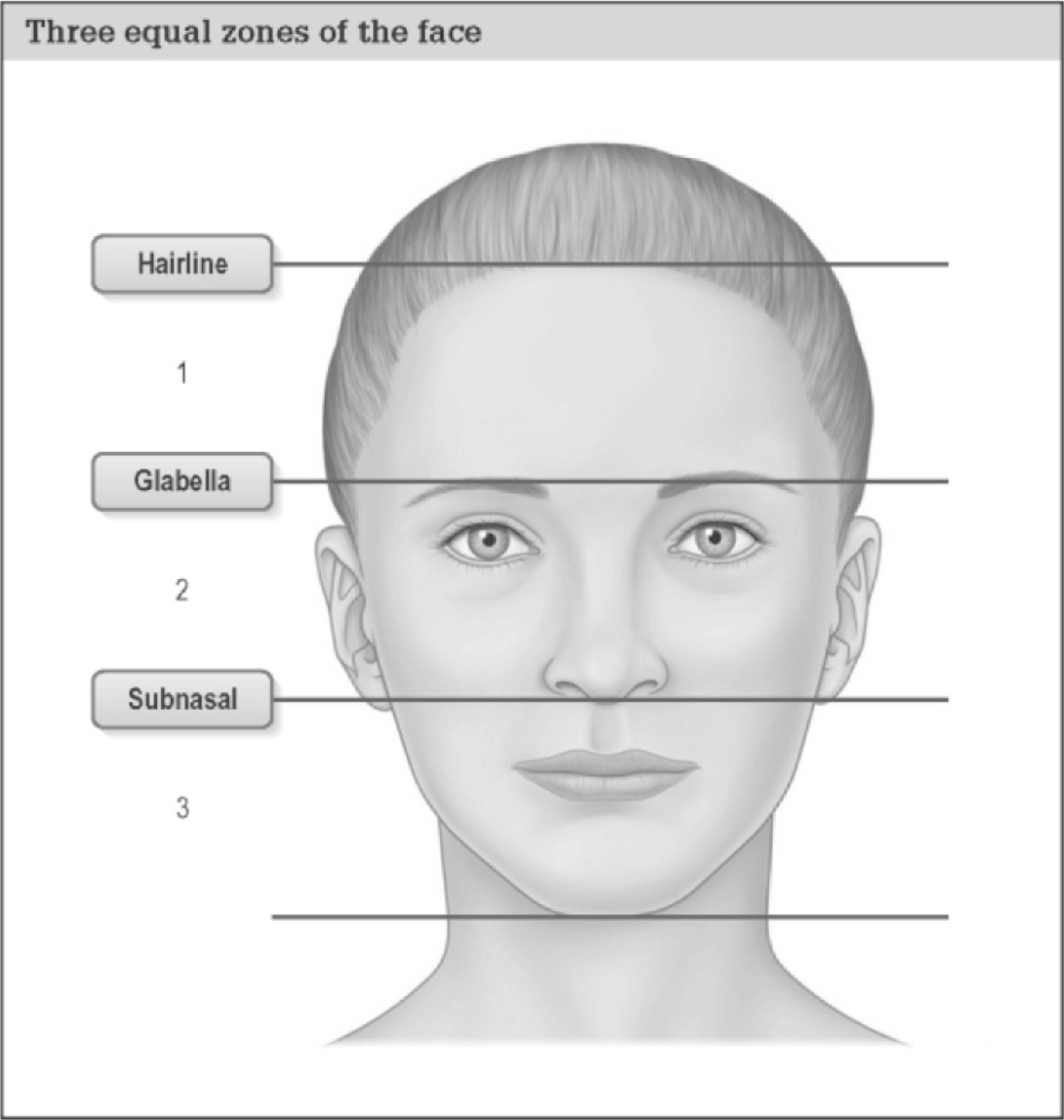
Frontal analysis
The face should be divided into three zones: upper, middle, and lower ( Fig. 2.1 ). The upper zone extends from the hairline to the eyebrows. The middle zone extends from the eyebrows to the subnasale. The third zone extends from the subnasale to the menton. The face can be divided into five equal segments in the frontal view. Two segments are occupied by the eyes, extending from the lateral canthus to medial canthus. One segment extends from one medial canthus to the other, and the last two segments extend from the lateral canthi to the lateral border of the ipsilateral temple. Any asymmetry in these segments should be noted.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


