Abstract
Calvarial trauma in the pediatric population differs significantly from that seen in adults. Nonaccidental head trauma is the leading cause of death in infants less than 12 months of age, and must be ruled out during the initial patient evaluation. Unlike adults, most acute fractures can be managed nonoperatively, given the increased remodeling capacity of pediatric skulls. However, close follow-up is warranted in instances of conservative management; infants with linear skull fractures can develop a rare complication during early childhood as a result of accelerated calvarial expansion, known as growing skull fractures. While rare, this condition can result in severe and permanent neurological damage if diagnosis is delayed. Reconstructive options for calvarial defects need to take into account the growing skull, and need for long-term reliability and outcomes. As such, nonautologous techniques have a limited role in pediatric calvarial reconstruction, with most centers advocating for autologous techniques. Failure to appreciate the differences between children and adults when treating pediatric calvarial trauma will ultimately result in complications that can lead to severe morbidity or even death.
Keywords
pediatric reconstruction, skull, bone grafting, secondary reconstruction, cranial defects, delayed reconstruction, growing skull fractures, leptomeningeal cysts, frontal sinus reconstruction, cranioplasty, split calvarial bone, alloplastic reconstruction, autograft
Background
Pediatric head trauma is a major source of morbidity, resulting in 600,000 emergency room visits annually within the United States. Between 10% and 30% of head traumas are associated with calvarial fractures, and of those greater than 50% have neurological injury. While the overall mortality rate from cranial fractures is low (2.9%), cranial trauma still accounts for 7000 deaths per year in the United States. The most frequently cited causes for calvarial fractures that require operative treatment include objects hitting the head (48.2%), followed by falls (13.8%), and motor vehicle collisions (MVC) (10.3%). There are clear sex- and age-associated trends: boys have twice as many calvarial fractures as girls and young children (<5 years) are injured predominantly by falls while older children are more likely to sustain head trauma from collisions and sports.
Among children less than one year of age, nonaccidental head trauma (NAHT) is the leading cause of death. Estimates of the prevalence of NAHT are almost certainly underreported, with studies showing anywhere from 24 to 47 cases per 100,000 children less than a year old. Children suffering from NAHT are predominantly male (61%), less than 6 months of age (55%), and African American (47%). Infants and toddlers with a history of abuse frequently will have long-standing neurological compromise that extends into adulthood. Despite significant effort on the part of practitioners to diagnose NAHT, one study showed that one-third of all cases of abuse go unrecognized. Of the children who belong to the unrecognized NAHT group, four out of five deaths can be prevented by earlier diagnosis of abuse. Children that are discharged with a missed diagnosis of NAHT frequently sustain further abuse, leading to rehospitalization or death. Abuse is missed more frequently in white children than minorities, in two-parent vs. single-parent families, and in children presenting before the age of 6 months, likely secondary to evaluation bias on the part of practitioners.
Diagnosis of nonaccidental head trauma is particularly difficult because the symptoms are nonspecific (vomiting, fever, irritability), the patients are preverbal, and the history surrounding the trauma can be misleading. Furthermore, a false-positive diagnosis of child abuse can cause significant grievance to the family and child and result in dissolution of the practitioner–patient relationship. Several studies have attempted to isolate findings to differentiate nonaccidental from accidental head trauma. A systematic review on clinical and radiographic characteristics associated with pediatric head trauma found that children with NAHT had increased rates of cerebral ischemia, skull fractures, subdural hematoma, retinal hemorrhage, rib and long bone fractures, seizures, apnea at time of presentation, and inadequate or inconsistent histories. Despite these findings, the authors acknowledge the overall nonspecificity of presenting symptoms and history and recommend a holistic and discerning approach to evaluating all cases of pediatric trauma. All patients should be evaluated for bruises on the head and face when they present with nonspecific symptoms such as vomiting, fever, and irritability. Dedicated pediatric radiologists are also better able to discover radiographic evidence of skeletal trauma than nonspecialized practitioners.
Nonoperative management is typically advocated whenever possible for calvarial fractures in children, given the cranium’s increased capacity for remodeling and healing at this age. A large retrospective review of 897 children at a Level I trauma center noted that the overwhelming majority of patients with acute skull fractures were managed nonoperatively (86.1%). Of the patients who did undergo operative intervention, more than half did so to address underlying traumatic brain injury. Only 6.5% of all pediatric skull fracture patients had surgical intervention to address the fracture in isolation; the children who underwent surgery did so primarily for depressed or open skull fractures, as well as for frontal sinus fractures or injuries with intracerebral processes.
While there is copious data on management of acute head trauma in adults and children, there is less consensus on management principles for delayed calvarial reconstruction in the pediatric population. Long-term outcomes in managing rare complications such as growing skull fractures or follow-up for nonautologous cranioplasty is lacking. Here we seek to consolidate the evidence supporting indications for pediatric reconstruction, and offer the authors’ management principles in dealing with complex defects.
Clinical Presentation
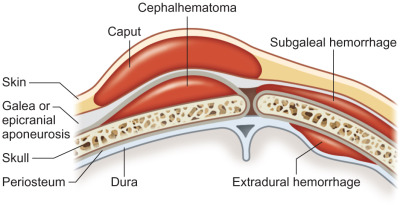
Pediatric calvarial fractures are classified by pattern (linear or comminuted, depressed or nondepressed, open or closed), and location (flat bone or skull base). Ninety percent of all pediatric skull fractures are linear, and approximately 15%–30% of these are associated with intracranial injuries. Linear skull fractures frequently advance to, but do not violate, suture lines. Most children with linear skull fractures will have overlying subgaleal hematomas ( Fig. 3.2.1 ). Comminuted fractures are a constellation of linear fractures. When found within the occipital or basilar regions, these are particularly concerning for repetitive or NAHT.
Lacerations with associated skull depressions warrant surgical exploration for foreign bodies, cerebrospinal leak, and injury to the dura or underlying brain parenchyma. Depressed skull fractures are commonly associated with intracranial injury (30%) and have an increased incidence of posttraumatic seizure and infection. Some children with depressed skull fractures will present with a palpable bony step-off or bony defect. Depressed skull fractures are clinically significant when displacement of the inner table is greater than one thickness of the bone; 33% of these will have dural lacerations. In the newborn or very young infant, depressed skull fractures are frequently referred to as ping-pong fractures, and can be managed nonoperatively with an obstetrical vacuum extractor. All depressed skull fractures, basilar skull fractures, linear skull fractures with greater than 3 mm diastasis, and fractures with intracranial injury, warrant evaluation by a pediatric neurosurgeon.
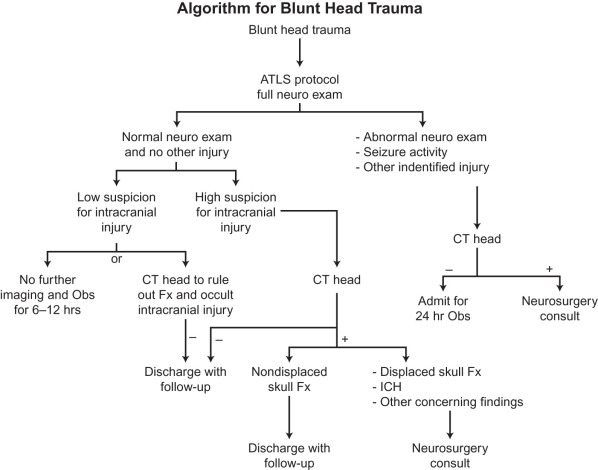
Several studies have attempted to risk stratify children who sustain head trauma into those who require hospitalization for observation or further radiological workup. Patients with a normal neurological exam in the setting of head trauma have less than a 5% chance of intracranial injury. Of those, only 1% require neurosurgical intervention. Current guidelines stipulate that children with an isolated, narrow (<3 mm diastasis) linear skull fracture and no focal neurological findings can be discharged without hospitalization. Follow-up studies have shown that this subset of patients is at low risk for complications, but national practices have yet to adopt the recommendations for direct discharge from the emergency room, resulting in avoidable healthcare expenditures. After discharge, the patient should be monitored at home for the first 24 hours following injury, and be assessed overnight for signs of vomiting or decreased arousal. Any neurological symptoms such as increased somnolence, seizure, persistent nausea or vomiting, coordination difficulties, confusion, or visual disturbance, warrants a repeat workup. A recent algorithm published by Blackwood and colleagues for evaluation and management of blunt head trauma (excluding NAHT) is depicted in Fig. 3.2.2 .
In infants, growing skull fractures (GSF), leptomeningeal cysts, or posttraumatic cephaloceles are a group of rare but serious complications that result from traumatic head injury with associated dural tears. Half of all cases are seen in children less than 12 months of age, and 90% of cases are found in children less than 3 years of age. Diagnosis of GSF is frequently missed as it is frequently seen in linear fractures in a closed head injury, and symptoms may present in a delayed fashion. Swelling, cephalhematoma or bony depressions at the site of the defect are also commonly noted. The challenge arises in risk stratifying patients with high probability of developing GSF or leptomeningeal cysts, prior to irreversible brain damage. Clinical presentation of GSF is varied; children can be asymptomatic or profoundly impaired with spasticity, seizures, hemiparesis, or visual disturbances.
Current guidelines for early diagnosis of GSF include the following parameters: (1) age <5 years with cephalohematoma; (2) bony diastasis greater than 4 mm; (3) underlying parenchymal injury; and (4) contrast MRI demonstrating dural tear and brain herniation. Definitive treatment relies on a successful duraplasty and cranioplasty, performed within a month of trauma to mitigate the effects on underlying brain parenchyma. Strict follow-up in patients who are managed conservatively is paramount, with care taken to document new neurological symptoms or an expanding scalp mass.
Neuroimaging
All pediatric patients with major head trauma require evaluation with a head computed tomography (CT) scan. For children with minor head trauma, current recommendations for ordering a head CT are based off of the Pediatric Emergency Care Research Network (PECARN) guidelines. The PECARN flow-chart is derived from a validated study that identifies children at very low risk of traumatic brain injury using clinical examination findings and Glasgow Coma Scores ( Fig. 3.2.3 ).
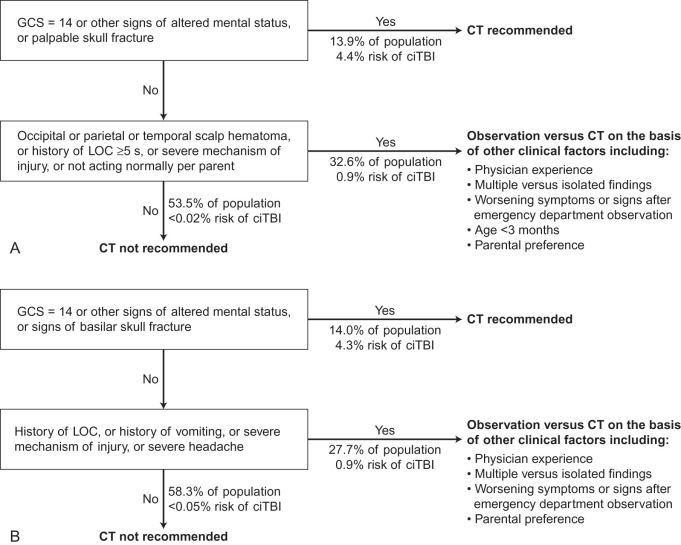
In brief, for children younger than 2 years of age, CT radiographs are not indicated if the child has normal mental status, no scalp hematoma, no loss of consciousness (LOC), no palpable skull fractures, has normal behavior, and has a nonsevere mechanism of injury. For children aged 2 years or older, CTs are not indicated for children demonstrating normal mental status, no LOC, no vomiting, nonsevere mechanism of injury, no symptoms of basilar skull fracture, and no headache.
Plain radiographs are not recommended as a screening tool when head trauma is suspected because of their limitations in assessing intracranial injuries. Orman and colleagues demonstrated that 3D reconstruction of CT images increased the sensitivity of diagnosing linear skull fractures in children across age groups. In addition, 3D-reconstructed images also increase the specificity of fracture diagnosis in children under 2 years of age, and where the fracture site is located close to a suture line. For children with suspected basilar skull fractures, a temporal bone CT without contrast with thin sections along the axial and coronal axes is helpful in providing a more nuanced understanding of involved structures.
The role of ultrasound is limited for the same reasons as that for plain radiographs. Namely, while it possesses good sensitivity (88%) and specificity (97%) for fractures diagnosis, it is less reliable in assessing intracranial pathology. Moreover, the technique is highly operator-dependent, and is unreliable in evaluating fractures of the orbital roof. The one area where ultrasound is effective is for screening patients for dural tears as seen with growing skull fractures or leptomeningeal cysts. The dura can be visualized as a bright linear structure through the acoustic window at the fracture site. The absence of a bright signal from the dura is indicative of a dural tear; either CSF or brain parenchyma fills the diastatic space.
For patients presenting for delayed calvarial reconstruction, CT with 3D reconstruction is helpful for evaluating the size, dimensions, and topography of the defect. Furthermore, patient-specific 3D-printed implants can be generated from the posttraumatic CT films and aid in allogeneic reconstruction techniques.
Indications for Repair
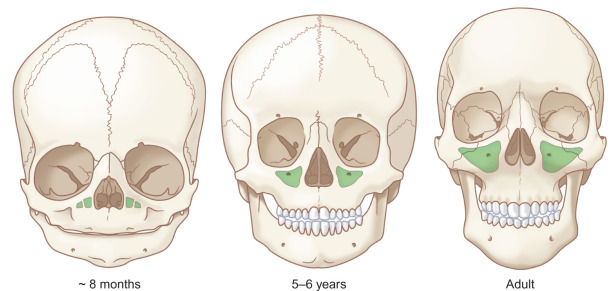
Several developmental and anatomical differences exist between pediatric patients and adults with respect to skull fractures. At birth, the skull is only 25% of its final size. By age 2, it has reached 75% of its adult size, and by age 10, 95%. The ratio in height between the cranium and midface diminishes as the child grows, owing to the preferential enlargement of the facial skeleton ( Fig. 3.2.4 ). At birth, the height discrepancy between the cranium and face is 8 : 1, decreasing to 4 : 1 at age 5, and 2 : 1 by adulthood. As such, within the 0–5-year age range, skull and orbital fractures are more common, while midface and mandibular fractures are more common in the 6–16-year-old age group. Retrospective reviews of facial trauma within the maxillofacial and neurosurgical literature demonstrate that decreasing age is an independent predictor for need of surgical intervention, due to several factors, including a protected environment, greater elasticity of immature bone, and the low ratio of midface to neurocranium height.
Infants and very young children have a higher remodeling capacity compared to young adults, and thus, nonoperative management has frequently been recommended for acute skull fractures in the young. In infants younger than one year, the osteogenic effects of dura compensate for small bony defects. However, conservative management must be weighed against anticipated cranial vault growth and expansion, which places the child at risk for unique complications. For example, fractures of the anterior cranial fossa can impact orbital growth, and structures of the upper face can be distorted by growth restriction or trauma to the calvarium, orbit, and frontal sinus.
The remodeling potential of pediatric calvarial bone is supported by case reports of complete resolution of anterior table contour deformities in the absence of operative management. In cases of isolated anterior table fractures without involvement of the posterior table or the nasofrontal outflow tract (NFOT), watchful waiting has resulted in spontaneous remodeling and resolution of minor contour depressions.
Growing Skull Fractures
Growing skull fractures, or leptomeningeal cysts, are frequently cited as a potential long-term complication of untreated linear skull fractures. The actual incidence of fracture extension is very rare, with reported rates ranging from 0.05% to 1.6%, and found almost exclusively in patients under the age of 3 years. Bonfield and colleagues reviewed 897 patients with skull fractures at a Level I trauma center and found that only 0.1% of patients with initial conservative treatment of a linear, frontal bone fracture (with orbital extension) developed a growing skull fracture that required delayed operative reconstruction. Growing skull fractures require an inciting dural injury. After the initial injury, herniation of intracranial tissues through the osteodural defect precludes apposition of dural tissues and healing. The defect ultimately enlarges as the child grows and can result in glial changes to the underlying brain parenchyma.
Most growing skull fractures are diagnosed within a year of the initial injury and present with localized swelling or pulsatile exophthalmos. On occasion, patients can have a delayed presentation, with neurologic symptoms such as headache, seizure, or other focal neurologic deficits that prompt further workup. Given the low incidence of late complications, current guidelines recommend close follow-up of all linear fractures with a diastasis greater than 4 mm, and early exploration only in cases with evidence of brain herniation on MRI. Liu et al. propose surgical exploration in all children with a linear fracture and MRI-proven brain herniation as close to the time of initial injury as possible, in an attempt to stymie progressive neurologic deficits. All children under 2 years of age with isolated skull fractures should be followed up 1–2 months after injury to assess for pulsatile swelling or a localized scalp defect raising concern for a growing skull fracture.
Definitive treatment for growing skull fracture requires resection of the leptomeningeal cyst and nonviable brain parenchyma, a water-tight duraplasty, and cranioplasty. In patients with associated hydrocephalus, a ventriculoperitoneal shunt may be placed. Liu et al. recommend autologous dural reconstruction using pericranium and fascia lata, given the lower complication rates as compared to artificial dural substitutes.
In instances of early diagnosis and repair, the bony margins along the fracture site are healthy and well vascularized. Significant cranioplasty can be avoided as long as the bone along the fracture site is well reapproximated. In patients with late presentation and diagnosis, long-term changes to the bone and dura result in a larger defect that may require significant cranioplasty and staged reconstruction. The neurological sequelae from late stage growing skull fracture are also less likely to be reversible than if the fracture were treated at an earlier point.
Pediatric Cranioplasty – Surgical Techniques
Calvarial cranioplasty on a growing skeleton presents unique challenges in the pediatric population. The timing of repair and choice of reconstructive technique are still frequently debated, without a clear consensus except in select situations. The fundamental principle of “replace like with like” is particularly relevant in this population, making autologous reconstruction the gold standard. Some surgeons find alloplastic options necessary, which includes ceramics, metals, hyaluronic acid, or a combination. The authors prefer the utilization of autogenous bone graft when at all possible as the pernicious sequelae of alloplastic material can arise at any point with complications that can potentially last a lifetime. The common indications for cranioplasties include repair after decompressive craniectomy (36%), bone flap infection following previous neurosurgical intervention (18%), osteomyelitis (14%), traumatic bone loss (14%), congenital calvarial dysmorphology (9%), or growing skull fractures (9%). Goals of repair include improved cosmesis and restoration of a protective encasement of the brain. In some instances, reconstructive cranioplasty can also provide the added benefits of improved cerebral blood flow, improved cerebrospinal fluid dynamics, and resolution of the syndrome of the trephined.
In the acute setting, the timing of reconstruction is dictated by the clinical condition of the patient. Extensive cranioplasty is generally not attempted until the patient is hemodynamically stable, free from infection, and has normalized intracranial pressures (3–6 months). Piedra and colleagues advocate for early repair (less than 6 weeks) following decompressive cranioplasties using autologous bone grafting. However, several other groups saw no clear difference in timing of repair. In infants younger than 12 months of age, a switch cranioplasty can be performed. Native calvarium is taken from the unaffected side and used to reconstruct the defect. The donor site then regenerates by harnessing the osteogenic potential of dura.
Autologous Reconstruction
Autologous reconstruction provides a restorative option that can grow with the patient. Once fully integrated and vascularized, bone grafts pose minimal infectious risk. However, autologous methods are often erroneously thought to be constrained by availability of donor tissue when the closure of large defects can actually be enhanced by utilizing advanced harvesting techniques. The most commonly used autologous tissues for cranioplasty are calvarial bone, hip, and rib.
In adults, replacement of the bone “flap” *
* Neurosurgical literature will frequently refer to the bone removed during a decompressive craniotomy as a bone flap, despite its lack of vascularity. For purposes of consistency, plastic surgeons frequently adopt the nomenclature of their neurosurgical colleagues and use “bone flap” in lieu of the more precise terminology, “bone graft.”
following decompressive craniotomies is generally regarded as the most expedient method to restore contour and provide protection of the brain. In children, bone resorption following delayed replantation of autologous bone flaps can be significant, and on occasion compromises the longevity of the repair. Grant and colleagues found that 50% of children who had delayed bone flap replacement following decompressive craniectomy required reoperation due to bone resorption, compared to 6.5%–26% in adults. Other groups reported similar rates of reoperation due to either resorption or infection, and found an inverse correlation between age at time of repair and risk of resorption.At the time of replacement, maximizing apposition of the bone flap edges within the craniotomy defect will promote greater osteointegration. Rigid fixation of the nonvascularized autologous bone graft also minimizes graft resorption and is shown to facilitate osteoconduction. Indeed, the high rate of bone resorption described in the neurosurgical literature is likely to be largely a function of poor bone to bone apposition and inadequate rigid fixation at the time of surgery.
Rates of resorption correlate to the size of the cranial defect; defects greater than 75 cm 2 have a failure rate greater than 60%, whereas smaller defects have a negligible failure rate. Bone flaps are preserved following craniotomy via subcutaneous storage or cryopreservation. Bone flaps can be stored in an abdominal pocket, anterolateral thigh, or under the scalp where their osteocytes can be nourished by the surrounding blood supply. At our institution, bone flaps that are set aside for delayed reconstruction are predominantly cryopreserved. However, if there is a possibility that the patient will move or be transferred to a separate institution, the flaps are embedded within the abdomen to ensure transport with the patient.
Subcutaneous storage can reduce the degree of bone devitalization as well as infection, but can be uncomfortable for children, and require creation of a second surgical site. Cryopreserved bone flaps are associated with high rates of bone resorption (up to 50%), which in turn, can lead to increased rates of infection and cosmetic deformity from inadequate bone stock. Alternative methods of sterilization such as autoclaving and irradiation have also been proposed, but are associated with equal or higher rates of bone devitalization and are thought to suffer from the destruction of bone healing factors such as BMP. Ultimately, large, long-term comparative studies in adults evaluating the efficacy and morbidity of subcutaneous bone flap storage versus cryopreservation indicate similar outcomes between the two methods. Within the pediatric literature, however, there is suggestion that increased devitalization of bone is seen with cryopreserved bone flaps, though the data is limited and more extensive studies are needed prior to drawing a definitive conclusion.
Despite the limitations and high resorption rates, the pediatric neurosurgical community still recommends delayed primary reconstruction with bone flaps. In the event of bone resorption, a delay of at least one year is recommended before attempting another repair to maximize the opportunity for spontaneous ossification. At our institution, the authors replace the bone flap in the immediate phase, insofar as the patient is stable and brain swelling has resolved. In instances requiring significant bone grafting or delayed reconstruction (i.e., where the original bone flap was lost or resorbed), the reconstruction is delayed months to years to allow for maximal spontaneous ossification and fibrosis around the defect. Between the ages of 6 and 8, we acquire a CT scan to evaluate the diploic space prior to proceeding with a large split calvarial graft cranioplasty.
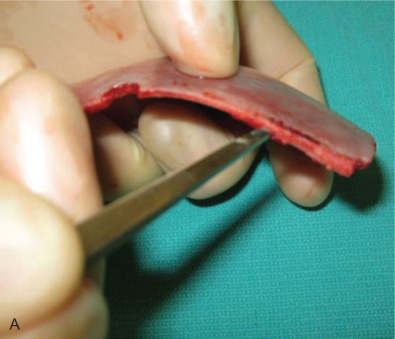
In children with full-thickness calvarial defects from trauma or infection, split calvarial bone grafts, particulate calvarial grafts, and split rib grafts are commonly used in repair. Cranial bone has a lower rate of resorption than grafts harvested from elsewhere along the body, as it is denser. Split and particulate grafts demonstrate lower levels of resorption and infection as compared to bone flaps. The traditional assumption that calvarial splitting is unreliable in children under 5 has largely been debunked. Vercler, Buchman, and colleagues demonstrate use of split bone grafts in children as young as 3 months applied to a range of calvarial defects. Bone is harvested as a full-thickness segment, and split between the inner and outer cortices through the diploic space. For large reconstructions requiring bone grafting, the procedure is delayed until the child is between 6 and 8 years of age, at which point a CT scan is obtained to ensure adequate development of the diploic space for bone splitting. One cortex is used to repair the donor site while the second cortex is used for repair of the defect ( Fig. 3.2.5 ) ( ).