Patellofemoral Instability Reconstructions
Matthew D. Milewski
Potential Procedures
Knee arthroscopy
Open lateral release
Medial patellofemoral ligament (MPFL) repair/medial plication/imbrication
MPFL reconstruction
Tibial tubercle osteotomy (TTO)
Roux-Goldthwait procedure/patellar tendon transfer
Patellar Instability Surgery—General Principles
Surgical Indications for Primary (First Time) Acute Patellar Instability
Loose body or osteochondral fracture
Failure of conservative treatment following primary dislocation
Concomitant surgical procedures (ie, cartilage treatment)
History of recurrent contralateral patellar instability (relative indication)
Surgical Indications for Recurrent/Chronic Patellar Instability
Failure of conservative treatment including rest, activity modification, patellar stabilization bracing, and physical therapy
Continued instability ± patellofemoral pain
Loose body or osteochondral fracture
Cartilage injury requiring surgical treatment/failure of conservative treatment
History
Important considerations in the workup of a patient with acute or chronic patellar instability should include information about contralateral knee issues especially patellofemoral instability
Family history is a strong predictor of recurrent and/or contralateral patellar instability1
Hyperlaxity or other joint instability/laxity
Dislocation versus subluxation of the patella
Reduction maneuvers or medical/emergency department treatment needed for patellar reductions
Previous conservative treatment including activity modifications, bracing, and physical therapy. It is important to understand the type of treatment and duration. Also, it is important to understand the types of bracing and physical therapy modalities that have been utilized
Physical Examination
Age
Skeletal maturity
Hyperlaxity (Beighton-Horan scale)—9-point scale originally designed to assess for Ehlers-Danlos syndrome.2 Useful in assessment of all patients with suspected hyperlaxity. Generally, a score of >4 out of 9 is considered to be indicative of hyperlaxity
Rotational alignment assessment
Femoral version—Femoral anteversion is common with patellar instability
Prone examination of hip range of motion (ROM)
Prominence of greater trochanter can be used to measure femoral version3
Tibial torsion—External tibial torsion is common with patellar instability
Prone examination of foot-thigh axis
Foot progression angle gives assessment of overall rotational alignment of the lower extremity
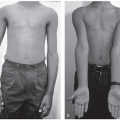
Should also assess patellar position with feet forward as the patellae will often face inward with feet forward in patients with patellar instability/patellofemoral syndrome (“Grasshopper eyes”)
Coronal alignment assessment
Genu valgum versus varus—Genu valgum common in patellar instability
Can be assessed by Q-angle or finger breaths between the medial malleoli with knees together
Important to remember Q-angle can be unreliable due to subluxation of patella in full extension or change in Q-angle with knee flexion angle
Effusion
Patellar height
Q-sign—Lateral translation of the patella during the last 30° of extension (or conversely medial translation of the patella during the first 30° of flexion)
Lateral retinacular tightness—Assessed by comparing the ability to anteriorly tilt patella laterally versus medially
Patellar apprehension—Generally done at about 30° of knee flexion with lateral translation of the patella causing the patient pain, anxiety/apprehension, or the sense of impending subluxation/dislocation
Tenderness over the medial retinaculum/MPFL complex—Can help to localize the site of MPFL disruption (patella, femur, or midsubstance)
Imaging Considerations
Anteroposterior (AP), lateral, notch, and sunrise views are standard for young patients with acute/chronic knee injury/pain
Presence of loose body/osteochondral fracture—Must distinguish between loose body/intra-articular fracture versus MPFL avulsion fracture. Magnetic resonance imaging (MRI) is often needed to distinguish these entities
Patellar height—often alta in patellar instability—can be assessed with Caton-Deschamps index in skeletally immature and mature patients. Insall-Salvati ratio is less reliable in skeletally immature patients where the tibial tubercle is not fully ossified
Patellar tilt/subluxation—Best assessed on the sunrise view. Needs to be sunrise view with thoughtful positioning of the knee as too much knee flexion underrepresents the presence of subluxation or trochlear dysplasia
Trochlear dysplasia—Dejour classification A-D—Dejour et al4
Crossing sign, the supratrochlear spur, and the double-contour sign on lateral knee radiographs
Skeletal maturity—Bone age can be useful
Standing alignment film with patella forward from hips to ankle can be useful to assess for genu valgum/leg length differences
MRI indicated following most patellar instability events (especially if effusion present) to assess primarily/acutely for a cartilage injury/osteochondral fracture
Cartilage injury/osteochondral fracture—Often medial facet of patella and far lateral portion of lateral femoral condyle
Location of MPFL complex injury—Femoral, patellar, or midsubstance. More often patellar-sided injury in adolescents compared with adults.5 Can be associated with MPFL avulsion fracture (medial aspect of patella)
Trochlear dysplasia6
Trochlear sulcus angle >145°
Trochlear depth < or equal to 3 mm on axial MRI sequences
Ventral trochlear prominence > or equal to 7 mm with step-like transition on midsagittal MRI
Anterior prominence at most anterior/proximal part of femoral trochlear on midsagittal MRI
TTTG (tibial tubercle trochlear groove) distance can be measured on MRI or computed tomography (CT) imaging. Measures the distance between the center of the patellar tendon at its tibial insertion and a line through the deepest point of the trochlear groove tangential to a line across the posterior aspect of the femoral condyles
Generally, >20 mm is an indication for potential TTO correction in skeletally mature patients with chronic patellar instability
Can be affected by knee flexion
Knee Arthroscopy
Indications
Generally recommended in most cases of patellar instability surgery
Arthroscopy allows an assessment of intra-articular pathology. Patellar instability cases particularly involve an assessment of the cartilage of the patella and the lateral femoral condyle, where cartilage injuries are most common
Arthroscopy allows for an assessment of patellar alignment (particularly tilt and subluxation)
Arthroscopy can allow for arthroscopic lateral release in association with other arthroscopic and open procedures
Equipment
Standard 30° 3.5-mm arthroscope for vast majority of cases
A 70° 3.5-mm arthroscope can improve the field of view if looking for loose bodies posteromedially or posterolaterally
Smaller knees (generally in patients younger than 5 or 6 years) may necessitate a smaller 2.7-mm-sized arthroscope
Arthroscopic instruments for a loose body removal should be available
Curettes (in particular, sharp ring curettes) are useful if cartilage debridement is needed. Also useful for cartilage biopsy for matrix-induced autologous chondrocyte implantation if needed
It is important to have fragment/osteochondral fracture fixation sets available
These can include SmartNail (Linvatec) or bioabsorbable headless compression screws
Metal screw fixation is also possible for osteochondral fracture fixation and can include headless compression screw sets (ie, Acutrak screw set or 2.4/3.0 mm Synthes headless compression screw sets) or small-headed screws (ie, Synthes minifragment screws) can be used (but do require placing the head of the screw below the articular cartilage surface)
Radiofrequency ablation device or arthroscopic Bovie are 2 different options for potential arthroscopic lateral release
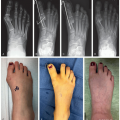
Position (Figure 32.1)
Supine, standard OR bed. One can use a radiolucent extension if extensive fixation if needed. However, we find it easier to use a standard bed with the patient positioned distal on the table to facilitate the C-arm fluoroscopy coming under the bed
An arthroscopic lateral side post or an arthroscopic circumferential leg holder can be used. These are less crucial for patellofemoral surgeries as extensive valgus stress is usually not needed in these cases (as they are needed at times for medial meniscal repair, for example)
Tourniquet can be placed as far proximally as possible. An inflated tourniquet may inhibit or alter normal tracking of the patella. Therefore, it is beneficial to do the examination under anesthesia (EUA) prior to utilizing the tourniquet. It may also be beneficial to hyperflex (>120°) the knee during tourniquet inflation to not capture the quadriceps. This can facilitate more normal patellar tracking during surgical correction
 Figure 32-1 ▪ Supine position for patellofemoral surgery of the right knee. Markings allow for standard knee arthroscopy and medial patellar incision for medial patellofemoral ligament (MPFL) reconstruction. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Examination Under Anesthesia
Best done after general anesthesia is induced and usually after regional anesthetic has been completed. As noted above, it is also best to be done prior to tourniquet placement and inflation
EUA should include an assessment of ROM, crepitus, varus/valgus stability, anterior cruciate ligament/posterior cruciate ligament (ACL/PCL) integrity (anterior drawer, Lachman test, posterior drawer), patellar tracking (assessment of J-sign), and patellar translation (number of quadrants of medial and lateral translation at 0° and 30° of flexion)
Lateral release may be indicated if patella is not reducible to the trochlea or if there is significant tilt on examination or imaging
Surgical Approach (Figure 32.2)
Standard anteromedial and anterolateral portals. A superior (“high”) lateral portal can be utilized for assessment of the patellofemoral articulation (both in terms of diagnosis and also to assess tracking post intervention arthroscopically)
 Figure 32-2 ▪ Lateral view of right knee arthroscopy. Standard 30° arthroscope is in the lateral portal with an arthroscopic instrument in the anteromedial portal. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Surgical Technique
Standard diagnostic arthroscopy is appropriate to assess all 3 compartments including posteromedial and posterolateral (especially in cases of possible loose body/osteochondral fracture)
Loose bodies in the lateral compartment can hide posterolaterally above the meniscus, posterolaterally below the posterior horn of the lateral meniscus, and laterally below the body of the lateral meniscus. There is much more of a recess below the lateral meniscus when compared with the medial meniscus
The patellofemoral joint should be assessed for loose bodies, damage to the facet cartilage of the patella, trochlear dysplasia, and presence of trochlear cartilage injury/abnormality (Figure 32.3)
Preoperative imaging should be referenced for trochlear dysplasia. Presence and examination for a supratrochlear spur can indicate higher grade trochlear dysplasia and may indicate the need for a trochleoplasty in specific cases
Assessment of patellar tracking can be done arthroscopically by bringing the knee through a gentle ROM (often with arthroscope in the superolateral high portal). Generally, by bringing the knee from full extension to about 60° of flexion, one can assess the patellar tracking from all the way to trochlear engagement. Remember that the fluid from arthroscopy and an insufflated tourniquet can change the tracking of the patella
Patellar tilt and translation can not only be assessed with an EUA but can also be assessed during arthroscopy. The need for lateral release is generally done preoperatively. In general, appropriate tilt should consist of the ability to passively correct or gently evert the lateral edge of the patella. Failure to be able to evert or correct to neutral of the patella can indicate the need for a lateral release
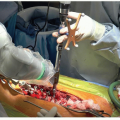
Arthroscopic lateral release can be indicated for lateral patellar compression syndrome or as part of the corrective/reconstructive process for patellar instability. In general, it is no longer indicated as a solo procedure for patellar instability. More extensive open lateral release or retinacular lengthening procedures can be done when associated with congenital or habitual patellar dislocators where the patella is fixed laterally. Open lateral release may be appropriate in these more extensive realignments or when combined with distal procedures such as a TTO or Roux-Goldthwait procedures (Figure 32.4)
Arthroscopic lateral release should involve release of the lateral retinaculum and capsule from the junction with the vastus lateralis proximally and released distally to the anterolateral portal location (within the lateral anterior fat pad)
Arthroscopically, this can be completed with a radiofrequency ablator or arthroscopic Bovie or alternatively involve passage of scissors through the anterolateral portal with hemostasis assistance after release (Figures 32.5 and 32.6)
Proximally, the release should start near the superior border of the patella and the junction of the vastus lateralis
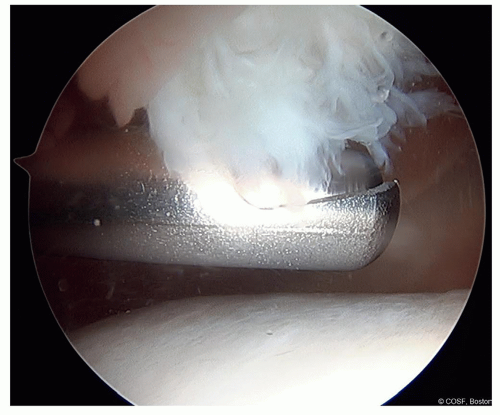
Figure 32-3 ▪ Arthroscopic view of the medial patellar facet high-grade chondral damage from chronic patellar instability. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
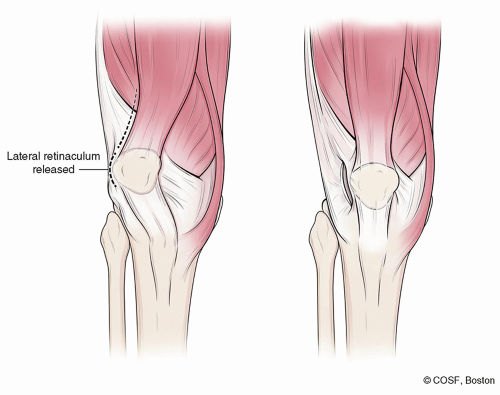
Figure 32-4 ▪ Lateral release. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
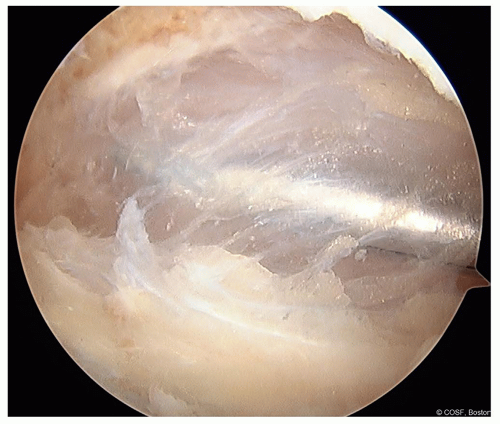
Figure 32-5 ▪ Arthroscopic view of the left knee undergoing an arthroscopic lateral release. A portion of the lateral capsule has been released with a radiofrequency ablator. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
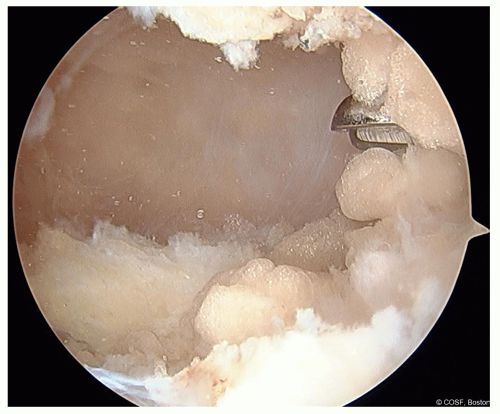
Figure 32-6 ▪ Arthroscopic view of the left knee undergoing an arthroscopic lateral release. Curved Mayo scissors can be used to complete the release. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
It is technically important not to get too superficial with your release as in slender young knees, the subcutaneous tissue can be very close to the retinaculum and overly aggressive releases can scar the skin/subcutaneous tissue
Open lateral release can be done for more extensive releases especially with congenital or habitual dislocators in flexion. For these releases, a larger lateral incision is needed (or lateral extension of an anterior midline distal incision). A Cobb elevator can be used to release the vastus lateralis proximally with a subperiosteal release appropriate in younger patients to facilitate hemostasis. This open lateral release is often left open for these larger releases, but a partial closure or retinacular lengthening can be done in some settings
Postoperative Care
Postoperative care of the arthroscopic procedure is often dictated by the other procedures it is often combined with including, but not limited to, cartilage fixation, MPFL reconstruction, medial plication, TTO, etc
Weight-bearing is often limited initially, especially if cartilage restoration procedures (such as osteochondral fracture fixation or microfracture) are completed. Traditionally, weight-bearing is limited for about 4 to 6 weeks for these cartilage procedures. ROM can be done during this time but might be limited again by associated procedures such as soft tissue or bony reconstructions
Complications
Arthroscopy can be complicated by persistent effusion or hemarthrosis (particularly if an arthroscopic lateral release is completed). Good intra-articular intraoperative hemostasis can mitigate some of this risk. Postoperative compressive wraps and/or bracing can also help this process
MPFL Repair/Medial Plication
Indications
MPFL repair or medial plication has evolved over the past several decades. It was the workhorse soft tissue procedure for patellar stabilization. MPFL reconstruction has replaced it in some indications
Currently, the author’s indications for MPFL repair is in the setting of a first-time dislocator with a loose body that requires surgical treatment as an adjuvant to their cartilage surgical treatment. This is particularly important in the setting of an acute avulsion off the medial patella
MPFL repair is best addressed at the site of injury. The MPFL complex can be injured or avulsed off the femur, off the patella or midsubstance. In pediatric and adolescent patients, it is often injured off the patella. This is best confirmed on preoperative imaging
MPFL repair or reconstruction usually accompanies TTO when used for patellar stabilization
Equipment
Standard setup as described above
Medial plication or MPFL repair can be done with side-to-side repair or plication sutures. This can be done with absorbable #1 Vicryl sutures or #2 nonabsorbable ultra-high-molecular-weight polyethylene (UHMWPE) sutures
For intrasubstance injuries or patellar-sided avulsion injuries, the author prefers to use anchor-based fixation in the medial patella. These can be biocomposite, metal, or all-suture anchors. Currently, the author prefers all-suture anchor fixation within the patella (due to small size of the anchors, ie, 1.8-mm Q-fix anchors [Smith & Nephew, Andover, MA])
Femoral-sided MPFL avulsion injuries can be addressed with suture or suture anchor-based constructs
Position
Standard supine positioning as described above in the knee arthroscopy section
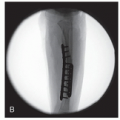
Proper positioning for potential use of fluoroscopy is important for concomitant procedures. Fluoroscopy can be used to identify patellar or femoral anchor positioning
Examination Under Anesthesia
Best done after general anesthesia is induced and usually after regional anesthetic has been completed. As noted above, it is also best to be done prior to tourniquet placement and inflationRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree