Key Words
oncoplastic surgery, breast conservation surgery, partial breast reconstruction, level 2 oncoplastic surgery, oncoplastic reduction surgery, breast cancer surgery, breast cancer surgical treatment
Introduction
Partial breast reconstruction using large volume displacement oncoplastic techniques has become an important part of reconstructive practice. As an option for women with breast cancer who undergo breast conservation therapy (BCT), this approach has many proven benefits. In some well-selected patients it improves upon standard lumpectomy alone and in others it has advantages over skin-sparing mastectomy and reconstruction.
The term oncoplastic combines cancer surgery and reconstruction, with the two main reconstructive techniques being volume replacement and volume displacement. The specific reference to large volume displacement oncoplastic surgery implies reduction or mastopexy techniques used in breast cancer patients with moderate- to large-sized breasts. Such oncoplastic designs include large partial mastectomy resections and involve reconstruction with mastopexy or reduction mammoplasty designs to reconstruct the large volume defects with contralateral symmetry breast mastopexy or reduction mammoplasty operations. The goals of the oncoplastic approach are to avoid the BCT deformity, minimize positive margins, broaden indications for BCT, avoid full mastectomy and preserve shape.
Oncoplastic surgery expands the indications for breast conservation allowing the resection of much larger tumors relative to breast size, tumors larger than 4 cm, locally advanced cancers, and prior neoadjuvant chemotherapy that would otherwise only be treated with mastectomy. Partial reconstruction prior to radiation therapy will minimize the number BCT deformities and improve breast shape. Compared to partial mastectomy alone, there is less deformity long term especially after radiation with regards to possible nipple eversion volume loss deformity and breast asymmetry. Compared to simple mastectomy with reconstruction, the large volume displacement oncoplastic approach has similar locoregional recurrence and overall survival rates, preserves better skin and nipple sensation, is aesthetically better according to validated patient self-assessment tools, and has been shown to result in lower complication rates and without potential donor-site morbidity.
Indications
The various indications for large volume displacement oncoplastic surgery are listed in Table 17.1 . Women with central or lower quadrant tumors have also been shown to have a worse cosmetic outcome because of tumor location, especially when a significant amount of skin is removed. Lower quadrant partial mastectomies have been shown to reduce cosmesis by 50% when compared to other quadrants. The tumor to breast ratio is one of the most important factors when predicting the potential for a poor outcome. In general, when more than 20% of the breast is excised with partial mastectomy, the cosmetic result is likely to be unfavorable. A recent study of 350 patients demonstrated that the maximal volume of tissue resected with lumpectomy without resulting in unacceptable aesthetic and functional outcomes of decreased quality of life (QOL) were 18%–19% in the upper outer quadrant, 14%–15% in the lower quadrant, 8%–9% in the upper-inner quadrant and 9%–10% in the lower inner quadrant.
| Cosmetic Reasons | Oncological Reasons |
|---|---|
|
|
Contraindications to the immediate oncoplastic technique include those patients not candidates for breast conservation surgery (BCS), prior history of chest wall irradiation, diffuse multicentric breast disease, inflammatory breast cancer and those patients without sufficient breast tissue remaining to warrant BCS.
Preoperative Evaluation and Special Considerations
When indicated, it is better to perform oncoplastic techniques immediately at the time of tumor resection. This is often preferred since it is only one procedure and has the benefits of operating on a non-irradiated breast. Reduction techniques prior to radiation therapy result in a significantly lower complication rate when compared to performing reductions after completion of radiation therapy. If margins are a major concern, the delayed immediate approach can be performed, where partial breast reconstruction is delayed until confirmation of negative margins and before radiation therapy. When a BCT deformity exist, the partial reconstruction can be performed in a delayed fashion. Since the delayed approach requires operating on an irradiated breast, this often has higher postoperative complications, increased need for flap reconstruction and poorer aesthetic outcomes.
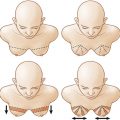
The breast reshaping oncoplastic procedures all essentially rely on advancement, rotation or transposition of a large area of breast using mastopexy or reduction techniques to fill a moderate- to large-sized defect. This absorbs the volume loss over a larger area. The most common large volume displacement techniques are shown in Table 17.2 .
| Skin Incision Pattern | Pedicle Blood Supply to NAC | Tumor Location in Breast |
|---|---|---|
| Circumvertical | Superior | Inferior pole |
| Inverted T | Superomedial | LIQ, LOQ, UOQ |
| Inverted T | Inferior | LIQ, LOQ, UOQ, UIQ |
| Inverted T | Free nipple graft | Central |
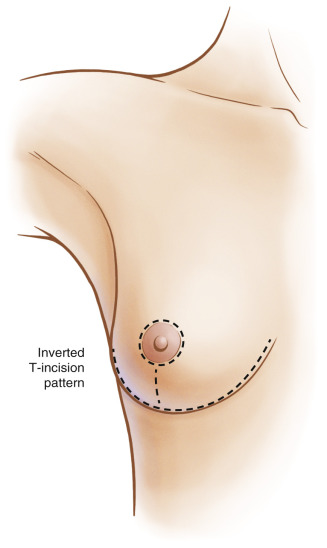
The ideal patient is one where the tumor can be excised within the expected breast reduction specimen, in medium to large or ptotic breasts where sufficient breast parenchyma remains following resection to reshape the mound. Past descriptions for oncoplastic operations have included: (1) planning skin incisions and parenchymal excisions following reduction/mastopexy templates; (2) parenchymal reshaping following excision; (3) repositioning the nipple; and (4) correction of the contralateral breast for symmetry. Any moderate to large breast can be reconstructed using these techniques unless a skin deformity exists beyond the standard Wise pattern. Plastic surgeons are all familiar with these techniques, making the incorporation of this approach into their reconstructive practice an easy addition. Using the new ASBrS/SSO/ASTRO margin guidelines, as long as a breast cancer can be removed with adequate margins (no tumor on ink for invasive cancer, and at least a 2-mm margin for ductal carcinoma in situ ) and the overlying skin is not diseased, taking the overlying skin is not necessary. Therefore, using standard skin incision patterns such as the circumvertical or inverted T skin patterns and planning a pedicle away from the cancer site can allow for easy access to the cancer site. Specific steps in skin incision design are described in the cases below.
Surgical Techniques
Once the resection is performed (see Case 17.1.6 ), the cavity is inspected paying attention to the defect location in relation to the nipple, as well as the remaining breast tissue. Clips should be placed either by the breast or plastic surgeon at the borders of the lumpectomy defect (at least 6 clips). The reconstructive goals include: (1) preservation of nipple viability; (2) closure of the defect space; and (3) reshaping of the breast mound. If the partial mastectomy resection is close to the nipple–areola complex, the obliteration of dead space is important to reduce the nipple inversion complication especially from the scarring post-radiation. The nipple and dermatoglandular pedicle is dissected ( Case 17.1.8 ), and remaining tissue is resected if necessary for completion of the reduction. The contralateral procedure is performed using a similar technique The ipsilateral side is typically kept about 10% larger to allow for radiation fibrosis.
Larger, more remote defects and defects in smaller breasts can be reconstructed using autoaugmentation flaps during oncoplastic reduction or mastopexy procedures (see Case 17.1 ). Autoaugmentation options include extending the primary pedicle to rotate into a defect or creating a secondary dermotoglandular pedicle to move independent to the nipple pedicle and fill a defect ( Case 17.1.9 ).
Case Examples
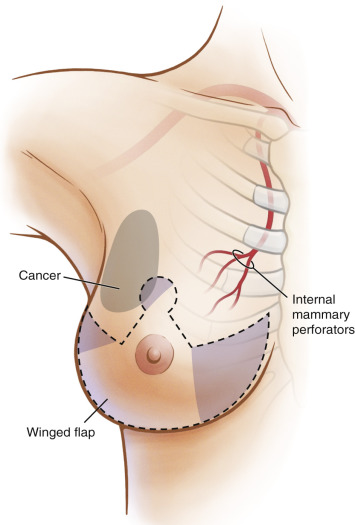
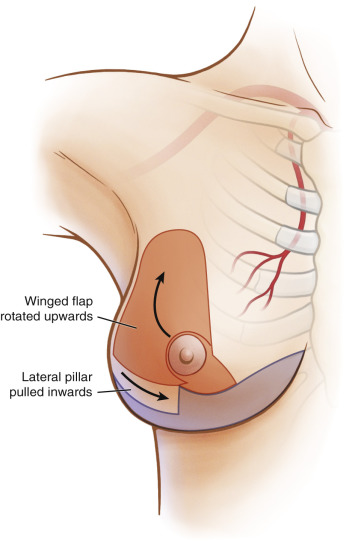
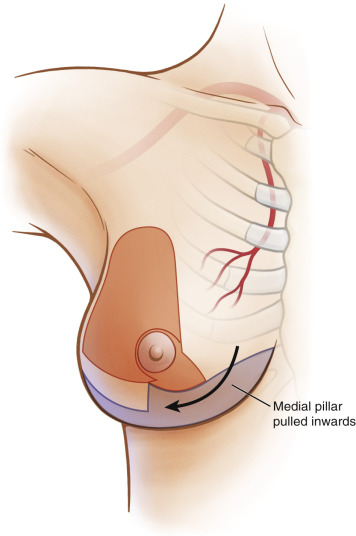
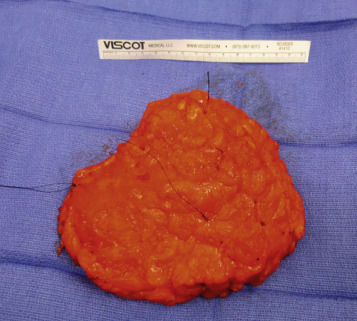
This is a 48-year-old female with large breasts with grade 2 ptosis ( Cases 17.1.1 & 17.1.2 ). Her cancer was located in the upper outer quadrant and was large even after neoadjuvant chemotherapy. The plan was to perform an extended superomedial pedicle (winged), inverted T skin incision oncoplastic reconstruction rotating the lower outer quadrant tissue into the upper outer quadrant defect after the cancer had been removed ( Cases 17.1.3–17.1.5 ). The upper outer quadrant access for the breast surgeon was facilitated using the inverted T incision that allowed the surgeon to remove the necessary large region ( Case 17.1.6 ). The partial mastectomy specimen was larger than 15 cm ( Case 17.1.7 ). The extended superomedial pedicle (winged) specimen was de-epithelialized with perfusion noted at the tip of the pedicle region in the lower outer quadrant showing punctate bright red bleeding ( Case 17.1.8 ). Autoaugmentation of the large upper outer quadrant defect was performed by tucking the extended superomedial pedicle into the upper outer quadrant and securing it in place with two or three absorbable sutures ( Case 17.1.9 ). The lateral and medial pillars were then brought in centrally as one would do in an inverted T incision closure pattern ( Case 17.1.10 ). A symmetry reduction was performed on the contralateral side ( Case 17.1.11 ). Pre- ( Case 17.1.11 ) and postoperative ( Case 17.1.12 ) comparison photographs even after radiation note good symmetry and aesthetic form.



Related posts:
 Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Fat Grafting as an Adjunct Procedure in Breast Reconstruction
Fat Grafting as an Adjunct Procedure in Breast Reconstruction
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Symmetry Procedures in Breast Reconstruction
Symmetry Procedures in Breast Reconstruction
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


