Key Words
immediate breast reconstruction, breast implants, breast tissue expanders, total submuscular coverage, implant exchange
Introduction
The rates of mastectomy and immediate breast reconstruction have increased over the past two decades, according to a number of large population-based datasets. Changes in the oncologic approach to breast cancer have contributed to increasing rates of bilateral mastectomies. Looking more closely at immediate reconstruction, the trends demonstrate increased utilization of implant-based reconstruction modalities, but a relatively constant rate of autologous reconstruction. Throughout this time, there have also been advances in breast implant technology that have significantly improved safety.
The most commonly used technique in implant-based breast reconstruction is two-stage, total submuscular coverage of the tissue expander in the subpectoral plane. The senior author (P.G.C) of this chapter has had extensive experience in this reconstructive modality and has seen an evolution in his practice over the past 20 years. The purpose of this chapter is to discuss the lessons learned and to highlight the pearls and pitfalls of how to ultimately achieve a safe, reliable, and aesthetically favorable two-stage breast reconstruction.
Indications and Contraindications
There are few absolute contraindications for two-stage implant-based breast reconstruction. The main factors limiting the ability to perform reliable reconstruction include previous radiation therapy, smoking, and morbid obesity, all of which are considered by some to be relative contraindications.
Patients with a history of radiation therapy (whether for breast-conserving therapy necessitating salvage mastectomy or mantle field radiation) must be carefully examined to determine the impact of the radiation on the soft tissues. If the skin and underlying soft tissue are relatively supple with minimal fibrosis, a two-stage approach in a subpectoral plane with total submuscular coverage can still be utilized. If, however, the skin and breast tissue have been significantly impacted by the previous radiation and the patient still desires implant-based reconstruction, using autologous tissue from a donor site to provide non-radiated coverage over the tissue expander may be the best option initially. In most cases, the latissimus dorsi is the optimum donor site for such coverage. Most importantly, a history of radiation therapy must be carefully discussed in the context of risk for postoperative complications, which is certainly increased. Managing expectations becomes very important given this increased risk.
Smoking and obesity both have the potential to impact the result and the reliability of implant-based breast reconstruction. Smoking influences mastectomy skin flap perfusion, which may already be tenuous. Obesity may hinder satisfactory aesthetic results with alloplastic materials, given the limitations in implant sizes. The risk of complications is certainly higher in this cohort overall as well. Our institutional approach is to assess these patients and discuss the risks with them. If they understand the risks, we often will proceed to surgery if they strongly desire breast reconstruction. In the setting of smoking, having total vascularized tissue coverage is even more critical, as this gives an added layer of vascularized tissue between the skin (which is tenuous) and the expander or implant.
Aside from the relative contraindications listed above, a significant comorbid profile may be the only other major relative contraindication to performing reconstruction. This is not, however, specific to total submuscular coverage in the immediate reconstruction setting and is a more generalized health risk decision point.
Preoperative Evaluation
Nearly all women who are scheduled to undergo mastectomy at Memorial Sloan Kettering Cancer Center meet with the Plastic and Reconstructive Surgery Service for a consultation on all the methods of reconstruction, including the option for no reconstruction. A detailed history of the patient is taken with a focus on current diagnosis, previous breast surgeries, and history of radiation therapy to the breast or chest wall. A full physical examination is performed, with a focus on the breast. Preoperative asymmetry between breasts is noted and discussed with the patient, as well as the grade of mammary ptosis. If previously radiated, the pliability of the tissues is assessed. Standard breast measurements are obtained, including sternal notch to nipple, nipple to inframammary fold, breast base width, and nipple–areola complex diameter. Donor sites are assessed, including the back, lower abdomen, and inner thighs. A focused discussion about ideal reconstructive modalities follows the examination.
Prior to surgery and typically after the preoperative consultation, preoperative testing is performed in accordance with the American Heart Association (AHA) and American Society of Anesthesiologists (ASA) recommendations based on age and comorbidities. Patients with significant comorbid conditions should be cleared for surgery by their primary care provider or by a cardiologist who would perform the appropriate preoperative risk assessment.
Surgical Technique
All patients are marked in the preoperative holding area on the day of surgery. The midline meridian and the inframammary fold are marked on each breast to aid the breast surgeon with regards to the inferior resection. If skin-sparing mastectomy is performed, an ellipse of skin including the nipple–areola complex is also marked. Nipple-sparing mastectomy most commonly is performed with an inferior periareolar incision and lateral extension.
Mastectomy Incision
Over the past 20 years, the placement of the skin-sparing mastectomy incision has changed significantly from an oblique incision intended to avoid any visible scar along the medial cleavage ( Fig. 11.1 ). The oblique incision made the medial dog ear difficult to correct and prevented adequate expansion of the lower pole, which is an essential component of the two-stage approach. The incision has evolved to a horizontal incision with minimal medial extension. Such an incision allows the surgeon to tailor the mastectomy flaps, often extending the incision laterally to remove excess tissue, especially in a previously ptotic breast. This maximizes the amount of lower pole skin that can be expanded without an overlying scar.
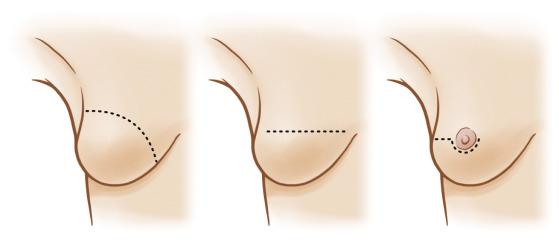
The preferred nipple-sparing mastectomy incision is a periareolar incision with lateral extension. Our institutional experience has demonstrated good exposure and lower rates of nipple and mastectomy flap necrosis with this exposure. This incision also allows better access at the time of exchange.
Mastectomy Defect
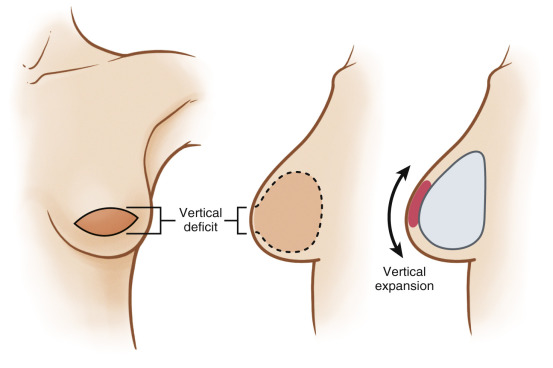
Following skin-sparing mastectomy, the skin defect is in the vertical dimension after removal of the ellipse surrounding the nipple–areola complex ( Fig. 11.2 ). As a result, the majority of the expansion, preferably with full-height expanders, is focused on this vertical deficit. Full-height expanders maximize the overall volume and skin expansion in the vertical dimension. The base width of the expander is chosen based on the patient’s breast base width, measured intraoperatively within the pocket following the mastectomy.
Tissue Expander Placement: Concepts and Operative Details
Point of Maximal Expansion
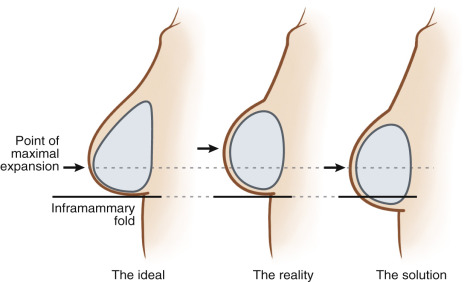
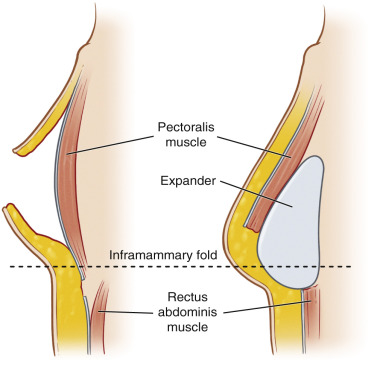
The point of maximal expansion in the reconstructed breast pocket must be in the lower third of the breast ( Fig. 11.3 ). Over the past two decades, the senior author has seen an evolution in technique to achieve this ideal point of expansion. The ideal expander would be an anatomically shaped expander, which would be placed at the inframammary fold and then expanded in the lower third of the reconstructed breast. However, in reality, this placement causes expansion at a point slightly superior to this (too high), which at the time of exchange results in a reconstruction that appears constricted in the lower third of the breast. A reason for this may be that the chest tissues tighten around the expander as volume increases in the device, and the expander assumes a more rounded shape as pressure within increases. To address this, the device is now placed more inferiorly, minimizing upper pole expansion and maximizing lower pole precise expansion. The full-height expander is placed 1–2 cm below the inframammary fold. The medial boundary is 1–2 cm from the midline, and the lateral boundary is the anterior axillary line.
Musculofascial Pocket
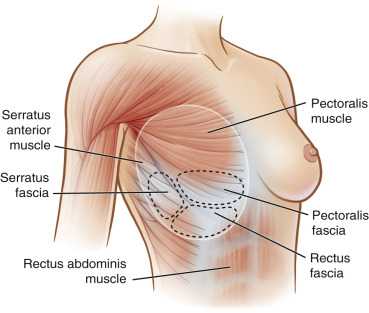
Historically, the approach to total vascularized coverage involved elevating the pectoralis major muscle medially and the entire serratus muscle laterally. This serratus muscle elevation often resulted in a painful surface area of exposed ribs for the patient and not ideally suited for sutures. This technique has now evolved from total muscular coverage to musculofascial coverage ( Fig. 11.4 ). In musculofascial coverage, the superior aspect of the pocket is defined by the entire pectoralis muscle. Laterally, only a portion of the serratus muscle with all of its fascia is raised. Inferiorly, the insertion of the pectoralis is highly variable, at times being too high on the chest wall for appropriate positioning of the implant only underneath the pectoralis and the serratus. To address this, the inferior musculofascial pocket includes rectus fascia, which is raised in continuity with the serratus fascia. This approach has two main benefits: (1) the pocket provides structural support for long-term reconstruction and (2) the vascularized layer provides a protective layer to the expander and implant. This protection may prevent loss in the event of mastectomy flap necrosis or wound breakdown.
Inferior Fasciotomy
The inferior dissection is carried out 1–2 cm below the inframammary fold to achieve adequate expansion of the lower pole ( Fig. 11.5 ). However, it was initially noted that this can be limited by a fascial band that lies across the lower pole. This compression prevents adequate expansion of the lower pole and can push the expander superiorly. To address this band, the dissection is adjusted to perform a curvilinear fasciotomy at or just below the inframammary fold. This places the expander superiorly in the submuscular plane and in the subcutaneous plane inferior to the fasciotomy. Once this fasciotomy is completed, it is important to manually assess the release to assure there are no remaining bands.
Related posts:
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Immediate Implant Breast Reconstruction – One-Stage
Immediate Implant Breast Reconstruction – One-Stage
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Immediate Prepectoral Implant Breast Reconstruction
Immediate Prepectoral Implant Breast Reconstruction
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


