Abstract
Viral infections frequently present with cutaneous manifestations, especially in children. Both viral exanthems and enanthems have a broad range of clinical findings, which may be distinctive or nonspecific. This chapter describes classic childhood exanthems, less common exanthems, eruptions associated with poxvirus infections, trichodysplasia spinulosa, and the cutaneous manifestations of hepatitis A, B, and C viral infections. Kawasaki disease, which features a polymorphic exanthem together with other mucocutaneous findings and systemic features that can mimic a viral syndrome, is also reviewed.
Keywords
viral exanthem, enterovirus, coxsackievirus, hand-foot-and-mouth disease, herpangina, measles, rubella, erythema infectiosum, papular-purpuric gloves and socks syndrome, roseola infantum, unilateral laterothoracic exanthem, Gianotti–Crosti syndrome, poxvirus, molluscum contagiosum, smallpox, dengue, viral hemorrhagic fevers, West Nile virus, Zika virus, Chikungunya fever, hepatitis B virus, hepatitis C virus, trichodysplasia spinulosa, Kawasaki disease
Introduction
Viral infections are frequently associated with cutaneous manifestations, especially in children, in whom they are the most common cause of exanthems. An exanthem is defined as a skin eruption occurring as a sign of a general disease. Viral exanthems may present with distinctive cutaneous features or in an entirely nonspecific fashion, and at times they may pose a significant diagnostic challenge, even to the most astute clinician . While dermatologists are most likely to be consulted for atypical or less widely recognized exanthems, a solid working knowledge of the classic disorders, whether common (e.g. roseola) or rare in high-income countries (e.g. measles), is essential .
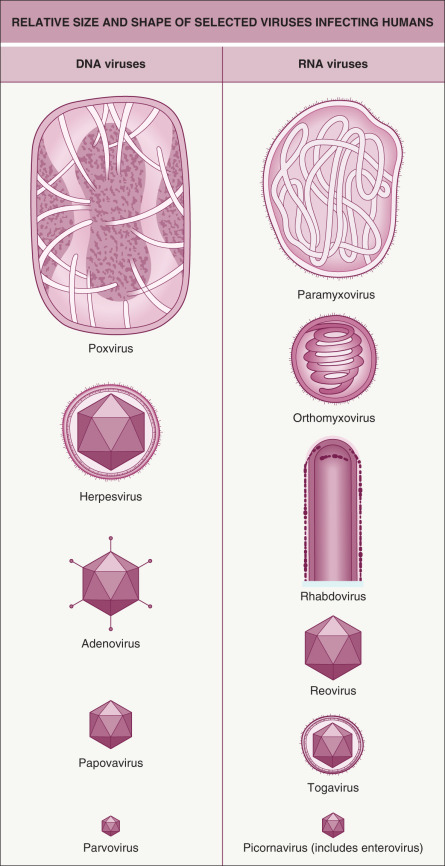
This chapter describes classic childhood exanthems, less common exanthems, eruptions associated with poxvirus infections, and the cutaneous manifestations of hepatitis A, B, and C viral infections. Kawasaki disease, which features a polymorphic exanthem together with other mucocutaneous findings and systemic manifestations that can mimic a viral syndrome, is also discussed. In contrast to the symptomatic management of most viral exanthems, prompt recognition and initiation of therapy for Kawasaki disease is necessary to prevent potentially life-threatening systemic complications. Herpesvirus infections, including infectious mononucleosis, are covered in Chapter 80 . Structural features and sizes of major types of viruses that infect humans are shown in Fig. 81.1 .
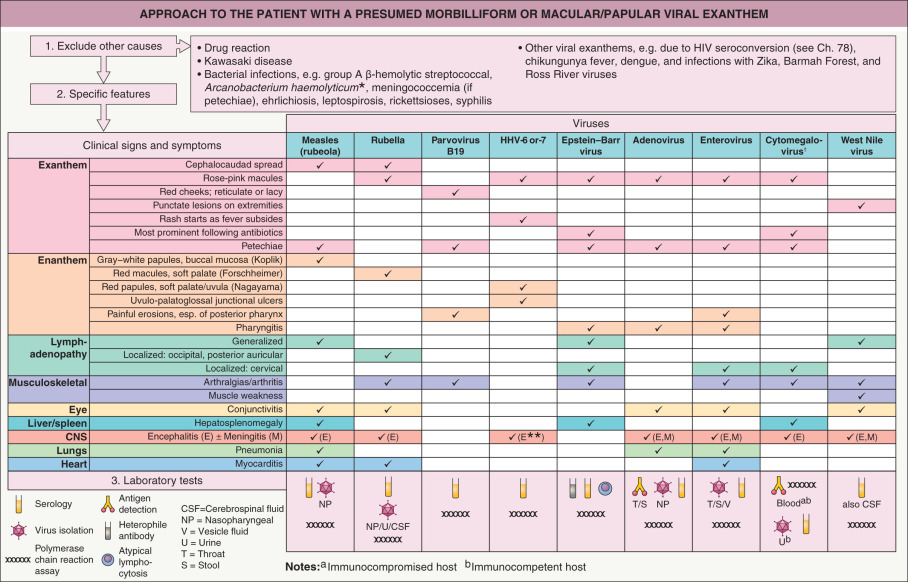
Nonspecific viral exanthems are the most common type of exanthem seen in children. These eruptions lack distinctive features such as specific lesional morphologies, distribution patterns, natural histories, or enanthems (eruption on the mucous membranes). They most often present with blanchable erythematous papules and macules in a widespread distribution on the trunk and extremities, and less often the face. Associated symptoms such as a low-grade fever, myalgias, headache, rhinorrhea, or gastrointestinal complaints may be present. Although multiple infectious agents can cause such exanthems, the most common etiologies in children are the non-polio enteroviruses (see below) in the summer/fall and respiratory viruses such as adenovirus, parainfluenza virus, and respiratory syncytial virus in the winter. Nonspecific exanthems tend to be self-limited, with spontaneous resolution within 1 week, and supportive therapy is usually sufficient. While identification of the exact etiologic agent would be desirable, in many instances it is neither necessary nor clinically feasible. Fig. 81.2 outlines the clinical features to be considered when evaluating the patient with a morbilliform (“maculopapular” or “ measles-like ” ) viral exanthem, highlighting similar and different aspects of various etiologies. Diagnostic considerations in patients presenting with fever and a “rash” are listed in Fig. 0.12 .
Enterovirus Infections
- ▪
Most common in summer and fall
- ▪
Exanthems include erythematous, vesicular, and petechial types
- ▪
Meningitis and encephalitis possible
Introduction
The enteroviruses, a subgroup of the picornavirus family, cause a wide array of illnesses associated with exanthems. The non-polio enteroviruses include echoviruses and coxsackievirus types A and B, with >100 genetically distinct types that infect humans. These viruses consist of a single-stranded RNA genome with an unenveloped capsid.
Epidemiology
Enteroviral infections occur worldwide and are usually transmitted human-to-human via fecal–oral or respiratory routes, usually with a 3–6-day incubation period. They can also be spread from mother to infant in the peripartum period. Exposure to virus in fecally contaminated water in swimming pools or via ingestion of oysters may be responsible for some infections. Clinical attack rates are highest in young children, and infections occur more frequently in lower socioeconomic groups. In temperate climates, infections are most common in the summer and fall. However, coxsackievirus A6 outbreaks frequently affect adults and can occur in the winter.
Pathogenesis
Enteroviruses infect epithelial surfaces of the pharynx and lower alimentary tract. They then replicate in lymphoid tissues and disseminate via an initial minor viremia. Subsequently, replication may occur at multiple anatomic sites, including the CNS, heart, liver, adrenals, respiratory tract, skin, and mucous membranes . This replication correlates with the appearance of clinical symptoms. A major viremia occurs during the period of viral multiplication in the secondary infection sites.
Clinical Features and Differential Diagnosis
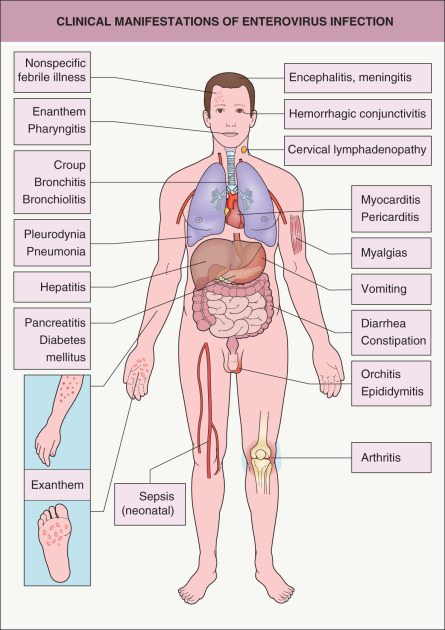
Fig. 81.3 depicts the potential clinical manifestations of an enteroviral infection.
The most distinctive exanthematous illness due to enteroviruses is hand-foot-and-mouth disease (HFMD). This disorder is characterized by a vesicular eruption on the palms and soles ( Fig. 81.4A ) in conjunction with an erosive stomatitis. The dorsal aspect of the hands and feet may be involved as well as the buttocks and perineum; oral lesions are most common on the tongue, buccal mucosa, palate, uvula, and anterior tonsillar pillars. Onychomadesis occasionally occurs 1–2 months after HFMD as a consequence of temporary nail matrix arrest related to the viral infection .

Patients with HFMD often present with fever and malaise, and they may have a mild prodrome prior to the onset of the exanthem. Numerous coxsackievirus serotypes have been implicated, most commonly type A16; in addition, type A10 represents a major cause of recent outbreaks in Europe and Asia. Although HFMD generally runs a benign and self-limited course, since 1998 there have been multiple epidemics of severe enterovirus 71 infection, primarily in the Asia-Pacific region, which have resulted in cardiopulmonary and neurologic complications and even deaths in affected young children .
Globally beginning in 2008 and since 2011 in the US, coxsackievirus A6 (CVA6) has emerged as a cause of both outbreaks and sporadic cases of severe and atypical HFMD . This variant is characterized by more widespread vesicular, papulovesicular, and sometimes bullous or petechial eruptions, frequently involving the perioral area, extremities and trunk, as well as the palms, soles, and buttocks ( Fig. 81.4B–G ). Oral lesions develop in approximately half of patients, and delayed acral desquamation and onychomadesis are common . The eruption may be accentuated in areas of pre-existing skin injury or eczematous dermatitis, with the latter referred to as “eczema coxsackium” (see Fig. 81.4F ). The differential diagnosis may include eczema herpeticum, varicella, disseminated zoster, Gianotti–Crosti syndrome, erythema multiforme, and autoimmune bullous diseases. In addition, patients with HFMD due to CVA6 are often febrile but do not usually have neurologic or other complications.
Herpangina is a febrile illness, primarily in children 3–10 years of age, characterized by painful vesicles and erosions on the soft palate, uvula, tonsils, pharynx, and buccal mucosa. An exanthem is usually absent. Coxsackievirus groups A and B, as well as echoviruses, are the usual pathogens.
In addition to HFMD and herpangina, enteroviruses cause a diverse spectrum of exanthems that may be morbilliform, rubelliform, roseola-like, urticarial, scarlatiniform, vesicular, pustular, and/or petechial. The majority of enteroviral exanthems feature erythematous macules and papules in a widespread distribution. Petechiae are fairly common, especially with echovirus 9 infection, and may lead to consideration of a more serious infection such as meningococcemia. Non-polio enteroviruses often infect newborns, producing a nonspecific erythematous exanthem and additional features such as fever, gastroenteritis, hepatitis, pneumonia, and meningoencephalitis .
In 1969, Cherry et al. described four children with echovirus 25 or 32 infection who had fever and transient, spontaneously resolving, vascular papules; histologically, dilated blood vessels were seen. The term eruptive pseudoangiomatosis was subsequently proposed, and >100 additional cases have been reported in adults as well as children, with occasional documentation of an underlying infection with an enterovirus or, less often, cytomegalovirus (CMV) or Epstein–Barr virus (EBV).
While classic HFMD and herpangina are fairly straightforward clinical diagnoses, other less specific exanthematous illnesses due to enteroviruses may have a broad differential diagnosis. Important factors that may point to the etiology include the season, exposure history, geographic location, and clinical signs and symptoms.
Confirmation of an enteroviral infection may be accomplished via viral culture, which has low sensitivity (especially for CVA6) , or reverse transcription polymerase chain reaction (RT-PCR)-based assays; determination of the specific type of enterovirus via gene sequencing following RT-PCR is currently done only at research and public health laboratories (e.g. the US Centers for Disease Control [CDC]). Viral testing can be performed from vesicular fluid (preferred for HFMD), throat swabs, stool samples, and cerebrospinal fluid (CSF). Serologic diagnosis is difficult due to the large number of different serotypes and the time delay, which make it clinically less useful. Table 81.1 lists types of serologic assays.
| SEROLOGIC ASSAYS OF ANTIBODY RESPONSES | |
|---|---|
| Assay | Principle |
| Neutralization | Visual read of infected cell monolayers incubated with test sera, looking for CPE inhibition |
| Radioimmunoassay (RIA) | Ab and Ag bind, then radiolabeled antiglobulin added, or radiolabeled Ag added and it binds Ab; radioactivity measured |
| Enzyme-linked immunosorbent assay (ELISA) | Microplates coated with Ag, serum and enzyme-labeled antiglobulin added, then enzyme substrate added and color change measured |
| Western blot | Ag mixture separated by electrophoresis, transferred to membrane, serum added and then labeled antiglobulin; seen as colored bands |
| Latex agglutination | Ag-coated latex particles incubated with serum, Ab agglutinates particles |
| Hemagglutination inhibition (HI) | Serially diluted test sera mixed with viral Ag, then animal erythrocytes added; inhibition of agglutination measured |
| Complement fixation | Ag added to serially diluted test sera; Ag–Ab complex binds complement, so the latter is unavailable for lysis of sheep erythrocytes in the presence of Ab to erythrocytes |
| Immunodiffusion | Ab and soluble Ags combine to produce visible lines of precipitate in a gel |
| Immunofluorescence | Test sera added to infected cell monolayer, then fluorescein-labeled anti-IgG Ab added; examined with fluorescence microscope |
Pathology
Skin biopsy is generally not a useful diagnostic procedure in enteroviral infections. Histopathologic features of the vesicular lesions of HFMD include epidermal necrosis with intraepidermal vesicles, a lack of inclusion bodies or multinucleation, and a nonspecific dermal inflammatory infiltrate.
Treatment
For most enteroviral exanthems, the course is self-limited, the prognosis is excellent, and supportive care suffices. However, in certain patient populations, e.g. immunosuppressed individuals or neonates, an enteroviral infection may be associated with potentially life-threatening complications. Pleconaril, a drug that interferes with enterovirus attachment and uncoating by binding to the protein capsid, has been demonstrated to be effective both in vitro and in clinical studies, including a recent randomized, placebo-controlled trial in neonates with enteroviral sepsis ; it therefore holds promise as a specific antiviral therapy for serious enteroviral infections . Two inactivated enterovirus-71 vaccines are licensed for clinical use in China, and other enteroviral vaccines are under development.
Measles
▪ Rubeola
- ▪
Incidence greatly decreased with vaccination
- ▪
Prodrome of cough, coryza, conjunctivitis, and Koplik spots
- ▪
Cephalocaudad spread of exanthem
Introduction and History
The incidence of measles has markedly decreased since the introduction of the live vaccine in 1963. Despite high vaccination coverage, measles outbreaks continue to occur in both high-income and low-income countries, and the disease is still regarded as a major health burden. Use of the vaccine is estimated to have reduced global measles morbidity and mortality by 74% and 85%, respectively, compared with the prevaccine era .
Epidemiology
The incubation period of measles, which is highly contagious and spread via respiratory droplets, is 10–14 days. In the prevaccine era, measles was endemic throughout the year in heavily populated areas, without regard to age or gender. During the 1989–1990 epidemic, reported measles cases in the US increased six- to ninefold over the mean of 3000 cases diagnosed annually between 1985 and 1988. Target populations during that epidemic were unvaccinated children younger than 5 years of age and vaccinated school-aged children who failed to develop immunity against the virus. The latter highlighted the need for more than one dose of vaccine; as a result, a two-dose measles vaccine schedule was recommended in 1989, which greatly decreased the incidence of measles in the US . Although the median number of cases of measles diagnosed annually in the US is now ~50, outbreaks still occur; for example, 147 individuals developed measles from December of 2014 to early 2015 following an initial exposure at a popular amusement park in California . Such observations underscore the importance of sustained efforts at universal vaccination against measles.
Pathogenesis
Measles is caused by an RNA virus in the Paramyxoviridae family, and humans are the natural host and reservoir of infection. The disease starts with replication of the virus within the epithelial cells of the respiratory tract, with subsequent spread to the lymphoid tissue and blood, resulting in viremia. The virus can then disseminate to internal organs, including the lungs, liver, and gastrointestinal tract.
Clinical Features and Differential Diagnosis
Measles classically presents with a prodrome of fever, cough, nasal congestion, and rhinoconjunctivitis. A pathognomonic enanthem, Koplik spots, appears during the prodrome and is composed of gray–white papules on the buccal mucosa. The exanthem develops over 2–4 days and consists of erythematous macules and papules that begin on the forehead, hairline, and behind the ears and then spread in a cephalocaudad direction ( Fig. 81.5 ). On the fifth day, the exanthem starts to fade in the same order as it appeared.

Morbilliform (“measles-like”) eruptions can result from other viral infections, e.g. with enteroviruses, EBV, parvovirus B19, and human herpesvirus-6 (HHV-6) . The differential diagnosis may also include a drug eruption and Kawasaki disease (see Fig. 81.2 ).
Atypical measles due to infection with wild-type virus in the setting of partial immunity has been reported in several groups, including recipients of killed measles vaccine (used from 1963 to 1968), those who failed vaccination, and immunocompromised individuals. It is characterized by high fevers, cough, and pulmonary infiltrates that reflect immune complex deposition related to non-protective, complement-fixing antibodies. Coryza and conjunctivitis are generally absent, and the exanthem is variable, potentially including vesicles, petechiae, purpura, and acral edema.
Complications of measles include otitis, pneumonia, encephalitis, and myocarditis. Subacute sclerosing panencephalitis is a delayed neurodegenerative disorder that can occur as a complication of measles many years after the acute disease. It is characterized by seizures, personality changes, coma, and death. Laboratory diagnosis of measles can be accomplished by virus isolation or detection via RT-PCR in nasopharyngeal secretions or urine, as well as serologic assays for measles-specific antibodies (IgM or IgG).
Pathology
The histopathologic findings are nonspecific, including a superficial perivascular lymphocytic infiltrate together with variable spongiosis and dyskeratosis.
Treatment
There is no specific antiviral therapy for measles. Because low serum vitamin A levels are associated with increased measles-related morbidity and mortality, the World Health Organization (WHO) recommends that all children with acute measles receive vitamin A once daily for 2 days at the following doses: 200 000 IU if age ≥12 months; 100 000 IU if age 6–11 months; or 50 000 IU if age <6 months.
Prevention of measles by vaccination is the most effective way to reduce measles morbidity and mortality. The current recommendation for measles immunization is an initial vaccine dose at 12–15 months of age and a second dose at 4–6 years of age . For unvaccinated individuals exposed to measles, administration of the vaccine within 3 days or intramuscular or intravenous immunoglobulin (IM/IVIg) within 6 days of the exposure may provide some protection.
Rubella
▪ German measles
- ▪
Exanthem of rose-pink macules with cephalocaudad spread
- ▪
Tender lymphadenopathy, especially occipital and posterior auricular
- ▪
Joint involvement common
- ▪
Fetal infection is associated with congenital anomalies
Introduction and History
Rubella is caused by an RNA virus in the Togaviridae family. Although usually a mild, self-limited disease in children and adults, it can cause major complications when transmitted to a fetus in utero , including miscarriage, stillbirth, and severe congenital malformations.
Epidemiology
The disease is spread via respiratory droplets, with an incubation period of 16–18 days. The incidence of rubella has markedly declined since the licensure of the MMR vaccine in 1969. For example, in the US, the incidence of rubella has declined by more than 98%, with <15 cases reported to the CDC annually in the past decade. Rubella has a worldwide distribution and occurs most often in the spring.
Pathogenesis
The primary site of infection is the nasopharynx, followed by spread to regional lymph nodes and a subsequent viremia.
Clinical Features and Differential Diagnosis
Rubella typically presents with a mild prodrome that includes fever, headache, and upper respiratory symptoms. In children, many cases are subclinical. One to 5 days following the prodrome, an eruption of erythematous macules and papules appears on the face, spreading in a cephalocaudad direction. Erythematous petechial macules may also be present on the soft palate (Forchheimer spots). The eruption is often accompanied by tender lymphadenopathy, especially of the occipital, posterior auricular, and cervical regions. The cutaneous eruption tends to fade in 2–3 days in the same order as it appeared.
Rubella may result in arthralgias and arthritis, especially in postpubertal girls and women; less frequent complications include hepatitis, myocarditis, pericarditis, hemolytic anemia, and thrombocytopenia. Encephalitis occurs in approximately 1 in 6000 infected individuals .
Rubella can be diagnosed by detection of anti-rubella IgM antibodies or a fourfold increase in specific IgG antibodies; virus isolation or detection via RT-PCR from a nasal wash, throat swab, or urine sample is also possible. The exanthem of rubella is nonspecific and the differential diagnosis includes other viral exanthems (e.g. adenovirus, enterovirus, measles, EBV) and toxin-mediated eruptions such as scarlet fever. The occipital lymphadenopathy and the typical progression of the eruption can be helpful in diagnosing the disease.
Congenital rubella occurs when a nonimmune pregnant woman transfers the virus to the fetus. Birth defects are most commonly observed when infection is during the first 16 weeks of pregnancy. Congenital rubella syndrome is characterized by cataracts, deafness, congenital heart defects (patent ductus arteriosus, ventricular septal defects), and CNS abnormalities (microcephaly, developmental delay). A “blueberry muffin baby” presentation due to dermal hematopoiesis is occasionally observed (see Ch. 121 ).
Pathology
Reported histopathologic findings include a superficial perivascular infiltrate with mild spongiosis. Atypical lymphocytes may be evident in the cutaneous infiltrate as well as in peripheral blood.
Treatment
Treatment of rubella is supportive. The current recommended immunization schedule for rubella vaccine, which is given in conjunction with the measles and mumps vaccines (MMR vaccine), is an initial dose at 12–15 months and a second dose at 4–6 years . In a pregnant woman who has been exposed to rubella, serologic testing (IgG and IgM) should be performed. Prophylaxis via administration of IM/IVIg to rubella-susceptible women exposed to confirmed rubella early in pregnancy may be considered, but it does not reliably prevent fetal infection. If rubella-specific IgM antibodies or a diagnostic rise in IgG anti-rubella antibodies (the latter not useful following IM/IVIg administration) are detected, the patient should be offered prenatal counseling.
Erythema Infectiosum
▪ Fifth disease ▪ “Slapped cheek” disease ▪ Parvovirus B19 infection
- ▪
“Slapped cheeks” followed by lacy extremity-predominant eruption, especially in children
- ▪
Eruptions in adolescents and adults may be petechial and/or have an acral or periflexural distribution
- ▪
Marked affinity of parvovirus B19 for erythrocyte precursors
- ▪
Fetal infection may result in anemia, fetal hydrops, or death
Introduction and History
Human parvovirus B19 (B19), the only parvovirus known to infect humans, was accidentally discovered in 1975 by Cossart and colleagues, who were screening blood samples for hepatitis B virus. The small, single-stranded DNA virus, which was named after the panel of sera in which it was found (number 19, row B), was identified as the etiology of erythema infectiosum in 1983. Subsequent elucidation of the pathogenesis of human B19 infections has led to its association with a wide variety of clinical findings ( Table 81.2 ).
| PARVOVIRUS B19 CLINICAL ASSOCIATIONS |
| Established associations |
| Mucocutaneous |
|
| Extracutaneous |
|
| Possible associations |
| Vasculitides |
|
| Additional exanthems |
|
| Other |
|
* Patients suffering from decreased red cell production (e.g. iron deficiency, thalassemias) or increased red cell destruction (e.g. sickle cell anemia, hereditary spherocytosis, pyruvate kinase deficiency, glucose-6-phosphate dehydrogenase deficiency), as well as patients with HIV infection and recipients of allogeneic hematopoietic stem cell or solid organ transplants.
Epidemiology
Infection with B19 occurs in a seasonal pattern, with a peak incidence of erythema infectiosum during the winter and spring. Transmission is via respiratory secretions, blood products, and vertically from mother to fetus; the incubation period is between 4 and 14 days. B19 infection occurs worldwide and is most common in school-aged children. A cyclical pattern of epidemics seems to have peaks about every 6 years , and individual community epidemics last 3–6 months. The seroprevalence of B19 antibodies increases in direct proportion with age, with immunity in 2–15% of children 1–5 years of age, 15–60% of those 5–19 years of age, and 30–80% of adults.
Pathogenesis
B19 has a strong tropism for erythroid progenitor cells, and the erythrocyte “P antigen” (globoside) is the cellular receptor to which the virus binds. In fact, individuals who lack the P antigen (blood group P 1 k or p phenotypes) seem to be naturally resistant to B19 infection .
After initial infection of the respiratory tract, a B19 viremia occurs, ending when the anti-B19 IgM antibody appears ~8–10 days post inoculation ( Fig. 81.6 ). During the viremic period, reticulocytopenia occurs for 7–10 days . One week after the appearance of IgM antibody, anti-B19 IgG appears and coincides with the appearance of the rash and arthralgia. An immune-mediated process is suggested by the temporal disconnect between the viremia and the clinical symptoms.
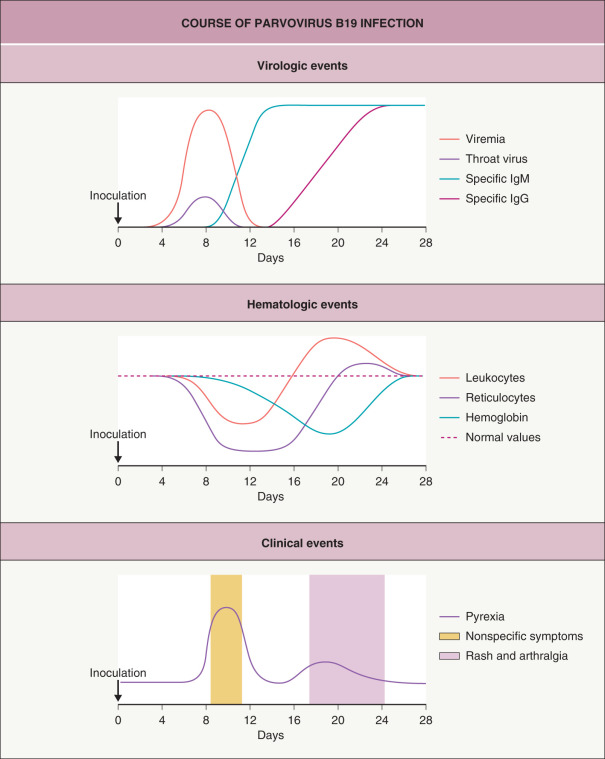
The anemia and reticulocytopenia tend to be inconsequential in the normal host but may result in transient aplastic crises in at-risk individuals, such as those with disorders resulting in enhanced red blood cell destruction or decreased production; thrombocytopenia, neutropenia, and pancytopenia may also occur (see Table 81.2 ). Fetal infection from intrauterine virus transmission causes fetal anemia of varying severity (see below).
Clinical Features and Differential Diagnosis
The most common illness caused by B19 infection is erythema infectiosum, which most often occurs in children 4–10 years of age. Mild prodromal symptoms such as a low-grade fever, myalgias, and headache may develop 7–10 days before the characteristic exanthem appears. The initial stage of the exanthem consists of bright red macular erythema of the cheeks, with sparing of the nasal bridge and circumoral regions ( Fig. 81.7A ). One to 4 days later, the second stage appears as erythematous macules and papules on the extremities and to a lesser extent the trunk, progressing to form a lacy, reticulated pattern ( Fig. 81.7B,C ). This exanthem typically lasts 1–3 weeks or occasionally longer; it fluctuates in intensity during this period, often with exacerbations upon exposure to sunlight or overheating. The differential diagnosis of erythema infectiosum may include scarlet fever, enteroviral infection, and rubella, but the diagnosis is usually straightforward when the characteristic eruption is present. Although the evanescent exanthem of systemic juvenile idiopathic arthritis (Still disease) is also accentuated by heat, it is accompanied by episodic high fevers, has a more chronic course, and often exhibits the Koebner phenomenon.

In adolescents and adults with B19 infection, the exanthems tend to be petechial and often have an acral or periflexural distribution (see Table 81.2 ) . A distinctive papular-purpuric gloves and socks syndrome (PPGSS) was first described in 1990 and subsequently found to be associated with acute B19 infection, although other infectious etiologies have also been reported, e.g. coxsackievirus B6, HHV-6, and EBV. PPGSS most often develops in the spring, and although it has a predilection for young adults, PPGSS may occur at any age, including in children. The hallmark findings are edema and erythema of the hands and feet, especially the palms and soles, in association with petechiae and purpura ( Fig. 81.8 ). Occasionally, there is extension onto the dorsal surfaces of the hands and feet, and patients may complain of burning and pruritus. Additional manifestations can include an enanthem of erosions and petechiae involving the palate, pharynx, and tongue, as well as fever and mild prodromal symptoms.

Therapy of PPGSS is symptomatic, and spontaneous resolution usually occurs over 1–2 weeks. Although few studies have addressed the immune response in PPGSS, based on limited data it appears that patients develop the mucocutaneous lesions while still viremic, which implies contagiousness and therefore has different epidemiologic implications than the classic eruption of erythema infectiosum.
Arthralgia or arthritis occurs in up to 10% of patients with erythema infectiosum and is usually self-limited, typically resolving in 1–3 weeks but sometimes lasting for months. It tends to affect the small joints of the hands as well as the wrists, knees, and ankles. Joint involvement related to B19 infection is more common in adults, especially women, occurring in up to 30–60% of those with acute infection . Arthropathy may be seen without an accompanying exanthem.
The manifestations of fetal B19 infection range from self-limited anemia to hydrops, spontaneous miscarriage, or stillbirth. The greatest susceptibility is associated with infections acquired before 20 weeks’ gestation, and most fetal losses occur between 20 and 28 weeks’ gestation. Third-trimester fetal demise may also occur, but it is less often associated with fetal hydrops . The overall risk of fetal loss in the setting of acute B19 infection during pregnancy is only 2–6% , and the majority of infants born to B19-infected mothers are delivered asymptomatic at term. There is no evidence for long-term neurodevelopmental sequelae for surviving infected infants, and congenital malformations have not been conclusively demonstrated.
When diagnostic confirmation of B19 infection is needed, detection of serum anti-B19 IgM antibody is the preferred method, and its presence indicates infection within the previous 2–4 months. PCR-based assays may be helpful in diagnosing infection in immunocompromised patients.
Pathology
Skin biopsy is generally not useful in the diagnosis of B19 infection. In patients with PPGSS, histologic evaluation demonstrates a lymphocytic dermal infiltrate with frequent extravasation of erythrocytes. Anti-B19 antibodies can highlight infected endothelial cells in superficial dermal blood vessels.
Treatment
No specific antiviral therapy is available for B19 infections. Children with erythema infectiosum usually feel well and often require no treatment. NSAIDs are useful if symptomatic arthropathy is present. Patients who develop an aplastic crisis may require red blood cell transfusions. Pregnant women with confirmed primary B19 infection during the first two trimesters should undergo serial fetal ultrasonography, and management of severely affected fetuses is possible with in utero transfusions and other interventions.
Roseola Infantum
▪ Exanthem subitum ▪ Sixth disease
- ▪
High fever followed by an exanthem at defervescence
- ▪
Affects primarily infants and toddlers
- ▪
Febrile seizures possible
The characteristic presentation is a high fever (to 40–40.5°C; 104–105°F) for 3–5 days in an infant who otherwise appears well. Seizures occur during the febrile period in up to 10% of patients. Defervescence is accompanied by the appearance of rose-pink macules and papules on the trunk, neck, proximal extremities, and occasionally the face. Mild upper respiratory symptoms, injection of the tympanic membranes, cervical or occipital lymphadenopathy, edematous eyelids, and a bulging anterior fontanelle may also be present. An enanthem of red papules on the soft palate and uvula (Nagayama spots) can develop, and uvular and palatoglossal junctional ulcers represent a characteristic finding . The skin eruption typically fades over a few days. Nonspecific fevers with or without otitis media in infants may also be due to HHV-6 infection.
Additional pathogenic features and clinical manifestations of HHV-6 infection, including reactivation in the settings of immunosuppression and drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, are discussed in Chapter 80 .
Unilateral Laterothoracic Exanthem
▪ Asymmetric periflexural exanthem of childhood
- ▪
Initial unilateral distribution, most often affecting the axilla and lateral trunk
- ▪
Subsequent generalization, but maintains unilateral predominance
- ▪
Spontaneous resolution over 3–6 weeks
- ▪
Presumed to be viral in etiology, although exact cause unknown
Introduction and History
This disorder was first described in 1962 , and the term “unilateral laterothoracic exanthem” (ULTE) was introduced in 1992 . ULTE is initially characterized by a unilateral periflexural (often axillary) location, with spread in a centrifugal pattern to the contralateral side over time.
Epidemiology
ULTE occurs most commonly in toddlers and preschool-aged children, with an age range of 6 months to 10 years. The male : female ratio is 1 : 2, and most reported patients have been Caucasian. The condition is widespread in Europe and North America, and the majority of cases occur in the spring.
Pathogenesis
The etiology of ULTE remains unknown despite multiple attempts to identify a causative infectious agent. The seasonal pattern, associated prodrome, reports of familial cases, and lack of response to systemic antibiotics suggest a viral etiology. In studies in which screening for multiple viruses (e.g. EBV, CMV, HHV-6, HHV-7) was performed, no etiologic agent has been consistently demonstrated. A relationship to infection with Spiroplasma , parvovirus B19, and EBV has been noted in individual cases .
Clinical Features and Differential Diagnosis
The eruption typically begins with a unilateral distribution ( Fig. 81.9 ), most commonly in the axillary region, followed in frequency by the trunk, arm, and thigh. It is usually morbilliform or eczematous in nature and tends to spread to contralateral areas while maintaining a unilateral predominance.

The exanthem may be preceded by a low-grade fever, diarrhea, and/or rhinitis in up to 60% of patients, and pruritus is common. Lymphadenopathy may also be present. The eruption typically lasts 3–6 weeks and then resolves spontaneously, usually without recurrence.
Contact dermatitis is often initially suspected, and the differential diagnosis also includes a nonspecific viral exanthem, a drug eruption, atypical pityriasis rosea, scabies, miliaria, and tinea corporis. If there is prominent involvement of the extremities, Gianotti–Crosti syndrome may also be considered. An eczematous eruption with a distribution pattern similar to ULTE can occur in association with mollusca contagiosa located in the same areas. Laboratory evaluation is generally unnecessary.
Pathology
Histologic features are nonspecific and include mild spongiosis, exocytosis of lymphocytes into the epidermis, and a superficial perivascular infiltrate that is predominantly lymphocytic. The dermal infiltrate may be accentuated around eccrine ducts.
Treatment
Supportive treatment is indicated in symptomatic patients, although topical corticosteroids tend to be of little help. Parents should be reassured that the exanthem will resolve spontaneously in about 3–6 weeks.
Gianotti–Crosti Syndrome
▪ Papular acrodermatitis of childhood ▪ Papulovesicular acrolocated syndrome
- ▪
Symmetric papular eruption on the extremities, face, and buttocks
- ▪
EBV and globally hepatitis B virus represent the most common triggers
Introduction and History
Gianotti–Crosti syndrome (GCS) was first described by Gianotti and Crosti in the 1950s. This childhood condition is characterized by the acute onset of a symmetric papular eruption on the face, extremities, and buttocks. In 1964, Gianotti and Crosti reported coexistent anicteric hepatitis, and in the 1970s an association with hepatitis B virus was described. Subsequent reports demonstrated that GCS can result from a variety of viral triggers ( Table 81.3 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


