Introduction
The secret of a beautiful face lies behind a well-balanced proportion of facial features and is a composite of all of the anatomical elements, including skin, subcutaneous tissues, muscle, bone, and teeth. Facial plastic surgeons strive daily with the achievement of this harmonious balance.
Dentofacial deformities affect approximately 20% of the population, out of which 5% have major skeletal deformities . Orthodontic and surgical treatment of dentofacial deformities can produce a high degree of satisfaction for the patient and surgeon. However, presurgical treatment planning and execution remain challenging. The adage “form follows function” is applied, as a significant overlap occurs between occlusal function and facial aesthetics. Ideally the goals of orthognathic surgery should be (1) to correct any masticatory dysfunction and establish a functional masticatory system; (2) to enhance aesthetics of the patient’s face and profile; (3) to prevent further degeneration of any mechanical problem; and (4) to stabilize the occlusion in a patient with temporomandibular joint (TMJ) disease.
Although surgery of the nose mainly involves correction of skeletal and cartilage abnormalities, aesthetic surgery on the remainder of the face is often concerned with soft tissue deformities. In many instances, surgery of the soft tissues is sufficient; however, attention must often be paid to underlying skeletal deformities to correct many congenital or traumatic reconstructive problems.
In order to achieve an aesthetic ideal, the surgeon must have a clear concept of proportion, a method to analyze deformities, and the ability to apply specific techniques to a given deformity. Evaluation of facial deformities should include skeletal and soft tissue analysis. Soft tissue analysis can be done in an unstructured way through focused observation or by careful study of consistent frontal and lateral photographs. Generally, skeletal analysis involves evaluation of the facial bones and is easier to quantify by determining the patient’s dental occlusion and through the use of cephalometric radiography.
After careful skeletal and soft tissue analysis, a detailed, systematic treatment plan is established. This involves using 3D imaging and dental and bony models, and is often the product of multidisciplinary teamwork. Surgical correction is then performed with the aim of establishing or enhancing facial harmony.
Aesthetic Facial Analysis
Dental Analysis and Occlusion
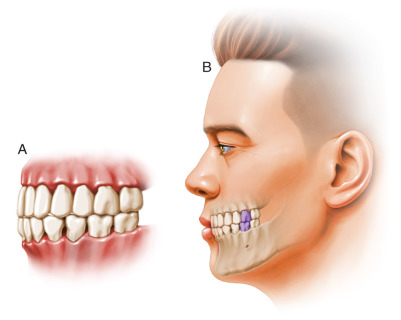
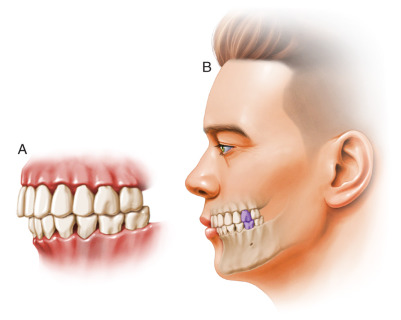
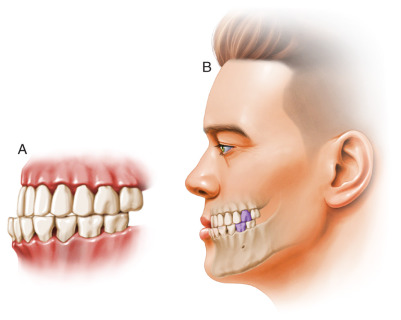
Dental analysis and treatment directly address the relationship of the maxillary and mandibular teeth. Since the introduction of the Angle classification system in 1899 , orthodontists and surgeons have used this system to describe normal and abnormal dental occlusion. The reference point in the Angle classification is the relationship of the maxillary to the mandibular first molar teeth. In class I occlusion, the mesiobuccal cusp of the first maxillary molar fits in the groove on the lateral or buccal surface of the first mandibular molar tooth ( Fig. 23.1 ). This description represents the ideal relationship of the molar teeth only. When the remainder of the teeth interdigitate perfectly, the occlusal relationship is said to be normal. However, malocclusion can exist when the molar relationship is class I. In class II malocclusion, the mesiobuccal cusp of the first maxillary molar is mesial or in front of the first mandibular molar ( Fig. 23.2 ). Class II malocclusion may arise from the lack of mandibular development or from an abnormally protuberant maxilla. The resulting posteriorly positioned mandible is termed retrognathia. Retrognathia may be associated with airway compromise in infants and obstructive apnea in adults. In class III malocclusion the mesiobuccal cusp of the first maxillary molar is positioned distal to the ideal position. This type of malocclusion is primarily skeletally based and is characterized by a large protrusive mandible (prognathism) or by an underdeveloped retrusive maxilla ( Fig. 23.3 ). Prognathism is a horizontal excess and can be present in the mandible or maxilla. With dentoskeletal deformities, the teeth are often crowded or tipped in a manner that may mask a given deformity. The patient with mandibular prognathism often exhibits a lingual tipping of the mandibular incisors. This tendency of the lip to attempt to “normalize” the situation is called a dental compensation .
In mandibular micrognathia or retrognathia, there is a decrease in horizontal growth of the mandible. This deformity often results in a “Sunday bite,” in which the patient is functioning anteriorly of centric relation. This type of bite increases the chance of TMJ disease and myofascial pain dysfunction. If the patient and physician are not aware of a Sunday bite, the treatment plan may be incorrect and result in a poorly functioning or less than optimal aesthetic result. If the mandible is in the correct position but the chin is deficient, a condition termed microgenia is present. This deformity is best treated either with bony genioplasty or chin augmentation with an alloplast.
When the maxillary and mandibular teeth do not contact, the term apertognathia or open bite is used. Apertognathia is most often secondary to vertical excess of the posterior mandible or maxilla. An open bite also may be caused by abnormal tongue habits, abnormal speech habits, or other intraoral defects. Often, patients with apertognathia have TMJ disease and have difficulty bringing their lips together. Vertical maxillary excess (VME) is a condition in which there is vertical excess of the midface. VME is often associated with excess incisor show (gummy) smile with lip incompetence . When observing a patient with VME at rest, at least two-thirds of the crown of the upper incisor is often visible ( Fig. 23.4 ).

Skeletal Analysis
Dimension and proportion are two key elements in diagnosing structural facial disharmony. Skeletal analysis demonstrates the relationship of the facial bones and illustrates any deformity in this relationship.
The cephalometric radiograph allows objective evaluation of bony and soft tissue morphology, and provides objective data that assist in the diagnosis and treatment of facial skeletal deformities. Cephalograms were originally introduced into orthodontics during the 1930s. Strikingly, it has been only until the late 1960s that this imaging tool has gained widespread acceptance for practical application .
Several methods have been developed for the production of standardized cephalometric radiographs, such as those presented by Hofrath and Broadbent in 1931 . Using a cephalostat, stabilization of the head in a fixed and reproducible position is achieved. In order to further standardize the radiograph, a consistent subject-to-film distance and x-ray target-to-subject distance must be used. The use of a soft tissue technique helps to clearly demonstrate the relationship between the soft tissues and the facial skeleton. A true lateral view, with no head rotation in the sagittal plane, is then taken. This cephalometric radiograph provides a two-dimensional outline of the lateral aspect of the craniofacial skeleton on which various analyses may be performed. To effectively use the lateral cephalometric tracing, standardized bony landmark points are used. These skeletal points allow linear and angular measurements to be performed. These measurements can be compared with normative reference values in order to quantify the skeletal abnormality.
The line connecting the nasion (N) and sella (S) is midline and is often used as the reference plane on which most cephalometric analysis is based ( Fig. 23.5 ). Angles SNA (anteroposterior position of maxilla), SNB (anteroposterior position of mandible), and ANB (difference between SNA and SNB) are relatively simple to derive and provide valuable basic information in analyzing the relationship of the maxilla and mandible to the skull base. If the angle ANB is greater than 4 degrees, a skeletal class II malocclusion is present. The maxillary versus mandibular contribution to this malocclusion may be determined by measuring the angles SNA and SNB. If ANB is greater than 4 degrees and SNA is greater than normal, the class II malocclusion is most likely secondary to maxillary protrusion. If ANB is greater than 4 degrees and SNA is less than normal, mandibular retrognathia probably exists.
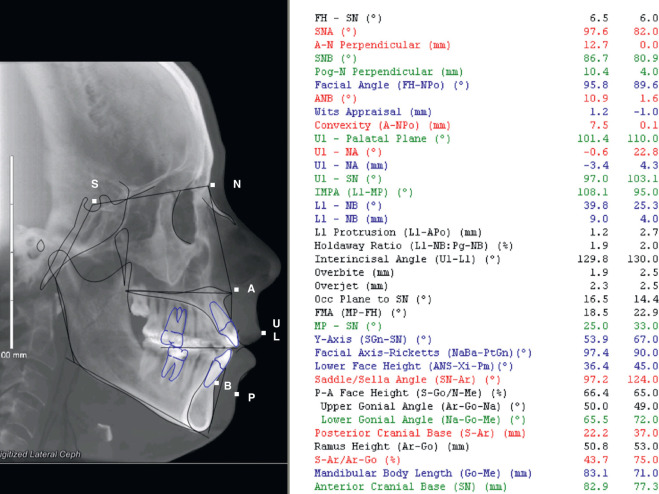
Other important angles exist ( Table 23.1 ). The Frankfort mandibular plane angle is created by the intersection of the Frankfort horizontal plane and the mandibular plane (from gonion to menton). The mandibular plane angle as defined by Tweed is the inclination of the mandibular plane . The saddle angle is the angle between the anterior and posterior cranial bases. The articular angle (S–Ar–Go) can be affected by orthodontic treatment and it is reduced in all cases of mandibular prognathism. The gonial angle (Ar–Go–Me) plays a role in growth prognosis of the mandible and is affected by the relationship between the body and the ramus of the mandible. The gonial angle indicates the direction of mandibular growth, with a large gonial angle indicating posterior condylar growth.
| Points of the Angle | Definition | Mean Value (Degrees) |
|---|---|---|
| N–S–Ar | Saddle angle | 123 |
| S–Ar–Go | Articular angle | 143 |
| Ar–Go–Me | Gonial angle | 128 |
| Ar–Go–N | Upper gonial angle | 52–55 |
| N–Go–Me | Lower gonial angle | 70–75 |
| SNA | Anteroposterior position of maxilla | 82 |
| SNB | Anteroposterior position of mandible | 80 |
| ANB | Difference between SNA and SNB | 22 |
| SN–MP | Angle between SN and mandibular plane | 35 |
| Pal–MP | Angle between palatal and mandibular plane | 25 |
| O–P | Intersecting Frankfort mandibular plane angle | 20–29 |
Various linear distances have also been described ( Table 23.2 ). These lines are measured by identifying the two connecting points on the cephalometric radiograph. The mandibular base is determined by measuring the distance between the gonion (Go) and pogonion (Pog) when projected onto the mandibular plane. The maxillary base is measured from the posterior nasal spine (PNS) to point A. The distance from the sella (S) to the nasion (N) is the anteroposterior extent of the anterior cranial base.
| Distance | Definition | Mean Value (mm) |
|---|---|---|
| S–N | Anteroposterior extent of anterior cranial base | 71 |
| S–Ar | Extent of lateral cranial base | 48 |
| S–Go | Posterior facial height | 87 |
| N–Me | Anterior facial height | 114 |
| PNS–Point A | Maxillary base | 48 |
| Go–Po | Mandibular base | 78 |
A variety of analyses using the previously mentioned skeletal points, lines, and angles have been described . In all instances, these analyses represent an attempt to describe the normal relationship of the facial skeleton.
Soft Tissue Analysis
The successful correction of dentofacial deformities also requires careful preoperative assessment of soft tissues and an accurate prediction of their response to skeletal surgery. Consequently, dental and skeletal analyses alone are inadequate in evaluating and predicting facial form.
Soft tissue analysis is the final determinant in evaluating the overall attractiveness of the face. As used by the casual observer, this method is subjective, less easily quantified, and more importantly, it can vary among different cultures and ethnic backgrounds .
Although the soft tissues are more difficult to standardize than dental or skeletal parameters, analysis may be performed by using fixed soft tissue reference points, as described in Fig. 23.5 . These points are often directly correlated with associated bony reference points, e.g., (n) soft tissue nasion correlating to the skeletal nasion (N) or (pog) soft tissue with skeletal pogonion (Pog). However, some soft tissue points are variable in location and have no associated skeletal points, e.g., the trichion (tr) or hairline. It is the variable thickness of the soft tissues such as the lips or nose and the relative position of nonfixed points such as the trichion that determine the overall facial structure and appearance.
Finally, to accurately correct facial deformities, the facial plastic surgeon must understand the amount of soft tissue change gained by a given bony alteration . The soft tissue response to skeletal surgery varies in different regions of the face. In portions of the face where the overlying soft tissues are relatively thin, larger, and more predictable, soft tissue changes are usually obtained for a given bony alteration ( Table 23.3 ). The accurate prediction of these responses determines the final aesthetic result.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


