Orbital Expansion for Anophthalmia and Microphthalmia
Brad Morrow
Rogerio I. Neves
DEFINITION
Anophthalmia, either congenital or acquired, is a rare condition in the pediatric population.
Development of the globe is critical for the stimulation of orbital and maxillofacial growth.
Anophthalmia presents a unique challenge to the reconstructive surgeon to create an aesthetic orbit, restore facial harmony, and improve the psychosocial well-being of the affected child.
Orbital expansion is a minimally invasive technique that avoids the morbidity of orbital osteotomies. In properly selected patients, accelerated orbital growth is achievable and can reverse the midface discrepancies by bone remodeling.
ANATOMY
Although the orbit is a pear-shaped cavity with a posteriorly tapering apex to the optic canal, it can be thought of as a box with four walls: medial, lateral, floor, and roof (FIG 1A).
The medial wall, composed of the ethmoid, lacrimal, maxillary, and sphenoid bones, is the thinnest section and adjacent to the ethmoid and sphenoid sinuses.
The lateral wall, composed of the zygoma and the greater wing of the sphenoid, is the thickest section and extends to the equator of the globe to protect the posterior portion, yet allow for peripheral vision. It is separated from the lesser wing of the roof by the superior orbital fissure (FIG 1B,C).
The floor, composed of the maxillary, palatine, and zygomatic bones, ends at the pterygopalatine fossa and contains the infraorbital neurovascular structures.
The roof, composed of the frontal bone and the lesser wing of the sphenoid, also forms the base of the anterior cranial fossa.
The diameter of the globe exponentially expands during the first 12 months of age.3 The rate of expansion begins to slow during 12 to 35 months of age and tapers off by 8 years of age when the diameter is approximately 96% of mature growth. Orbital dimensions and subsequent bony growth are significantly correlated with changes in globe diameter.
Based on anthropometric soft tissue measurements, Farkas et al.4 determined that approximately 90% of orbital growth occurs by 5 years of age.
PATHOGENESIS
Congenital anophthalmia occurs in the first weeks of gestation during neural tube formation when the neuroepithelium of the ventral forebrain fails to invaginate and form the optic vesicles.
Etiology
Primary genetic defect
SOX2
PAX6
CHX10
GDF6
Gestational
Rubella
Varicella
Herpes simplex virus
Cytomegalovirus
Intrauterine exposure to thalidomide
Vitamin A deficiency
Incidence
The reported incidence ranges from 0.2 to 1.5 per 10 000 births.
Acquired enucleation or evisceration after birth secondary to:
Tumor
Retinoblastoma
Choroidal melanoma
Trauma
Infection
NATURAL HISTORY
The developing globe is critical for the stimulation of orbital and maxillofacial growth.
Absence of a globe creates a three-dimensional midface hypoplasia of the skeletal, soft tissue, and adnexal structures.1,2
The resulting bony orbit is markedly reduced in volume and dimensions of the aperture.
Horizontal and vertical zygomaticomaxillary development is subsequently affected with ipsilateral deficiencies manifested as a canted occlusal plane, loss of facial width, and projection of the malar prominence.
The hypoplastic skeletal foundation creates significant soft tissue asymmetries with an inferiorly displaced eyebrow and short phimotic eyelids.
Adnexal structures are also poorly developed with contraction of the conjunctiva and fornices.
Enucleation in early childhood results in arrest of symmetric orbital growth. The severity of hypoplasia depends on the age at surgery as the orbit rapidly expands during the first 5 years of life.
Without restoration of intraorbital volume and pressure, through autologous or alloplastic material, the socket and fornices contract, which compromises the ability to wear a prosthesis.
As the infant progresses through childhood to adolescence, facial asymmetries will become more pronounced.
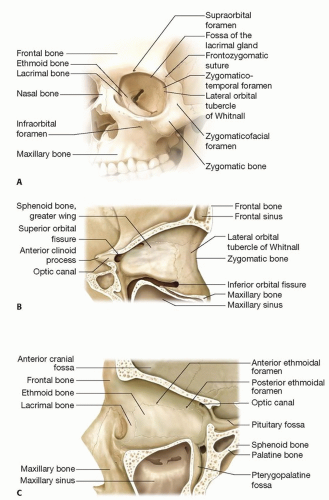 FIG 1 • A. Frontal view of the orbital bones. B,C. Lateral and medial walls of the orbit. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Anophthalmia or microphthalmia is predominantly unilateral but can be bilateral (FIG 2).
Children with severe microphthalmia may retain potential for vision, and a complete examination is critical. A pediatric ophthalmologist should assess vision, including electrodiagnostic studies.
Flash visual evoked potentials establish optic nerve dysfunction and the presence of residual vision.
Electroretinogram may identify retinal dysfunction.
In unilateral cases, the contralateral globe, lens, and optic nerve must be examined for additional anomalies such as a coloboma, cataract, glaucoma, retinal dystrophy, or optic nerve hypoplasia.
The lacrimal system may be dysfunctional ranging from canalicular stenosis to nasolacrimal duct obstruction that requires dacryocystorhinostomy.
A complete assessment of the child must be undertaken to determine the presence of associated systemic abnormalities including craniofacial, cardiac, genital, respiratory, neurologic, or metabolic.
Anophthalmia-plus syndrome includes anophthalmia, cleft lip and palate, facial clefts, and sacral neural tube defects.
IMAGING
Diagnostic imaging should be obtained to evaluate the intraorbital contents.
Ultrasound of the orbit may determine whether an ocular remnant or cyst is present. Simultaneous renal ultrasound is recommended due to the association of ophthalmic and renal anomalies.
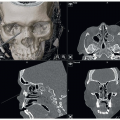
Computed tomography (CT) precisely delineates the bony anatomy but poorly defines the soft tissue structures and exposes the child to radiation. The implementation of lowdose radiation protocols has significantly lowered this theoretical risk (FIG 3).

FIG 2 • Six-month-old patient with right unilateral congenital microphthalmia.
Magnetic resonance imaging (MRI) provides superior detail of intraorbital soft tissues and intracranial visual pathways and screens for brain anomalies.
MRI has the additional advantage of avoiding radiation exposure; however, sedation is required in order to obtain a high-quality study in a young child.
DIFFERENTIAL DIAGNOSIS
Clinical congenital anophthalmia refers to a phenotypic spectrum of blindness due to a developmental defect of the globe:
Anophthalmia: the complete absence of ocular tissue
Microphthalmia: the presence of a hypoplastic, rudimentary cyst; ocular remnant; or globe
The distinction is not clinically relevant as the management does not differ and the terms are frequently interchanged.
NONOPERATIVE MANAGEMENT
Multidisciplinary team care is essential for the management of affected children and includes plastic surgery, pediatric ophthalmology, prosthetic ocularist, optometry, genetics, and social work.
In unilateral cases, vision in the contralateral unaffected eye must be protected with regular ophthalmologic examinations and safety glasses to prevent trauma.
Conventional treatment of anophthalmia is initiated in the first few weeks of life by serial placement of progressively enlarging custom-made static acrylic, glass, or silicone intraorbital and scleral conformers. Although this technique can enlarge the orbit, it is not without several limitations including the following:

FIG 3 • Follow-up CT scan showing the appropriate position of the intraorbital tissue expander.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access