Oral Cavity
OVERVIEW
Lesions involving the mucous membranes of the oral cavity may be confined to the mouth, or they may be associated with widespread cutaneous entities, or with systemic disease. Oral mucous membrane lesions often leave clues to the presence of systemic and cutaneous illnesses such as acquired immunodeficiency syndrome (AIDS), lichen planus, and systemic lupus erythematosus.
Clinical findings may also be helpful in diagnosing the following infectious diseases: measles, hand-foot-and mouth disease, and secondary syphilis. Aphthous ulcers (“canker sores”) are often seen as isolated phenomena, but they may also be an accompaniment or a precursor to a symptom complex, such as seen in Behçet syndrome or ulcerative colitis.
INFANTS, CHILDREN, AND ADULTS
Oral Mucous Cyst (Mucocele)
An oral mucous cyst (mucocele) is a common, mucus-filled, blister-like lesion, derived from the minor salivary glands. They appear most commonly in infants, young children, and young adults.
Such lesions are not true cysts; rather, they are “pseudocysts” due to the absence of a true epithelial lining. They are considered to be the result of trauma to the openings of salivary glands. An injury or rupture of these microscopic excretory ducts leads to an accumulation of mucus inside of the connective tissue of the lip. The trauma of lip biting and the sucking action of drawing the mucous membranes of the lower lip between the teeth are thought to be common causes. Patients and parents are most often not aware of having noticed any such injury.
Distinguishing Features
Most commonly occur on the inner surface of the lower lip (Fig. 9-1), but may also appear on the floor of the mouth, buccal mucosa, and tongue
Painless, sometimes bothersome, bluish or clear, glistening, dome-shaped cyst that contains mucoid material
Bluish color is due to the thin layer of epithelium that covers the capillaries. Deeper lesions are usually the same color as the rest of the lip because they are covered with a thicker layer of tissue
Easily ruptured and may spontaneously disappear, particularly in infants
May recur repeatedly
Diagnosis
Clinical
Incision and drainage reveal mucoid material
A biopsy may be performed to rule out other suspected mucosal neoplasms
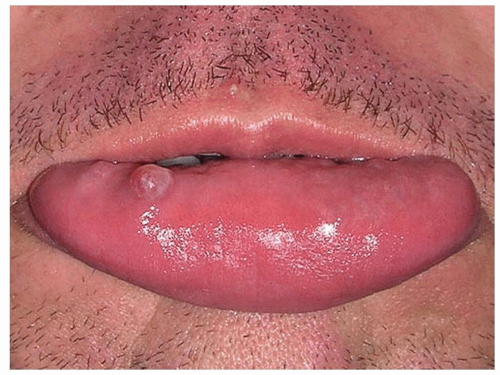 Figure 9-1 Oral mucous cyst (mucocele). Shiny, cystic papule on the labial mucosa. |
Management
Reassurance, because superficial mucoceles most often resolve spontaneously
Incision and drainage, if necessary
For frequent recurrences, or if problematic to the patient, treatment options include cryosurgery with liquid nitrogen (LN2) spray, intralesional injections of triamcinolone acetonide, or electrodesiccation
Oral surgery is the treatment of choice for deeper, recalcitrant lesions. Excision should include the immediate adjacent glandular tissue
Oral Fibroma
An oral fibroma, also referred to as traumatic fibroma, or oral polyp, is a common benign reaction to persistent long-standing irritation in the mouth. It is a very common oral neoplasm and it probably represents reactive fibrous hyperplasia due to trauma or chronic irritation.
Distinguishing Features
Asymptomatic, smooth-surfaced, firm solitary papule or nodule (Fig. 9-2)
Usually lighter in color than the surrounding normal tissue, with the surface often appearing white
Ulceration due to repeated trauma may occur
Diagnosis
Shave biopsy
Management
A shave biopsy often establishes the diagnosis and may lead to ultimate resolution
Laser ablation
Excision
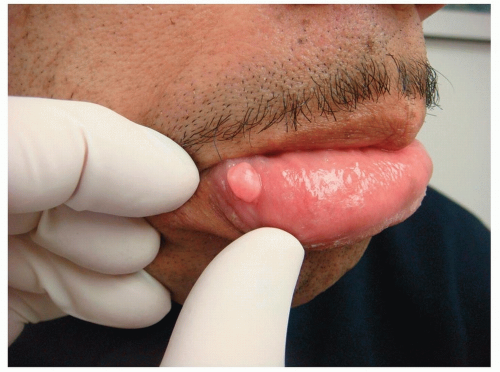 Figure 9-2 Oral fibroma. This firm papule was caused by the repetitive manipulation by this patient’s teeth. |
Aphthous Ulcers
Aphthous ulcers (aphthous stomatitis), commonly known as “canker sores,” are very common, recurrent, painful erosions or ulcers of the mucous membranes of the mouth. They occur in children and adults and appear to be more common in women than men. They have no known cause, but an immune mechanism is considered the most likely contributory factor. Patients often ascribe recurrences to psychological stress or local trauma. Women may correlate them with their menstrual cycle. Most cases heal spontaneously, only to recur unexpectedly.
Persistent or large painful, persistent aphthae may be seen in Behçet disease, inflammatory bowel disease, and human immunodeficiency virus (HIV)/AIDS.
Distinguishing Features
Painful lesions may be seen on the buccal, labial, and gingival mucosa, as well as on the tongue
Begin as vesiculobullous lesions that rarely remain intact and unruptured; instead, such lesions usually become erosions or ulcers by the time a clinician sees them
Single or multiple small (2 to 5 mm) round or oval, shallow, well-demarcated, punched-out erosions covered with gray or yellowish exudate and surrounded by a ring of erythema (halo) (Fig. 9-3)
Tend to heal in 4 to 14 days, without scarring
Diagnosis
Clinical
Management
Symptomatic therapy with topical anesthetic viscous lidocaine (Xylocaine)
Superpotent (class 1) topical steroid ointments applied directly to lesions and held in place by pressure with one’s finger. Similarly, tacrolimus 0.1% ointment (Protopic) applied at bedtime may accelerate healing
Tetracycline suspension (250 mg/tsp)—“swish and swallow”
Diphenhydramine (Benadryl) suspension—“gargle and spit”
“Magic mouthwash” is a compounded suspension composed of diphenhydramine (Benadryl), viscous lidocaine, magnesium hydroxide/aluminum hydroxide, and corticosteroids. It can be used every 4 to 6 hours for symptomatic relief
Silver nitrate applied directly to lesions also can promote healing (Fig. 9-4)
Intralesional corticosteroid injections or a brief course of systemic corticosteroids are effective in reducing pain and healing. This is particularly useful in patients with large, persistent, painful ulcers
In severe cases, consider oral colchicine, dapsone, and thalidomide
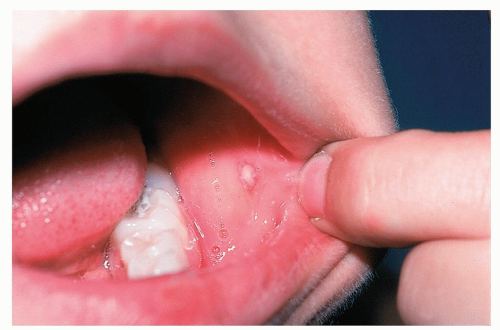 Figure 9-3 Aphthous ulcer. Small punched-out erosion with a bright red halo is present on the buccal mucosa. |
Primary Herpes Gingivostomatosis
Primary herpes gingivostomatosis occurs mainly in infants and young children, often subclinically. Most often the primary infection is mild and unnoticed, but it can be severe.
Distinguishing Features
Initially presents with mouth pain, excessive drooling, irritability, and a child not wanting to eat or drink
Fever, which may be high, with malaise, and restlessness
Lesions present as painful vesicles on an erythematous base that rapidly evolve into shallow ulcers on the palate, tongue, or gingivae (Fig. 9-5)
Gums may be red, swollen, bleed easily, and regional lymphadenopathy is often present
Local lymph glands may be enlarged and tender (submandibular or cervical lymphadenopathy)
Is usually self-limited and lesions heal within 1 to 2 weeks

Figure 9-4 Aphthous ulcer.
Here silver nitrate is applied directly to a lesion.
Some patients may require IV hydration and systemic pain control in addition to antiviral therapy
Encephalitis and aseptic meningitis are very rare complications
Diagnosis
Clinical, usually based on clinical appearance and history
A Tzanck smear is the fastest and easiest test to help make the diagnosis (see Appendix: Diagnostic and Therapeutic Techniques)
A fresh viral culture from intact vesicles or direct fluorescent antibody testing
Polymerase chain reaction for HSV DNA detection
Differential Diagnosis
Aphthous stomatitis
Hand-foot-and-mouth disease
Herpangina
Erythema multiforme
Management
Pain Control
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


