Abstract
Proper nutrition is fundamental to human life. From fetal development to adulthood, proper nutrition is essential for survival, physical growth, mental development, productivity, and overall health. The skin, hair, nails, and mucous membranes may all provide clues to the presence of a nutritional deficiency, and often a patient will have multiple deficiencies. In addition to inadequate oral intake, there are secondary causes of nutritional deficiencies, e.g. intestinal malabsorption. Two classic protein–energy malnutrition syndromes have been described, kwashiorkor and marasmus, and each has characteristic features. Deficiencies of vitamins and trace elements can lead to a wide range of mucocutaneous findings, from follicular keratoses to photodistributed erythema to periorificial erosions and atrophic glossitis.
Keywords
protein–energy malnutrition, vitamin deficiencies, obesity, kwashiorkor, marasmus, vitamins, trace elements, zinc deficiency, pellagra, acrodermatitis enteropathica, scurvy, phrynoderma, atrophic glossitis, vitamin D deficiency
- ▪
Nutritional deficiencies may affect any organ system, including the skin, which may provide clues to the diagnosis
- ▪
The two classic protein–energy malnutrition syndromes are kwashiorkor and marasmus
- ▪
In addition to inadequate oral intake, there are secondary causes of nutritional deficiencies, e.g. intestinal malabsorption due to medical conditions or surgical procedures
- ▪
Vitamin and trace element deficiencies can lead to a wide range of mucocutaneous findings, from follicular keratoses to periorificial erosions and glossitis
- ▪
Insufficient and deficient levels of vitamin D have been noted worldwide, in both low-income and high-income countries
- ▪
Obesity can be associated with high-calorie malnutrition and a number of skin changes, from acanthosis nigricans to lipodermatosclerosis
Introduction
Proper nutrition is fundamental to human life. From fetal development to adulthood, proper nutrition is essential for survival, physical growth, mental development, productivity, and overall health . Deficiency of one isolated nutrient is rare, as individuals are usually deficient in multiple nutrients at the same time. In general, nutrients are categorized as macronutrients (carbohydrates, proteins and fats) or micronutrients (vitamins and minerals). Most people who suffer from nutritional deficiencies live in low-income countries. However, there are certain conditions that predispose individuals from high-income countries to develop nutritional deficiencies, such as alcoholism, intestinal malabsorption, anorexia nervosa or bulimia, and restrictive diets.
Nutrients require a process of ingestion, digestion, absorption and circulation plus subsequent metabolism in order to be beneficial. When any one of these steps is disrupted, clinical manifestations may appear.
Epidemiology and Pathogenesis
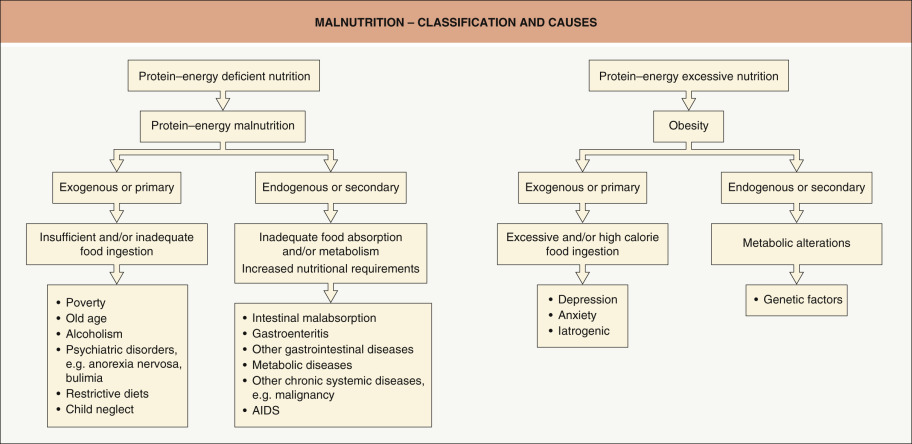
In low-income countries, malnutrition stems primarily from inadequate ingestion of all macronutrients as well as many micronutrients ( Fig. 51.1 ). The World Health Organization (WHO) has estimated that worldwide, ~50% of deaths in children <5 years of age are due directly or indirectly to the multisystem ramifications of malnutrition. In industrialized regions of the world, malnutrition is directly linked to the per capita gross national product; if a country has a per capita income that is less than US$300 per year, endemic malnutrition is likely, especially in infants and young children.
At the same time, a global epidemic of obesity has emerged within industrialized countries, with increasing rates of death due to cardiovascular disease and diabetes mellitus . Excessive consumption of foods high in calories but low in nutrients can lead to obese patients who lack essential vitamins and minerals. This is supported by a study in which 57% of morbidly obese patients undergoing preoperative assessment for bariatric surgery were found to have a deficiency in at least one micronutrient .
Restrictive diets, including those based upon real or perceived need (e.g. food allergies), psychiatric illness (e.g. anorexia nervosa) or mental impairment (e.g. illicit drug abuse), also disrupt the intake of appropriate nutrients and can result in malnutrition.
In addition to a diet inadequate in the quantity and/or quality of macro- and micronutrients (i.e. primary causes), there are medical conditions that can lead to a functional malnutrition, i.e. secondary causes. The latter include an increase in metabolic requirements (e.g. severe infections) and/or a decrease in the transport and utilization of nutrients (e.g. intestinal malabsorption, bariatric surgery). Malnutrition is also seen in individuals with late-stage internal malignancies and advanced AIDS ( Table 51.1 ).
| CHARACTERISTICS OF PROTEIN–ENERGY MALNUTRITION AND ESSENTIAL FATTY ACID DEFICIENCY | |||
|---|---|---|---|
| Protein–energy malnutrition | Essential fatty acid deficiency | ||
| Marasmus | Kwashiorkor | ||
| Causes |
|
|
|
| Cutaneous features |
|
|
|
| Systemic features |
|
|
|
| Lab findings and diagnostic criteria |
|
|
|
| Treatment |
|
|
|
| Prognosis |
|
|
|
* HIV infection is more often associated with marasmus than with kwashiorkor.
Clinical Features
Weight-for-height scores and height-for-age scores are utilized to evaluate malnutrition; scores are compared to the standard deviations (SD) from the median value for the reference population. An individual is considered to have moderate malnutrition if the scores are between the 2 nd to 3 rd (lower) SD and severe malnutrition if below the 3 rd SD, with or without symmetrical edema . Cutaneous manifestations in part reflect the fact that epidermal maturation (from basal cell layer to stratum corneum) occurs over a period of 10–14 days. Deficiencies, especially of macronutrients, can interfere with this process, resulting in skin that is dry and thin in appearance with associated epidermal atrophy. Prolonged deficiency can reduce both protein production, including that of dermal collagen and muscle, and the amount of subcutaneous fat. As a result, patients may develop dermal atrophy, muscle wasting, and/or lax skin.
Additional clinical findings of marasmus and kwashiorkor, such as dyschromia (hypo- and hyperpigmentation), desquamation and erosions, are reviewed in Table 51.1 . Patients may also have cutaneous manifestations from a deficiency in one or more micronutrients, and these are outlined in Table 51.2 . Mucocutaneous clues to the possibility of a nutritional deficiency are summarized in Fig. 51.2 .
| VITAMIN DEFICIENCIES IN ADULTS AND CHILDREN | |||||
|---|---|---|---|---|---|
| Vitamin | Clinical manifestations | Reference values | Replacement therapy | ||
| Mucocutaneous | Systemic | Other | |||
| Fat-soluble vitamins – can easily accumulate and lead to toxicity if replaced in high doses for prolonged periods | |||||
| A (retinol) |
|
|
|
|
|
| D D 2 : ergocalciferol D 3 : cholecalciferol |
|
|
|
|
|
| E (tocopherol) |
|
|
|
| |
| K K 1 : phytonadione (source = diet) K 2 : menaquinone (source = gut bacteria) | Purpura, ecchymoses |
|
|
| |
| Water-soluble vitamins – less likely to accumulate & lead to toxicity, but in high doses can lead to side effects, e.g. nephrolithiasis (vitamin C), hepatitis (niacin) | |||||
| C (ascorbic acid) |
|
|
|
|
|
| B 1 (thiamin; thiamine) |
|
|
|
|
|
| B 2 (riboflavin, lactoflavin) |
|
|
|
|
|
| B 3 (niacin, nicotinic acid) |
|
|
|
|
|
| B 5 (pantothenic acid) |
|
|
|
| Vitamin B 5 is ubiquitous in the food supply and deficiency rare |
| B 6 (pyridoxine, pyridoxamine, pyridoxal) |
|
|
|
| |
| B 7 (biotin) |
|
|
|
|
|
| B 9 (folic acid) |
|
|
|
|
|
| B 12 (cyanocobalamin [CNCbl]) |
|
|
|
|
|
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


