Periorbital rejuvenation is a common reason for patients to seek cosmetic treatment. There are several nonsurgical light and energy–based devices available to treat various aspects of periorbital rejuvenation without risks of an invasive, surgical procedure. Although ablative laser resurfacing appears to offer the most impressive clinical improvements, nonablative devices result in noticeable cosmetic improvement with more favorable side-effect profiles and shorter recovery times. The specific modality selected for periorbital rejuvenation should be tailored to patients’ individual characteristics, preferences, and aesthetic goals. With continued advancements, additional nonsurgical light and energy–based devices will become available in the future for periorbital rejuvenation.
Key points
- •
Various light and energy–based devices are utilized successfully for nonsurgical periorbital rejuvenation.
- •
Ablative laser resurfacing achieves significant clinical improvement, although associated with a longer recovery period and increased risk of adverse effects.
- •
Nonablative modalities are alternatives for periorbital rejuvenation associated with shorter recovery times and a more favorable side-effect profile.
- •
The specific modality selected should be tailored to the individual patient, patient preferences, and patient goals of treatment.
Introduction
The eyes play an important role in human interaction and overall facial appearance. The periorbital region is one of the first areas to show signs of aging. These changes include rhytides, dyschromia, skin laxity, textural changes, and telangiectasia. As such, patients commonly seek cosmetic treatment of periorbital rejuvenation to achieve a more youthful appearance. Traditional surgical interventions, including blepharoplasty, remain the gold standard for periorbital rejuvenation. Downtime and risk, however, associated with surgery, make nonsurgical light and energy–based methods increasingly popular, even though the objectives are somewhat different. The goal with these treatments is to achieve a natural aesthetic appearance while minimizing patient recovery times and associated adverse events. This article discusses the various nonsurgical light and energy–based devices available for periorbital rejuvenation.
Periorbital rhytides
The development of periorbital rhytides is multifactorial, with photoaging and movement of the orbicularis oculi both playing a role. Neuromodulators and soft tissue augmentation are used in treatment, but the focus of this article is on lasers and energy-based devices. Periorbital rhytides are common reasons patients seek cosmetic treatment, and both ablative resurfacing lasers and nonablative lasers successfully are used to treat periocular rhytides.
Ablative laser resurfacing was one of the earliest nonsurgical modalities utilized for periorbital rejuvenation. Ablative laser resurfacing devices include the carbon dioxide (CO 2 ) laser and the 2940-nm Er:YAG laser. Fully ablative laser resurfacing involves vaporization of the entire epidermis as well as part of the dermis, leading to collagen shrinkage, increased collagen production, and tissue remodeling, resulting in clinical improvement. , These devices are used in conjunction with blepharoplasty but also are shown to be effective for the treatment of periorbital wrinkles when used as monotherapy.
Fully ablative CO 2 laser demonstrates consistent efficacy for the treatment of periorbital rhytides with significant clinical improvement. , In 2004, Alster and Bellew performed a retrospective study of 67 patients, evaluating the safety and efficacy of high-energy pulsed CO 2 laser as monotherapy for the treatment of dermatochalasis and periorbital wrinkles. All patients demonstrated significant improvement in dermatochalasis and periorbital rhytides; however, those with more severe dermatochalasis and rhytides at baseline demonstrated greater improvement than those with mild to moderate findings at baseline. Fully ablative treatment with CO 2 resurfacing lasers is accompanied by long recovery periods, most commonly prolonged erythema that can persist for 3 months to 4 months. , Other adverse effects include postprocedural hyperpigmentation, hypopigmentation, milia, infection, scarring, and ectropion. Lower lid ectropion is considered a rare but severe complication, with the greatest risk in those who have undergone previous blepharoplasty. , , The medial one-third of the lower lid is the highest-risk area for developing ectropion. In the authors’ experience, patients with flat cheeks and prominent eyes also are at higher risk for lower lid ectropion. Prior to treatment with CO 2 laser resurfacing, patients are counseled appropriately on these potential adverse effects, and realistic expectations of outcomes should be established ( Fig. 1 ). The authors believe that full ablative laser skin resurfacing remains the gold standard in the treatment of moderate to severe eyelid and periorbital photoaging changes.

An effort to achieve a favorable result with fewer adverse events led to the application of fractional laser resurfacing. Fractional ablative resurfacing delivers ablative injury to microscopic columns of tissue in regularly spaced arrays, leaving parts of the intervening skin intact. This allows for more rapid epithelialization and decreased postprocedural recovery time. Rates of adverse effects also are reduced, including dyschromia due to decreased melanin absorption. , Kotlus evaluated the efficacy and safety of dual-depth fractional CO 2 laser ablation (Lumenis, Santa Clara, California) for the treatment of periorbital rhytides and observed a 53% improvement in periocular rhytides and 42% improvement in skin laxity. The recovery profile was favorable without prolonged erythema or serious complications, and only 2 patients experienced postinflammatory hyperpigmentation that resolved in 3 months with topical hydroquinone 4% cream. Similarly, Bonan and colleagues observed significant improvement, rated as moderate, marked, or excellent response, in skin tightening and periorbital rhytides in 69% of patients 1 year after treatment with the fractional CO 2 laser. Notably, 82% of patients demonstrated measurable eyebrow elevation 1 year after treatment. In practice, the degree of brow elevation after treatments often is clinically irrelevant. Clinical results with ablative fractional lasers are comparable to the standard ablative CO 2 resurfacing lasers but with more rapid recovery times and a better risk profile. Multiple treatments may be required, however, with ablative fractional lasers for optimal outcomes. Although the recovery time after ablative fractional resurfacing is shorter than after full ablative resurfacing, it still is not insignificant for most patients.
The 2940-nm Er:YAG laser is another ablative laser that clinically improves periorbital wrinkles. When compared with the CO 2 laser, the traditional short-pulsed Er:YAG laser has a more superficial depth of ablation with little coagulation and is considered less effective for deeper or severe rhytides, requiring more passes to achieve the same degree of tissue ablation. , Given the superficial energy absorption, the Er:YAG laser is associated with faster recovery times and decreased risk of scarring or adverse effects compared with the CO 2 laser. In a comparative, randomized, split-face trial of the fractional CO 2 laser and the fractional Er:YAG long-pulsed laser for the treatment of periorbital wrinkles, they demonstrated comparable efficacy. A recent review of the literature argued that the Er:YAG laser should be considered the treatment of choice for fine lines and superficial rhytides, whereas the CO 2 laser was better for deeper, severe rhytides and moderate to severe dermatochalasis. Newer long-pulsed Er:YAG systems have been developed that allow for increased depth of ablation and better coagulation, yielding results comparable to the CO 2 laser. These devices have 2 Er:YAG laser heads that combine short ablative and long sublative coagulative pulses, allowing for greater modification of optimal ablation depth and coagulation. Studies evaluating the efficacy of these newer Er:YAG systems demonstrate significant improvement in rhytides, including moderate to severe rhytides.
In order to maximize the results of laser therapy, pretreatment of periorbital rhytids with botulinum toxin 1 week to 6 weeks prior to laser therapy is shown to enhance and prolong the effects of ablative laser resurfacing. , Therefore, pretreatment with neuromodulators should be offered and discussed with patients prior to performing any ablative laser resurfacing procedure to maximize potential clinical improvements. Although the authors encourage pretreatment with neuromodulators, this is not an absolute requirement for treatment.
Nonablative fractional lasers (NAFLs), including the 1540-nm and 1550-nm erbium-doped mid-infrared lasers, the 1540-nm Er:GLASS laser, the 1440-nm NAFL, and the 1410-nm NAFL, demonstrate significant clinical improvement in periorbital wrinkles with minimal adverse effects. , In the authors’ experience, the 1550-nm NAFL yields superior results compared with other nonablative therapies. In the original split-face study, 30 patients with periorbital wrinkles were treated using the 1550-nm NAFL with the handheld scanning device. At 1 month after the last treatment, 54% demonstrated moderate to significant improvement in periocular wrinkles and 53% had moderate improvement in skin texture. At 3 months’ follow-up, 34% and 47%, respectively, had at least moderate improvement in wrinkles and skin texture. Long-term studies are needed to determine the sustainability of these effects in comparison to those seen with ablative procedures. In a study evaluating the long-term benefits of the 1540-nm Er:GLASS laser for the treatment of perioral and periocular rhytides, up to 30% of patients demonstrated sustained improvement at 35 months’ follow-up. All patients underwent 5 treatments at 6-week intervals, with 5 patients receiving 2 maintenance treatments at 14 weeks and 20 weeks. Therefore, although resurfacing with NAFLs may provide long-term clinical results, multiple treatments or maintenance treatments may be required to sustain these results, in contrast to ablative fractional resurfacing that provides significant improvement following a single treatment. Although these nonablative devices often are not used solely for periorbital rejuvenation, they are popular full-face treatments and are done more commonly than ablative procedures.
When discussing nonablative lasers for improving rhytides, NAFLs have been the most effective; however, other nonablative devices have been studied. Treatment with these devices produces dermal thermal injury while preserving the integrity of the epidermis, leading to less risk for adverse effects and shorter postprocedural downtimes. Although intense pulsed light (IPL) commonly is used to treat dyschromia and vascular lesions, it has demonstrated minimal effectiveness in improving periorbital rhytides. Based on the current literature and the authors’ experience, IPL offers no significant improvement in periorbital rhytides but does improve the appearance of some vascular lesions and dyschromia. Although studies suggest IPL is relatively safe in darker-skinned patients, caution should be taken, and appropriate preprocedural counseling performed.
IPL has demonstrated efficacy in the treatment of dry eye disease and increasingly is used in the periocular area for this indication. Dry eye disease is a multifactorial condition due to abnormalities of tear production, gland function, and the ocular surface. There appears to be an association with meibomian gland dysfunction and inflammatory skin conditions that occur in close proximity to the periocular area, including rosacea. Initially, IPL was noted to be helpful for symptoms of dry eye while patients were receiving treatment of facial rosacea. Studies demonstrate consistent improvements in signs and symptoms of dry eye disease after IPL treatment with and without adjunctive meibomian gland expression. Typically, treatments involve several IPL sessions, each consisting of IPL pulses from tragus to tragus just below the lower eyelids, although recent studies have demonstrated safety and efficacy with a unique handpiece treating the upper eyelids as well. Postulated explanations for the effectiveness of IPL in treating dry eye disease secondary to meibomian gland dysfunction include heating and softening of the abnormal meibum, reduction of epithelial turnover, decreased risk of gland obstruction, modulation of proinflammatory and anti-inflammatory molecules, suppression of matrix metalloproteinases, thrombosis of local vessels delivering secreted inflammatory markers involved in the inflammatory response, decreased Demodex species and local bacterial load contributing to chronic inflammation, and photomodulation. , Ultimately, these effects result in a diminished local inflammatory response and promote normal meibomian gland function, alleviating the signs and symptoms of dry eye disease.
The 595-nm pulsed dye laser (PDL) traditionally has been utilized for vascular lesions but also has been shown to improve periorbital rhytides, although results are inconsistent and often not clinically relevant. Zelickson and colleagues evaluated the safety and efficacy of the 585-nm PDL in 20 patients with mild to moderate or moderate to severe periorbital rhytides. After a single treatment, 9/10 patients with mild to moderate rhytides demonstrated greater than 50% improvement and 3/10 of these patients demonstrated greater than 75% improvement, which was maintained at 6 months’ follow-up. Those with moderate to severe rhytides demonstrated less clinical improvement. Significant postprocedural purpura and edema lasting for 1 week to 2 weeks were noted in a majority of patients. Although these devices commonly are used to treat vascular lesions, these studies show improvement in skin texture with a series of treatments. From a practical clinical perspective, the PDL treatment does not produce meaningful improvement in wrinkling. When PDL is used to treat dark circles caused by vascular changes within the eyelid skin, improvement in overall skin quality can be noted.
Based on current data, the Nd:YAG laser at various pulse durations is effective in the treatment of periorbital wrinkles. In a split-face study, Chang and colleagues evaluated the efficacy of the 1064-nm long-pulsed Nd:YAG laser for periorbital wrinkles in 20 Korean patients and found that all patients demonstrated modest improvement after 3 treatments. Mean wrinkle score on the laser-treated side decreased by approximately 35%, whereas no change was observed on the control side. These clinical improvements were not maintained at 6 months’ follow-up. No serious adverse effects were observed during the study. This suggests that the long-pulsed Nd:YAG may be a safe and effective option for treating periorbital wrinkles, even in patients of darker skin types. More than 3 treatment sessions likely are needed to maintain long-term clinical improvement.
Although ablative resurfacing produces the most consistent and significant improvement in periorbital rhytides, nonablative lasers are potential alternatives that offer less risk of erythema, pigmentary changes, or scarring and shorter recovery periods. Given that nonablative devices produce less injury and damage to the skin, these modalities require several treatment sessions to achieve desirable cosmetic outcomes, and the degree of clinical improvement often is less than with ablative resurfacing, even with multiple treatments.
Periorbital skin tightening
Periorbital skin laxity and dermatochalasis are additional components of photoaging that often are troublesome to patients, prompting them to seek aesthetic treatment. Similar to periorbital rhytides, ablative and nonablative laser devices have demonstrated efficacy in improving periorbital skin laxity and dermatochalasis. Studies also demonstrate the efficacy of other light and energybased devices including radiofrequency (RF) devices and microfocused ultrasound (MFUS) devices in promoting periorbital skin tightening and improving dermatochalasis, achieving tissue tightening by dermal heating.
Ablative laser resurfacing and fractional ablative laser resurfacing are efficacious in treating rhytides and improving periorbital skin laxity, with the latter modality having a more favorable risk profile. , , NAFL devices also are effective in the treatment of periorbital skin laxity. Sukal and colleagues evaluated the effects of the 1550-nm NAFL device on eyelid tightening and eye aperture opening in 31 patients who underwent 3 to 7 treatments at 3-week to 4-week intervals. One month after the last treatment, all patients exhibited some eyelid tightening, with 55% having greater than 50% tightening. An increase in eyelid aperture was observed in 56% of patients. Patients experienced mild to no edema postoperatively and there were no reports of dyschromia, persistent erythema, or scarring. Although the results of this study suggest NAFL devices are safe and effective options to improve periorbital skin laxity, in clinical practice, NAFL devices are not used for skin tightening.
RF devices are another modality that demonstrate efficacy for periorbital rejuvenation. These devices generate heat deep in the dermis and hypodermis, with limited effects on the epidermis, via a rapidly alternating electric current. The current is delivered by 1 or more skin electrodes. The thermal injury stimulates immediate collagen contraction and promotes progressive tissue remodeling and collagen and elastin production, resulting in skin tightening. The number of treatment electrodes characterizes the RF device as monopolar, bipolar, or multipolar. Monopolar RF devices have a single treatment handpiece or paddle, whereas bipolar and multipolar devices have multiple electrodes against the skin with current flowing between them. In addition, RF devices with microneedling are available that invasively deliver current through a needle or array of needles into the skin.
The first monopolar RF device (Thermage, Solta, Hayward, California) was approved by the United States Food and Drug Administration for the treatment of periorbital rhytides in 2002. It currently is the only device cleared for use on the eyelid itself. Fitzpatrick and colleagues performed a multicenter study of 86 patients who received a single treatment and observed Fitzpatrick wrinkle scale score improvements of at least 1 point in 83% of subjects 6 months after treatment; 62% of patients also demonstrated an eyebrow lift of at least 0.5 mm. Associated adverse effects were minimal, including transient erythema and edema. In a prospective, multicenter trial, Biesman and colleagues treated the eyelids of 72 patients with a single session using a monopolar RF device (Thermage). A shallow treatment tip was developed and utilized to deliver heat more superficially compared with existing treatment tips to decreasing the risk of injury to vital structures within the eye or eyelid. Six months after treatment, upper eyelid tightening and lower eyelid tightening were noted in 88% and 71% to 74% of patients, respectively. No serious adverse events were reported. Similar results with improvement in periorbital skin tightness following treatment with monopolar RF devices is reported. This particular monopolar RF device remains the only skin tightening device with a specific indication for use on the eyelids.
Transcutaneous, temperature-controlled, monopolar RF devices have been developed for treatment in the periorbital area to maximize safety by ensuring treatment temperatures remain within an appropriate range ( Fig. 2 ).

Studies evaluating bipolar RF devices similarly demonstrate efficacy in promoting periorbital skin tightening. Lolis and Goldberg evaluated the safety and efficacy of a bipolar fractional RF device (eMatrix, Syneron Medical, Irvine, California) in 20 patients with periorbital rhytides and laxity. Each patient underwent 3 treatments at 4-week intervals. At 6 months after the last treatment, 50% of patients demonstrated moderate to marked improvement. Treatments were well tolerated, with only 3 patients experiencing postinflammatory hyperpigmentation that resolved with hydroquinone cream. Later studies similarly demonstrate improvement in facial wrinkles and laxity with various treatment protocols utilizing fractional bipolar RF devices or fractional multipolar RF devices with a favorable safety profile. In all of these studies, patients of varying skin types demonstrated improvement with only occasional, mild side effects observed, including transient discomfort, erythema, and edema. Most patients were able to return to their daily routines almost immediately after treatment.
Microneedling RF devices were developed to enhance dermal heating by delivering energy directly through needles that penetrate the skin to a predetermined depth. Greater collagen remodeling is stimulated by both the dermal heating and the physical stimulation. In 2009, Hantash and colleagues , performed the initial studies evaluating the effects of a novel bipolar microneedling RF device, revealing the associated with neocollagenesis and neoelastogenesis. Kim and colleagues evaluated the efficacy of a fractional RF microneedling device for the treatment of periorbital rhytides in 11 Asian women undergoing 3 treatments at 3-week intervals. Three months after the last treatment, significant improvement in periorbital rhytides was observed. All patients tolerated the treatment, and no adverse events were reported.
RF devices appear to be an effective nonsurgical modality for the treatment of periorbital laxity, safe in patients of all skin types with no downtime with proper energy and a favorable side-effect profile. Response to treatment may be more gradual with effects seen in 4 weeks to 6 weeks or even 6 months after treatment. These devices are becoming increasingly popular, with a wide discrepancy between devices. These devices can be effective for skin tightening; however, it is treatment and technique dependent. There is a need for more standardized treatments and a way to compare the different available devices. Fractionated RF and microneedling with RF are invasive, and these devices have a depth of penetration, which is why there is a potential risk of postinflammatory hyperpigmentation. These devices should be used with great care on the eyelid skin. Treatment of eyelid skin with RF microneedling currently is off-label from a regulatory perspective.
MFUS is another noninvasive modality utilized for periorbital rejuvenation. MFUS acts by depositing points of microthermocoagulation at specific depths into the dermis, creating discrete points of skin contraction, promoting skin tightening and improvement in skin laxity. The MFUS device (Ultherapy, Ulthera, Mesa, Arizona) is the first and only energy-based device Food and Drug Administration approved for aesthetic lift of the brow, neck, and submental area. , The device is applied to the periorbital region (outside of the eyelids) and forehead to promote eyebrow lift and should not be used on the eyelids or within the orbital rim, because the eye cannot be shielded safely during treatment. Pak and colleagues evaluated the safety and efficacy of an MFUS device (Ulthera System, Ulthera) for periorbital rejuvenation and observed skin tightening and improvement in infraorbital laxity in all treated patients. Patients tolerated the procedure well with minimal pain during treatment and no adverse effects were reported. Although patients are reported to have minimal pain, in the authors’ experience, there is pain associated with the procedure that should be managed. Because the user is able to visualize the depth being targeted during treatment with ultrasound, only a certain zone is targeted, leaving remaining depths unaffected similar to a fractionated device, resulting in faster postprocedural recovery times. Newer devices on the market (Sofwave, Israel) deliver the ultrasound energy to a fixed depth (1.5 mm) within the skin (Sofwave), removing the need to precisely visualize the depth during treatment. Given that MFUS spares the epidermis, it is a favorable modality to use in patients prone to postinflammatory hyperpigmentation. MFUS appears to be a safe and effective alternative for nonsurgical eyebrow lift and periorbital rejuvenation.
RF devices and MFUS are effective treatment modalities for improving periorbital skin laxity with minimal down time, depending on the device, and decreased risk of associated adverse effects. The authors’ clinical experience is that there is variability in the results depending on the patient. Those patients with severe laxity and atrophic skin are not good candidates for these treatments and do not have optimal outcomes. These devices are effective, but, as discussed previously, they are not a replacement for surgery.
Periorbital hyperpigmentation
Periorbital hyperpigmentation is another aspect of photoaging that occurs in the periorbital region. Periorbital hyperpigmentation may be secondary to dyschromia, translucency of the thin periorbital skin, or underlying cutaneous vasculature, which can manifest as a brown or purple-red discoloration infraorbitally. Patients frequently seek cosmetic therapy for periorbital hyperpigmentation, or dark circles, under the eyes, because this has been associated with a tired or older appearance. Currently, the literature evaluating the efficacy of medical treatment of periorbital hyperpigmentation is mixed, without real data to confirm consistent benefit. Periorbital hyperpigmentation is treated successfully with various laser and light devices targeting vascularity and pigment.
Studies have shown significant improvement in infraorbital hyperpigmentation with CO 2 laser resurfacing. A risk of postprocedural dyschromia, especially in those with darker skin types, may limit use of ablative laser resurfacing in this patient population. The daily use of a bleaching cream for several weeks prior to and after the procedure can decrease the risk of subsequent pigmentary alteration.
IPL demonstrates efficacy in the treatment of periorbital pigmentation when used for periorbital rejuvenation. Negishi and colleagues treated 97 Asian patients with 3 to 6 sessions of IPL and observed good or excellent improvement in periorbital pigmentation in 90% of patients. In addition, these patients had improvement in periorbital telangiectasias and skin texture. Subsequent studies confirm improvement in pigmentation with IPL. , IPL effectively treats periorbital hyperpigmentation, even in darker-skinned individuals, with the additional benefit of treating associated vascular lesions and improving skin texture.
Several studies have established the efficacy of the 1064-nm Q-switched and long-pulsed Nd:YAG laser in treating periorbital hyperpigmentation, especially when associated with underlying vasculature. Several studies also support the use of the 694-nm QS ruby laser for periorbital hyperpigmentation. Following treatment, 80% to 93% of patients demonstrated good to excellent results, with up to 89% of patients experiencing greater than 50% improvement. , Most patients experienced only mild pain and erythema. ,
Newer technologies, such as the picosecond laser, are shown to be effective for periorbital dyschromia. In a study evaluating the picosecond 755-nm alexandrite laser, a significant improvement of periorbital hyperpigmentation was noted without any reports of postinflammatory hyperpigmentation at 3 months’ follow-up.
These nonablative lasers appear to have a relatively favorable side-effect profile with decreased risk of dyschromia and minimal postprocedural downtime. Selection of a specific modality for the treatment of periorbital hyperpigmentation is based on individual patient characteristics, patient preferences, and goals of cosmetic treatment to ensure optimal results, similar to when approaching treatment of periorbital rhytides or laxity.
Periorbital telangiectasias and vascular lesions
Telangiectasias and prominent vasculature, commonly seen in other areas of the face, are particularly bothersome in the periorbital area. The efficacy of laser treatment depends on several factors, including target chromophore, vessel size, vessel depth, and vascular flow rate. Many laser and light systems, such as the 532-nm potassium titanyl phosphate (KTP) laser, PDL, and IPL, represent treatment options, with PDL and long-pulsed 532-nm laser treatment of choice for superficial telangiectasias.
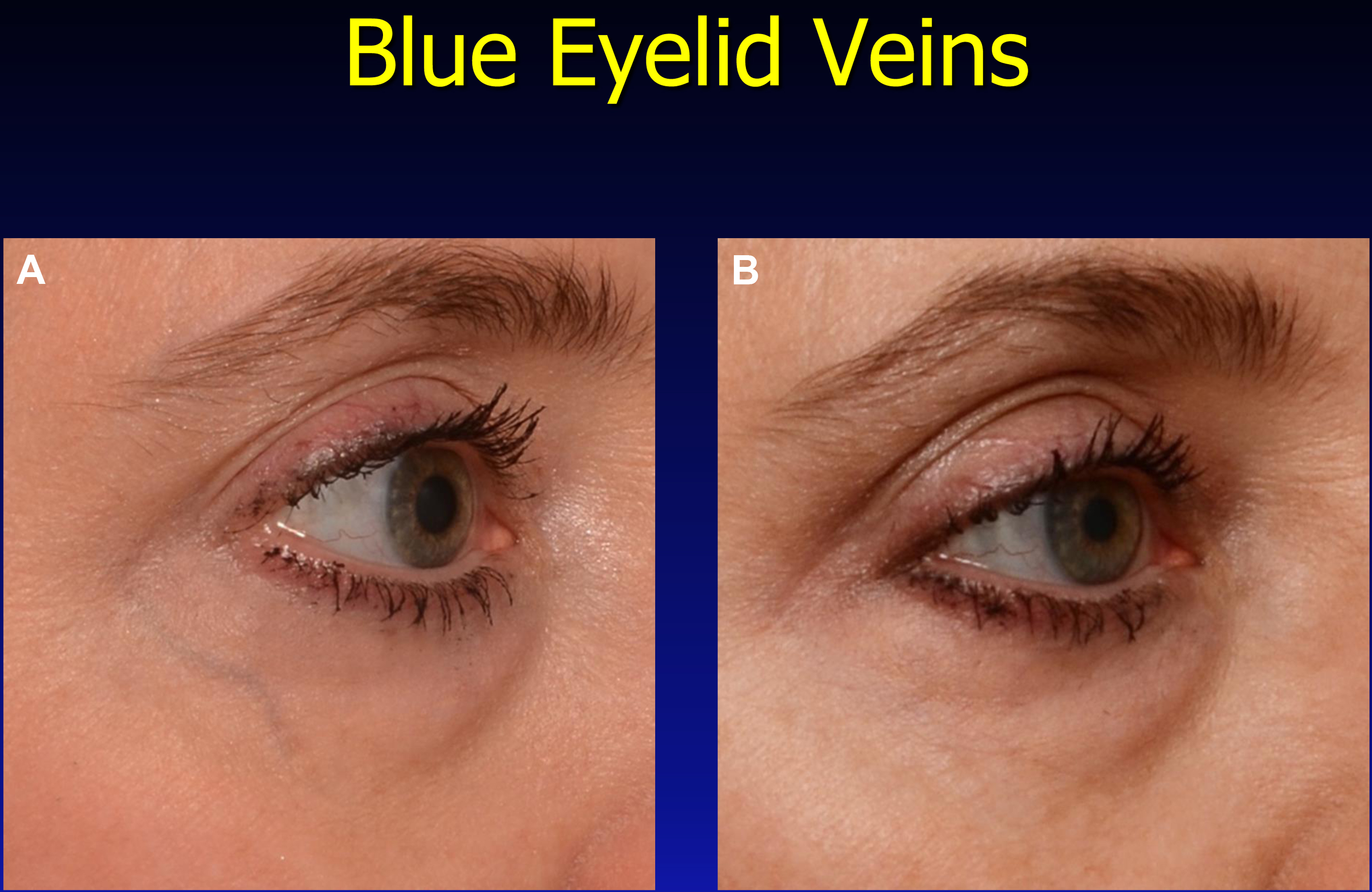
Treatment of facial reticular veins in the periocular area frequently is a requested cosmetic procedure. Patients may have a genetic predisposition or develop reticular veins after cosmetic surgery. Invasive therapies, including cautery, sclerotherapy, and phlebectomy, rarely are used due to side effects, including ulceration and blindness. , Due to these serious side effects, use of the 1064-nm Nd:YAG lasers has increased, which penetrate deeper into the dermal blood vessels, thereby decreasing the risk of epidermal damage. The treatment endpoint is disappearance of blue, which is achieved by increasing the fluence slowly, if needed. Warning endpoints include graying or whitening of the skin, which can result in blistering and scarring. Smaller veins on the lower eyelids may require higher fluences, whereas veins on the upper eyelids may be treated with lower fluences. Small arterioles near the eyelashes, despite their high-pressure flow, also may respond to laser therapy ( Fig. 3 ).
Related posts:
 Treatment Options for Lower Eyelid Festoons
Treatment Options for Lower Eyelid Festoons
 Blepharoptosis Repair: External Versus Posterior Approach Surgery: Why I Select One over the Other
Blepharoptosis Repair: External Versus Posterior Approach Surgery: Why I Select One over the Other
 The Treatment of Post-blepharoplasty Lower Eyelid Retraction
The Treatment of Post-blepharoplasty Lower Eyelid Retraction
 My Evolution with Endoscopic Brow-Lift Surgery
My Evolution with Endoscopic Brow-Lift Surgery
 Transcutaneous Blepharoplasty with Volume Preservation
Transcutaneous Blepharoplasty with Volume Preservation
 Periorbital Fat Grafting
Periorbital Fat Grafting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


