Neuromuscular Scoliosis
Brian Snyder
Operative Indications
Expected benefit outweighs negative consequences of natural history and surgical risks
Curve >50° with progression
Difficulty with seating, failed bracing
Age >10 versus <10 years → fusion versus growth sparing instrumentation
Adequate hip range of motion for sitting
Stable medical status (nutrition, pulmonary, neurologic)
Preoperative Workup
Pulmonary—restrictive lung disease
FVC < 25%—higher risk of complications
Upper airway obstruction—tonsillectomy/adenoidectomy
Need for BiPAP, CPAP, cough assist
Seizure medications (valproic acid increases bleeding)
Gastrointestinal disorders—reflux, constipation
Nutrition—poor nitrogen balance = poor wound healing
ANC > 1200, albumin > 3
G-tube
Cardiomyopathy—left ventricular (LV) ejection fraction < 50% contraindication
Osteopenia—poor purchase of bone anchors
Vitamin D supplement, bisphosphonates if previous fragility fractures
High-Risk Spine Protocol
Screen for methicillin-resistant Staphylococcus aureus (MRSA; swab nares, axilla, groin/anus)
Chlorhexidine shower night before
Alcohol + ChloraPrep skin prep
Antibiotics within 1 hour of incision, 24 hours postop
Cephalexin + aminoglycoside to lessen risk surgical site infection; plus vancomycin if there is methicillin resistant staph aureus (MRSA)
Tranexamic acid (TXA) to decrease blood loss
Titanium instrumentation
Prior to wound closure:
Dilute povidone lavage (3 minutes); debride necrotic tissue
Sprinkle 1 g of vancomycin powder into wound
Soak allograft in gentamycin irrigation solution × 2 hours
Drains deep to muscle closure—prevent hematoma
Equipment
Jackson table
Halo-femoral traction setup
Standard fluoroscopy/navigation/robotic equipment
Ultrasonic bone scalpel
Aquamantys tissue bipolar sealer
Cell Saver
Neuromonitoring
Spinal implant system
Titanium
Hooks/bands/screws
Pelvic fixation screws
Positioning
Standard spine table
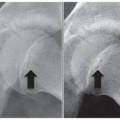
Headrest with pressure off eyes (Figure 6.1)
Halo ring for significant kyphosis, expected prolonged operative time, traction cases
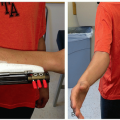
Muscular releases may be needed prior to spine surgery in order to position patient. This may include pectoralis release, biceps and wrist flexor release, hip releases, and hamstring releases (Figure 6.2)
Halo-femoral traction
Halo ring with single or bilateral femoral traction pins
Single pin in ipsilateral femur of high pelvis side
Levels pelvis and improves flexibility of lumbar curve
Neuromonitoring
Somatosensory spinal evoked potential (SSEP) may be unreliable in monitoring neuromuscular patient
Improved reliability when combined w/ SSEP
86% cerebral palsy (CP) patients (moderate involvement) had response to at least one modality
Indicated for patients w/ weight bearing function, usable motor function, preserved bowel/bladder function
Does NOT elicit seizure activity
Spinal muscular atrophy (SMA), Duchenne muscular dystrophy—motor evoked potentials may be absent, but SSEPs presentRelated posts:
 Surgical Decision-Making in Pediatric Hand and Arm
Surgical Decision-Making in Pediatric Hand and Arm
 Decision-Making in Pediatric and Adolescent Hip Disorders
Decision-Making in Pediatric and Adolescent Hip Disorders
 Clubfoot Casting and Heel Cord Lengthening
Clubfoot Casting and Heel Cord Lengthening
 Radioulnar Synostosis Derotation Osteotomy
Radioulnar Synostosis Derotation Osteotomy
 Neuromuscular Hip Surgery: Prevention to Reconstruction
Neuromuscular Hip Surgery: Prevention to Reconstruction
 Minimally Invasive Techniques for Foot Deformity Correction
Minimally Invasive Techniques for Foot Deformity Correction

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


