Since the first edition of this text, the word “neuromodulator” has become a more contemporary word than “neurotoxin” as the drug is not cytotoxic. Neuromodulators are medications that change the way conduction occurs between nerves and muscles. Many contemporary experts only use the term “neuromodulator” to refer to botulinum toxin, while others refuse to abandon the word “neurotoxin.” This chapter will use both of these terms interchangeably.
If there is a single treatment that has revolutionized cosmetic facial surgery over the past century, it would have to be botulinum toxin type A. Surgeons, patients, and the media are in constant search of a procedure that produces significant effects with insignificant recovery, but it rarely happens. Most products, surgeries, or devices that promise results without recovery time are problematic, and expectations exceed outcomes. This has not been the case with botulinum toxin A. It has become the most common cosmetic treatment in the world and is easy to administer, has no downtime, produces long-lasting cosmetic effects, and has proven safe for decades ( Fig. e9.1 ![]() ).
).

Many abbreviations exist to describe botulinum toxin A. In the USA, there are three Food and Drug Administration (FDA)-approved neuromodulators that are described in detail later in this chapter. Onabotulinum toxin A is Botox, Incobotulinum is Xeomin, and Abobotulinum toxin is Dysport. Botox and Xeomin are diluted and used in an equipotent manner and in this chapter, the units are the same. Dysport is diluted differently and the units are not equipotent to Dysport and Xeomin. Throughout this chapter I refer to botulinum toxin A as BoNT-A, which is common scientific nomenclature. Since two out of three of these drugs are equipotent, I describe all units as “Botox units” or simply BoNT-A. Dysport is used in my practice 3 : 1 for Botox and Xeomin, so 1 Botox unit equals 3 Dysport units. All references forward will be “Botox” units or BoNT-A, unless otherwise specified.
Botulinum Toxin Type A: History and Physiology
Botulinum toxin is one of the most poisonous substances known on earth and it has been theorized that a gram of the pure toxin could kill one million people. Botulism was first described in Germany in the late 1700s after outbreaks of food poisoning from sausage. Botulus is the Latin word for “sausage” and hence the name of the toxin.
Many years later, Van Ermengem (1897) investigated an outbreak of botulism, involving 34 individuals who had consumed raw, salted ham, served at a gathering of amateur musicians in Ellezelles, Belgium. In the investigation of this outbreak, Van Ermengem established that botulism was an intoxication, not an infection, and that the toxin was produced by a spore-forming obligate anaerobic bacterium, Clostridium botulinum . He also found that toxin was rapidly inactivated by heating and was only toxic to certain animal species. In 1904, other strains of the toxin were identified.
A later outbreak in Darmstadt, Germany, associated with canned white beans, established that there was a second type of botulism. Physicians treating patients with botulism noticed xerostomia and xerophthalmia. Since the autonomic nervous system uses acetylcholine as the neurotransmitter, the idea of therapeutic use was put forth many years ago. As time would prove, the parasympathetic nervous system could be harnessed to treat such conditions as sialorrhea, hyperhidrosis, rhinitis, and sphincter spasms.
As the Clostridium bacterium was studied and the toxin isolated, it was largely controlled by the US government. Botulinum toxin A is a 900-kDa (kilodalton) neurotoxin protein complex, which is isolated and from bacteria and purified. The government permitted academic investigations in the late 1940s and Dr. Edward Schantz, who was employed by the chemical corps, began university research to continue the study. Dr. Allen Scott had the biggest part in the medical progression of the drug in the 1960s and 1970s and the FDA approved clinical trials of BoNT-A for strabismus in 1977. In the early 1980s the drug, called Oculinum at the time, was used in studies as a treatment for strabismus and blepharospasm, which were published in 1980. Dr. Jean Carruthers is an oculoplastic surgeon in Vancouver, BC, and was part of the research using BoNT-A for the treatment of blepharospasm. She noticed that the drug was successful in treating the muscular disorder, but one patient presented stating that her glabellar wrinkles were gone, which gave her a more pleasing appearance. Dr. Jean shared this experience with her husband, Dr. Alastair Carruthers, an accomplished dermatologist who was intrigued with this finding. Dr. Alastair Carruthers electively injected one of his employees in the glabellar region with the botulinum toxin, and the first cosmetic treatment in history was performed ( Fig. e9.2 ![]() ). This led to more trial patients and the first publication on cosmetic use of botulinum toxin for cosmetic treatments in 1992.
). This led to more trial patients and the first publication on cosmetic use of botulinum toxin for cosmetic treatments in 1992.

After significant investigation and trials, Botox (Onabotulinum toxin A) (Allergan Inc., Irvine, CA) was approved by the FDA in 1989 for the treatment of strabismus and blepharospasm and used off-label for cosmetic treatments. In the year 2000, the FDA approved Botox for cervical dystonia, and in the same year, botulinum toxin B (Solstice Neurosciences, Dublin, Ireland) was approved and marketed in the USA as Myobloc (rimabotulinumtoxinB). In 2002, Allergan achieved FDA approval of Botox for glabellar rhytids and in 2004, received FDA approval for the treatment of axillary hyperhidrosis. In 2009, Dysport (AbobotulinumtoxinA) (Ipsen Pharmaceuticals, Paris, France) entered the cosmetic market and in 2010 Xeomin (IncobotulinumtoxinA) was developed by Merz (Merz Pharma, Frankfurt, Germany). Currently, these are the only FDA-approved neuromodulators in the USA ( Fig. e9.3 ![]() ).
).

The LD50 for BoNT-A in mice is 1 unit and is expressed as the amount of toxin injected intraperitoneally that kills 50% of a group of Swiss–Webster female mice weighing 18–20 g. The LD50 for humans has been calculated at 2500–3000 units for a 70-kg person for a lethal dose of 40 U/kg. Since the usual therapeutic dose for the treatment of hyperfunctional muscle lines is 25–50 Botox units, a 100× margin of safety exists.
The three popular available FDA-approved neuromodulators have slightly different chemical structures, area of spread, and onsets of action. Basically, Botox and Xeomin are equipotent in terms of units. Although no official conversion ratio exists, I personally use three times the “Botox” units for Dysport. In an area that I would treat with 20 units of Botox, I would use 60 units of Dysport or 20 units of Xeomin. To keep things standard when describing units in this chapter I refer to “Botox” units or BoNT-A.
Botox and Dysport are stored in a conventional refrigerator and once reconstituted, stored in the same manner, while Xeomin does not require refrigeration. BoNT-A is ordinarily incapable of crossing the blood–brain barrier and generally exhibits no systemic effects. The neurotoxin exhibits its effects on the neuromuscular junction by inhibiting the release of acetylcholine (ACh) at the presynaptic neuron, which produces weakness or flaccid paralysis.
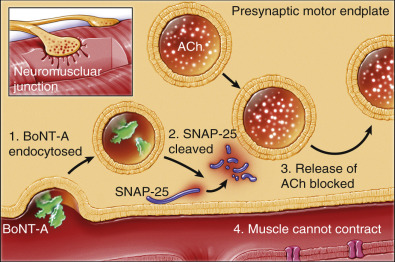
The physiology of the mechanism of action could fill multiple textbooks, as it includes extremely complex and numerous steps, reactions, activations, and deactivations. Put into the most basic explanation, when a neurotoxin is injected, the toxin enters the presynaptic nerve ending by endocytosis and the light chain of the BoNT-A molecule cleaves the SNARE proteins (SNAP-25) required for membrane fusion and ACh release. This prevents ACh from being released into the presynaptic cleft, which prevents the nerve from communicating with the muscle ( Fig. 9.1 ). The binding of the molecule to the motor endplate is permanent; it takes 24–48 h for the therapeutic condition of weakness or paralysis to ensue due to this chemical denervation. The reason for the delay is the time required for the storage vesicles of ACh within the presynaptic motor endplate to be depleted. Although the binding of the ACh is permanent, the paralytic effect only persists for 2–6 months.
The recovery phase of the presynaptic neuron occurs when axonal sprouts arise from feedback of the inactive muscle. The reactivation of acetylcholine release reestablishes the neuromuscular activity.
Resistance to botulinum toxin A (BTA) is rare and has been reported with repeated large doses of the exotoxin. Resistance from prolonged usage with strabismus treatments appears to increase with the use of >300 units within a 30-day period. Contraindications for BTA include known hypersensitivity to any component of the preparation (including human albumin), systemic neuromuscular diseases, or the use of aminoglycoside or spectinomycin antibiotics, which are known to effect neuromuscular transmission and potentiate the effects of BTA. Relative contraindications also include pregnancy and lactation.
Clinical Usage of Botulinum Toxin A
Before any patient is treated, it is imperative that they understand what a neurotoxin will or will not do. Some patients have unrealistic expectations. They may feel that all wrinkles are supposed to “go away” or that the treatment will be life-changing. Nothing is more important than a comprehensive informed consent. When a patient returns to the office and requests a refund because “my Botox did not work” or “I can still move my face,” it is very helpful to point them to their signed consent where drug resistance, no guarantee of result, or need for touchup at the patient’s expense was discussed.
Even though BoNT-A injections are the most popular cosmetic treatment in the world, many patients still do not understand the differences between neuromodulators and injectable fillers. As with all cosmetic procedures, the consent process is paramount for successful treatment and patient relations. It must be made clear in writing that neuromodulator treatments vary in effect and duration from patient to patient, and that some patients will not respond to treatment. The novice injector will soon find out that some patients will complain that their “Botox did not work” because they can still move their forehead, or the drug did not last long enough, or they had unwanted paralysis. The patient may expect a free touchup, retreatment, or a refund because their expectations were not met. For all these reasons, the patient must be made aware of the common effects, unwanted effects, expected duration or lack thereof, complications, patient and surgeon responsibilities, and any financial data that may be relevant. Although many doctors charge by the area, I prefer to charge by the unit. This makes treatment and retreatment simple and understandable for the patient. They are charged for what they receive, and touchups, when required, are simple math. In addition, some patients require more drugs than others because they have larger muscles or higher hairlines and that can complicate charging by the area.
I have been a Diamond level injector of Botox (top 3% of US injectors) for the past 7 years. I personally inject every patient myself and cherish this opportunity as well-spent doctor–patient relations time. There have been many Botox patients who turned into eyelid or facelift patients. Although many surgeons employ physician extenders to inject patients, I think they are missing great marketing and patient-relation opportunities. I also have a large group of local patients that come to my office because they are treated by a non-physician at other offices. Having said this, I personally know numerous nurses and PAs that are excellent injectors.
When I first began injecting Botox in the mid-1990s, the most common facial treatment areas were the glabella, frontalis, and lateral canthal region, in that order. Today the most commonly treated areas in my practice are the glabella, the lateral canthal regions, and the frontalis. In the early days of neurotoxins, patients wanted total paralysis and complained of any residual muscle movement. The frozen face appearance has fallen into disfavor and it is rare that any patient desires total forehead paralysis with the inability to raise the brow. Today, more and more patients present with customization requests. They desire “5 units here” and “3 units there.” Today, patients do not want to look unnatural and after 15 years’ experience they know exactly what they want and frequently self-direct treatment. This is fine with me as long as a patient realizes that treating an area with half of the traditional units will not produce the same effects and longevity as a full treatment. Patients requesting 8 units of Botox in the glabella cannot complain that they still have residual movement or that the result did not last 3 months.
Most patients present for multiple treatment areas, and most patients are regular users and average 90-day retreatments. The “rule of 3” is explained to all patients. The drug will start take effect by 3 days, will maximize by 3 weeks, and will last about 3 months. Obviously this is variable from patient to patient.
Injection Devices, Dilutions, and Caveats
Numerous pricing methods exist for neuromodulators and the average cost for Botox in my part of the USA ranges from US$10–13 per unit. Although the return on neuromodulators is high, there is significant cost in the product. There are also hidden costs in injection materials and vial waste.
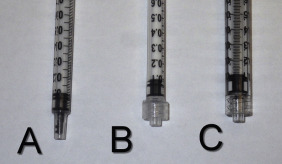
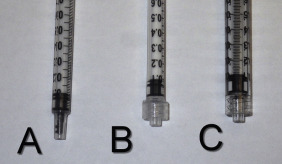
Numerous syringes exist for injecting neuromodulators and have varied costs depending on the syringe, hub, the presence of attached needles, and type of plunger ( Fig. 9.2 ). Some syringes also have plunger extensions that push the residual fluid out of the needle hub, which ensures more delivery and less waste ( Fig. 9.3 ). For high-volume injectors, syringes and needles can be a significant expense and vary dramatically in price. Syringe A in Fig. 9.3 costs 12 cents each; syringe B costs 21 cents per syringe; and syringe C costs 42 cents each (at time of writing).

Needle selection is also important. I am a firm believer that smaller needles cause less pain and make happier patients, which brings in more referrals. These advantages offset the increased expense of smaller needles. At time of writing, a 30-gauge needle can be purchased for as little as 7 cents; our 32-gauge needles cost 26 cents each, and our 33-gauge needles cost 36 cents each. Paying attention to expendables is an important part of remaining profitable. The standard in my office is 32-gauge 1.2-inch needles (TSK Steriject, Air-Tite Products, Inc., Virginia Beach, VA).
Some injectors prefer dedicated insulin syringes for neuromodulator injections ( Fig. 9.4 ). These are most useful for injectors who prefer a 1-mL dilution of Botox. When this is done, each insulin unit equals 1 Botox unit. This type of syringe is less useful for larger dilutions.

Dilution is an important part of delivering neurotoxins and is variable among clinicians. In my experience, the most common Botox dilution is 2.5 mL of preserved (bacteriostatic) saline per 100 unit Botox vial ( Fig. 9.5 ). This is a useful dilution for easy math. Diluting with 2.5 mL of preserved saline in a 100 unit vial will yield five syringes of 20 units, which is our most common dose. In reality, the 5th syringe has slightly less units from product waste. The actual product in a Botox vial is a thin precipitate on the bottom of the vial ( Fig. 9.6 ). Some novice injectors mistake this for an empty vial. This minute amount of drug underlines the potency of neurotoxins.


Xeomin is diluted in the same manner and the company stresses the need to gently roll and invert the vial to capture any toxin in the upper part of the vial.
I personally dilute Dysport with 3.0 mL of preserved saline, which provides six syringes of 60 Dysport units each. Again, 60 units is the amount we inject for the average treatment ( Fig. 9.7 ).

Allergan recommends that Botox solution should be discarded after 4 h, although some studies have shown that the effects are stable for up to 40 days. Many practitioners will keep reconstituted toxin in the refrigerator for several days or weeks without apparent loss of potency.
One of the main drawbacks existing today is the need for the practitioner to reconstitute the medication and draw it from the vial prior to injection. This inconvenience is accepted but inefficient in loss of time and money from the extra steps required. A more significant loss can result from residual neurotoxin that remains in the vial and cannot be drawn up through the stopper. It is impossible to capture 100% of the reconstituted toxin as there is liquid that, by capillary action, clings to the vial walls, stopper, syringe, and needle. This means that a small amount of waste is a given. In the business world, this is referred to as shrinkage. More importantly, the amount of this “waste” can vary by how the solution is removed from the vial.
The most common method of removing reconstituted product from the vial is to aspirate the liquid through the stopper. The Allergan Botox Cosmetic product brochure states “a new, sterile needle and syringe should be used to enter the vial on each occasion for removal of BOTOX.” Alternatively, some clinicians remove the stopper and aspirate from the vial base.
Conventionally, most people who draw from a vial have the stopper facing the floor, which means that surface area of the stopper and vial neck will harbor some liquid due to capillary action. When drawing from an upright vial with the stopper removed and the vial tilted 30 degrees, there is less surface area for residual liquid to adhere, plus the tilting of the vial allows one to get the last drop from the remaining puddle. A large-bore needle with a long bevel may not capture the total residual puddle, whereas a 32-gauge needle on a 1-mL syringe can aspirate the total residual. If the unstoppered vial is sitting level on its base, it may be impossible to see the residual and tipping the vial 30 degrees will reveal any residual amount.
When observing the vials shown in Fig. e9.1 ![]() , it is apparent that some residual fluid remains in most vials, which translates into wasted product, inaccurate injection delivery, and lost income.
, it is apparent that some residual fluid remains in most vials, which translates into wasted product, inaccurate injection delivery, and lost income.
In an informal effort to quantify how much residual neurotoxin remains in an average vial when drawn through the stopper, I randomly collected “empty” vials from my collection ( Fig. e9.1 ![]() ). I chose 50 vials (100 unit) and numbered them. The top was removed from each vial using a home-style bottleopener or bandage super scissors ( Fig. e9.4
). I chose 50 vials (100 unit) and numbered them. The top was removed from each vial using a home-style bottleopener or bandage super scissors ( Fig. e9.4 ![]() ). Care was taken to only engage the metal vial rim, so as not to fragment glass or displace the stopper. Each vial was tilted 30 degrees from vertical so that the residual liquid could be visualized, then it was aspirated with a 1-mL Luer Lock syringe and a 32-gauge needle ( Fig. e9.5
). Care was taken to only engage the metal vial rim, so as not to fragment glass or displace the stopper. Each vial was tilted 30 degrees from vertical so that the residual liquid could be visualized, then it was aspirated with a 1-mL Luer Lock syringe and a 32-gauge needle ( Fig. e9.5 ![]() ). As stated above, it is important to use the smallest needle possible when aspirating the last aliquot of residual liquid, as larger needles have a long bevel that cannot get to the bottom of the residual puddle and their larger-diameter needle will retain a small amount of residual liquid. The residual liquid was drawn up into the syringe and purged, so the liquid was at the “zero” measurement line on the syringe. Fig. 9.8 shows a 10-vial sample.
). As stated above, it is important to use the smallest needle possible when aspirating the last aliquot of residual liquid, as larger needles have a long bevel that cannot get to the bottom of the residual puddle and their larger-diameter needle will retain a small amount of residual liquid. The residual liquid was drawn up into the syringe and purged, so the liquid was at the “zero” measurement line on the syringe. Fig. 9.8 shows a 10-vial sample.



The results show that our technique of aspirating through the stopper with an 18-gauge needle will leave an average residual volume of 0.127 mL, which corresponds to 5.08 units of residual waste per vial at my dilution of 2.5 mL/vial. This represents a 5% waste of product per vial. A smaller dilution would be more concentrated and allow even more waste.
Extrapolating the residual waste of 5.08 units per vial, the year of the study (as a solo injector) I used 615 vials, which equals 3124 units. At my fee of $10 per unit, my loss in 2012 was $31,242. Since we double the product cost, my actual profit loss in 2012 was $15,621.
The price of a vial of Botox when I began injecting was $325 a vial and since 2008 has stayed at $525 per vial. If I used today’s pricing against my 5000 vials this would equal a loss of 25,400 units, which would be a loss of $254,000. Factoring a 50% product cost, my net profit loss would be $127,000! It is hard to believe that I could have added $127,000 to the bottom line by merely removing the stopper from the vials when reconstituting. This is certainly worth the effort. As this study was done several years ago, these numbers would be even higher today. The financial advantage of removing the stopper and aspirating the neurotoxin from the base of the vial is obvious.
Injection Devices, Dilutions, and Caveats
Numerous pricing methods exist for neuromodulators and the average cost for Botox in my part of the USA ranges from US$10–13 per unit. Although the return on neuromodulators is high, there is significant cost in the product. There are also hidden costs in injection materials and vial waste.
Numerous syringes exist for injecting neuromodulators and have varied costs depending on the syringe, hub, the presence of attached needles, and type of plunger ( Fig. 9.2 ). Some syringes also have plunger extensions that push the residual fluid out of the needle hub, which ensures more delivery and less waste ( Fig. 9.3 ). For high-volume injectors, syringes and needles can be a significant expense and vary dramatically in price. Syringe A in Fig. 9.3 costs 12 cents each; syringe B costs 21 cents per syringe; and syringe C costs 42 cents each (at time of writing).

Needle selection is also important. I am a firm believer that smaller needles cause less pain and make happier patients, which brings in more referrals. These advantages offset the increased expense of smaller needles. At time of writing, a 30-gauge needle can be purchased for as little as 7 cents; our 32-gauge needles cost 26 cents each, and our 33-gauge needles cost 36 cents each. Paying attention to expendables is an important part of remaining profitable. The standard in my office is 32-gauge 1.2-inch needles (TSK Steriject, Air-Tite Products, Inc., Virginia Beach, VA).
Some injectors prefer dedicated insulin syringes for neuromodulator injections ( Fig. 9.4 ). These are most useful for injectors who prefer a 1-mL dilution of Botox. When this is done, each insulin unit equals 1 Botox unit. This type of syringe is less useful for larger dilutions.

Dilution is an important part of delivering neurotoxins and is variable among clinicians. In my experience, the most common Botox dilution is 2.5 mL of preserved (bacteriostatic) saline per 100 unit Botox vial ( Fig. 9.5 ). This is a useful dilution for easy math. Diluting with 2.5 mL of preserved saline in a 100 unit vial will yield five syringes of 20 units, which is our most common dose. In reality, the 5th syringe has slightly less units from product waste. The actual product in a Botox vial is a thin precipitate on the bottom of the vial ( Fig. 9.6 ). Some novice injectors mistake this for an empty vial. This minute amount of drug underlines the potency of neurotoxins.


Xeomin is diluted in the same manner and the company stresses the need to gently roll and invert the vial to capture any toxin in the upper part of the vial.
I personally dilute Dysport with 3.0 mL of preserved saline, which provides six syringes of 60 Dysport units each. Again, 60 units is the amount we inject for the average treatment ( Fig. 9.7 ).

Allergan recommends that Botox solution should be discarded after 4 h, although some studies have shown that the effects are stable for up to 40 days. Many practitioners will keep reconstituted toxin in the refrigerator for several days or weeks without apparent loss of potency.
One of the main drawbacks existing today is the need for the practitioner to reconstitute the medication and draw it from the vial prior to injection. This inconvenience is accepted but inefficient in loss of time and money from the extra steps required. A more significant loss can result from residual neurotoxin that remains in the vial and cannot be drawn up through the stopper. It is impossible to capture 100% of the reconstituted toxin as there is liquid that, by capillary action, clings to the vial walls, stopper, syringe, and needle. This means that a small amount of waste is a given. In the business world, this is referred to as shrinkage. More importantly, the amount of this “waste” can vary by how the solution is removed from the vial.
The most common method of removing reconstituted product from the vial is to aspirate the liquid through the stopper. The Allergan Botox Cosmetic product brochure states “a new, sterile needle and syringe should be used to enter the vial on each occasion for removal of BOTOX.” Alternatively, some clinicians remove the stopper and aspirate from the vial base.
Conventionally, most people who draw from a vial have the stopper facing the floor, which means that surface area of the stopper and vial neck will harbor some liquid due to capillary action. When drawing from an upright vial with the stopper removed and the vial tilted 30 degrees, there is less surface area for residual liquid to adhere, plus the tilting of the vial allows one to get the last drop from the remaining puddle. A large-bore needle with a long bevel may not capture the total residual puddle, whereas a 32-gauge needle on a 1-mL syringe can aspirate the total residual. If the unstoppered vial is sitting level on its base, it may be impossible to see the residual and tipping the vial 30 degrees will reveal any residual amount.
When observing the vials shown in Fig. e9.1 ![]() , it is apparent that some residual fluid remains in most vials, which translates into wasted product, inaccurate injection delivery, and lost income.
, it is apparent that some residual fluid remains in most vials, which translates into wasted product, inaccurate injection delivery, and lost income.
In an informal effort to quantify how much residual neurotoxin remains in an average vial when drawn through the stopper, I randomly collected “empty” vials from my collection ( Fig. e9.1 ![]() ). I chose 50 vials (100 unit) and numbered them. The top was removed from each vial using a home-style bottleopener or bandage super scissors ( Fig. e9.4
). I chose 50 vials (100 unit) and numbered them. The top was removed from each vial using a home-style bottleopener or bandage super scissors ( Fig. e9.4 ![]() ). Care was taken to only engage the metal vial rim, so as not to fragment glass or displace the stopper. Each vial was tilted 30 degrees from vertical so that the residual liquid could be visualized, then it was aspirated with a 1-mL Luer Lock syringe and a 32-gauge needle ( Fig. e9.5
). Care was taken to only engage the metal vial rim, so as not to fragment glass or displace the stopper. Each vial was tilted 30 degrees from vertical so that the residual liquid could be visualized, then it was aspirated with a 1-mL Luer Lock syringe and a 32-gauge needle ( Fig. e9.5 ![]() ). As stated above, it is important to use the smallest needle possible when aspirating the last aliquot of residual liquid, as larger needles have a long bevel that cannot get to the bottom of the residual puddle and their larger-diameter needle will retain a small amount of residual liquid. The residual liquid was drawn up into the syringe and purged, so the liquid was at the “zero” measurement line on the syringe. Fig. 9.8 shows a 10-vial sample.
). As stated above, it is important to use the smallest needle possible when aspirating the last aliquot of residual liquid, as larger needles have a long bevel that cannot get to the bottom of the residual puddle and their larger-diameter needle will retain a small amount of residual liquid. The residual liquid was drawn up into the syringe and purged, so the liquid was at the “zero” measurement line on the syringe. Fig. 9.8 shows a 10-vial sample.



The results show that our technique of aspirating through the stopper with an 18-gauge needle will leave an average residual volume of 0.127 mL, which corresponds to 5.08 units of residual waste per vial at my dilution of 2.5 mL/vial. This represents a 5% waste of product per vial. A smaller dilution would be more concentrated and allow even more waste.
Extrapolating the residual waste of 5.08 units per vial, the year of the study (as a solo injector) I used 615 vials, which equals 3124 units. At my fee of $10 per unit, my loss in 2012 was $31,242. Since we double the product cost, my actual profit loss in 2012 was $15,621.
The price of a vial of Botox when I began injecting was $325 a vial and since 2008 has stayed at $525 per vial. If I used today’s pricing against my 5000 vials this would equal a loss of 25,400 units, which would be a loss of $254,000. Factoring a 50% product cost, my net profit loss would be $127,000! It is hard to believe that I could have added $127,000 to the bottom line by merely removing the stopper from the vials when reconstituting. This is certainly worth the effort. As this study was done several years ago, these numbers would be even higher today. The financial advantage of removing the stopper and aspirating the neurotoxin from the base of the vial is obvious.
Pain Control
Although most head and neck treatments are not painful, no patient looks forward to multiple needlesticks. Popular means of improving injection pain include topical anesthetic creams or preinjection icepacks. Vibratory devices have been used with injections for many years. They primarily serve as a diversion to the injection but offer some physiologic pain relief through the gate theory of pain control. In a simplified explanation, when a distractive stimulus (vibratory device) is applied at the same time as a noxious stimulus (the needle), the inhibitor neurons can attenuate the pain stimulus to the thalamus. Whether science or distraction, or a combination of the two are responsible for decreased pain, I am a true believer in the concept. I began using a lighted vibratory device (Blaine Labs, Santa Fe Springs, CA) around 2010 ( Fig. 9.9 ). At first, patients were skeptical of the concept but quickly appreciated the difference. I have personally had the device used on my own injections and can vouch for its effectiveness. After using this (or similar) device for a number of years, patients demand it for treatment. An informal survey has yielded a 97% rate of patients that request the vibratory device after initial use. The first question that most patients ask before treatment is, “Where is your buzzer?” The device not only provides vibration, but has a light to illuminate the region treated. Its ergonomic shape is handy to use as a retractor to lift and stretch tissues when injecting, which is especially useful in regions such as crow’s feet. This device has become a mainstay of my injectable treatment, as I also use it for pre-filler local anesthesia injection.

An excellent technological advance was made with the AccuVein vein viewing system (AccuVein Inc, Huntington, NY) ( Fig. 9.10 ). The AccuVein AV400 digitally displays a map of the vasculature on the surface of the skin in real-time, allowing clinicians to verify vein position and patency as well as avoid valves or bifurcations. It is handheld and lightweight, weighing only 9.7 ounces (275 g), and easily converts to hands-free with the use of optional wheeled or fixed stands. The device is battery operated and energizes on a battery stand. The AccuVein works by projecting a visible and invisible laser beam, which passes through a microprocessor then displays the veins on the skin surface. With center line accuracy to the width of a human hair, the AV400 can detect veins up to 10 mm deep. There is a saying with neuromodulators and fillers, “If you bruise them, you lose them” and no surgeon or patient is ever happy with a long-lasting unsightly bruise after a simple elective treatment. This device has been useful for avoiding veins, especially in the lateral canthal region and is also used for filler injection. The AccuVein and the Blaine vibratory device also add a marketing perspective to treatments, as patients appreciate technology that improves the experience. This device is also very useful for locating veins for difficult venipuncture and for surgeons that treat leg veins.

Treatment Regions
Regardless of the area I am treating, I never adhere to the old wives’ tales such as, “You can’t lay down for 4 h after receiving neurotoxin treatment,” “You can’t exercise that day,” “You can’t fly in a plane that day,” etc. I tell my patients to do whatever they wish and I inject many patients on the way to the gym, tennis match, and traveling flight crews. In terms of lying down, a glabellar injection would more likely gravitationally diffuse to the levator palpebrae superioris while standing as opposed to lying. I believe these are urban myths from the earliest days of neuromodulator injection.
Upper Face
Enhanced and expanded injection applications for neuromodulators have extended treatment to many areas of the head and neck (and body) and all injectors must have a firm understanding of cervicofacial musculature. The muscles of facial expression are all paired structures and have bony origins and dermal insertions, which in turn, move the facial skin. Wrinkles (rhytids) form perpendicular to the muscle movement.
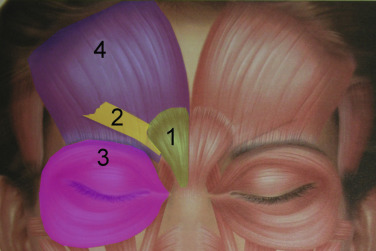
The main depressors of the brow are the paired procerus, corrugator supercilii, and medial orbicularis oculi muscles. The sole elevator of the brow is the paired frontalis muscle ( Fig. 9.11 ). This musculature works in conjunction to perform the very complex orchestra of facial expression.
Mimetic muscles commonly interdigitate, and in some areas (glabella, modiolus) are interfaced with numerous muscles. These muscles, through continual flexing of the skin, produce rhytids perpendicular to the muscular action. With years of muscular movement, the frown lines, horizontal forehead wrinkles, and lateral canthal (crow’s feet) wrinkles become deeper and more noticeable. Theoretically, if there is no muscle movement, rhytids do not form, as evidenced in patients with stroke or nerve injury. Taking this into account, the younger a patient begins to receive neurotoxin treatment, the less chance they have of forming wrinkles. For those patients with existing wrinkles, regularly paralyzing the muscles has a preventive effect.
Treatment of Dynamic Rhytids
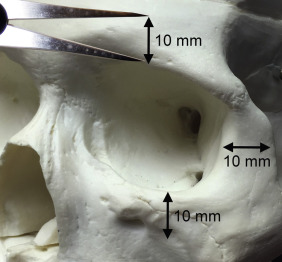
The procerus, corrugators, and medial orbicularis collectively produce the common “frown lines” in the central brow region. The two creases seen in this area are frequently referred to as the “11” or the “111” in cases of a triple crease. The common injection pattern of this region involves five injections placed in a manner to decrease contraction of the depressors. The most important pearl when injecting in the periorbital region is to keep all injections 1 cm from the bony orbital rim. Some injectors choose to inject closer to the orbit, but I can testify from tens of thousands of injections that staying 10 mm from the bony orbit has prevented a true eyelid ptosis in my career ( Fig. 9.12 ). I have, however, seen it happen to other injectors when neurotoxin is injected too close to the orbital rim. For the novice injector, it is a good idea to mark out the points of injection with a surgical marker and a ruler or caliper prior to injecting.
When considering needle placement, it is important to keep in mind that the offending muscles are not necessarily directly under the wrinkle. Because of variances among patients, the most accurate way to inject is to ask the patient to animate the area to be injected and observe the main area(s) of muscle action. Injecting in the main area(s) of muscle recruitment is the preferable location for injection. For experienced injectors, the glabellar, frontalis, and lateral canthal region injections are almost standardized. The area of maximum muscle contraction is generally consistent, and by injecting in a common pattern, the average person can be injected without flexing for the injector. It is, however, helpful to have patients animate to view their exact activity for greatest precision.
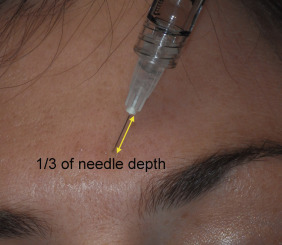
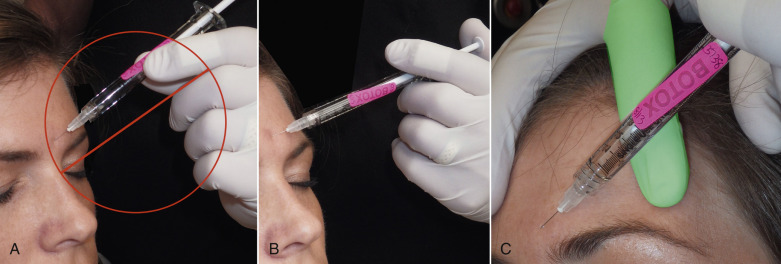
A common question from novice injectors is: “At what level is the neurotoxin injected?” Neuromodulators should be injected intramuscularly, since that is the site of intended drug action. Early accounts instructed injectors to insert the needle to periosteum and then draw back half the way. This is a poor practice for several reasons. The periosteum is innervated, it is painful, and it also will dull the needle quickly. The mimetic muscles are subcutaneous with dermal insertions and are superficial. Depending upon the amount of subcutaneous fat in the region, the muscle mass can be shallower or deeper. A general rule is to insert the half-inch needle about one-third of its length for the average patient ( Fig. 9.13 ). In reality, neurotoxins have a great affinity for presynaptic neuron and even if injected intradermally, will generally produce the desired effect. A common mistake of novice injectors (especially those used to giving intramuscular injections on the body) is to hold the syringe between their index finger and thumb, similar to holding a pencil. They puncture the skin and then have to re-grasp the inserted syringe to find the plunger, which is an awkward maneuver. It is better to inject with the thumb on the plunger and the index and second fingers on the hilt of the syringe. Another way to stabilize the syringe for accuracy is to use the index finger of the other hand as a guide in the same manner on uses a pool cue ( Fig. 9.14 ).
Frontalis Treatment
For the sake of order, I will describe the most common treatment areas from top to bottom beginning with the frontalis. Again, this is a paired muscle and some patients do not have any muscle in the upper midline, although I generally spread injections equally across the forehead. Treating the frontalis requires thinking and planning, as it has a big effect on brow posture and activity. In the early days of neurotoxins, total paralysis of the frontalis was vogue but is very undesirable in most contemporary patients. In younger patients with little or no eyelid skin excess, overtreatment of the frontalis is not a major problem and only affects animation. In older patients with significant brow ptosis and/or excessive upper-eyelid skin, frontalis overtreatment can be much more problematic, especially in females ( Fig. 9.15 ). Many of these patients unconsciously raise their brows to improve their visual field and to look younger ( Fig. 9.16 ). It is frequently a subconscious gesture similar to a patient with a recessive chin extending their mandible or short people standing up straighter to appear taller. Females with excessive upper-lid skin are well aware that they have to hyper-elevate their brows to put on eye shadow or eyeliner. If the frontalis is overtreated in these individuals it can bother them beyond comprehension. Dropping or paralyzing the brow and lids in one of these patients can bring out their wrath. If this happens, the surgeon will get a call about 72 h after treatment, usually when the patient is applying makeup. When they look in the mirror, they cannot elevate their brows and they see the increased skin excess and become disproportionately angry because it makes them look older. I realize that my description of this is dramatic, but I have seen this numerous times and can verify their anger. They become even angrier when they are told that there is no reversing treatment other than to allow the neuromodulator to wear off. Understanding this, it is best to examine the amount of brow ptosis or dermatochalasis in patients and discuss this possibility pre-injection. It is also important for the written informed consent to detail this situation. This is especially important for patients who have not been treated before or are new to the surgeon. Due to the aforementioned problems along with the fact that the paralyzed appearance is out of vogue, the frontalis should be treated conservatively. The biggest change I have made with my patients over the years is injection of 10–15 Botox units for frontalis treatment, whereas in the past I used to inject 20–25 units.










