Nasolacrimal Duct Obstruction
Emily M. Zepeda
Sarah M. Jacobs
Christopher B. Chambers
DEFINITION
Nasolacrimal duct obstruction (NLDO) is an obstruction that occurs within the duct of the nasolacrimal system, such that tears and mucus that have passed through the lacrimal sac are unable to appropriately drain into the nose.
NLDO results in varying degrees of epiphora (tearing) and is often associated with mucopurulent discharge, swelling, and pain.
ANATOMY (LACRIMAL SYSTEM)
The nasolacrimal duct is a part of the lacrimal drainage system that conveys tears from the ocular surface to drain into the nose (FIG 1).
It is about 15 mm long, starting at the terminus of the nasolacrimal sac.
The nasolacrimal duct passes inferiorly, posteriorly, and laterally within the canal formed by the maxillary and lacrimal bones. It travels into the inferior meatus and opens under the inferior turbinate. Its outflow is partially covered by the valve of Hasner.
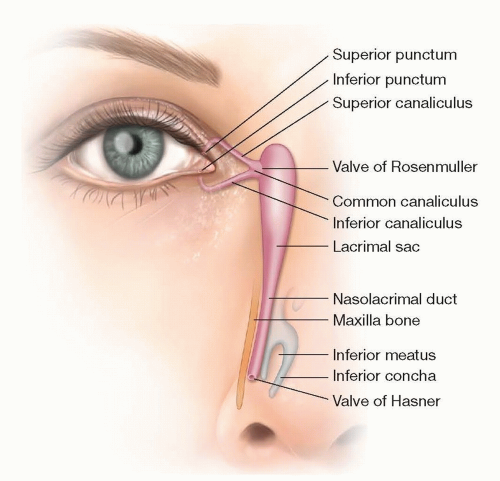 FIG 1 • Anatomy of the nasolacrimal system, which allows tears from the eye to pass through the puncta, canaliculi, and lacrimal sac, through the nasolacrimal duct to drain into the nasal cavity. |
PATHOGENESIS
NLDO can occur secondary to congenital or acquired disease.
Congenital NLDO is usually secondary to a membrane blocking the valve of Hasner at the nasal end of the NLD.
Obstructions become clinically evident in only 2% to 6% of full-term infants at 3 to 4 weeks of age.
Conservative management options of congenital NLDO consist of observation, lacrimal sac massage, and topical/oral antibiotics. It is estimated that 90% of symptomatic congenital NLDO resolves in the first year of life with conservative management.
For the remaining 10% of these cases, probing of the NLD can be curative by creating an opening through the imperforate valve of Hasner.1
Infants with craniofacial deformity or Down syndrome are also at higher risk of congenital NLDO. Dacryocystoceles can also create an obstructive process, leading to enlargement and potentially abscess of the lacrimal sac.
Acquired NLDO may arise from numerous causes such as facial trauma, sinus disease, chronic allergy and inflammation, radiation treatment to the midface, toxicity from chemotherapeutic agents or radioactive iodine, or following sinonasal surgery. Involutional stenosis is the most common cause of NLDO in adults.
Regardless of whether NLDO is congenital or acquired, any obstruction of the nasolacrimal outflow is capable of causing stagnation of bacteria leading to infection of the lacrimal sac known as dacryocystitis.
PATIENT HISTORY AND PHYSICAL FINDINGS
In both congenital and acquired NLDO, the primary symptom is epiphora as a result of backflow of tears due to blockage of the duct.
At times, enough tear and mucous volume is accumulated within the lacrimal sac that there is a palpable or visible enlargement of the sac. Light pressure over the area of the lacrimal sac can often cause mucopurulent discharge to reflux through the lacrimal drainage system and out the puncta.
Evaluation of a patient who presents with epiphora should focus on determining the underlying etiology of tearing, assessing for nonobstructive causes (eg, ectropion, reflex tearing, conjunctival infection or inflammation) and nonbenign entities (eg, nasolacrimal malignancy, granulomatosis with polyangiitis). Elements of the history and exam with this focus in mind include the following:
A history including duration since tearing onset, percentage of the day it occurs, how it interferes with activities of
daily living, and whether any particular activities provoke it (eg, cold, heat, wind, visual tasks such as computers or reading). Any history of facial trauma, prior episodes of dacryocystitis, radiation, or chemotherapy should be elicited. The patient should also be asked about bloody tears, which would be a concerning sign for underlying malignancy.
Prior to instilling any eye drops, the tear meniscus height should be noted, and the tear breakup time should be measured, as a cue to whether dry eye-related reflex tearing is contributing to the patient’s epiphora.
Eyelid structures and position in relation to the globe should be assessed for concurrent disease states such as ectropion, entropion, and trichiasis. The upper and lower puncta should be examined for patency and position relative to the globe. Lower lid tone should be evaluated for degree of laxity.
A dye disappearance test can be performed on patients of any age. A fluorescein eye drop is instilled in each eye. Normal nasolacrimal drainage will allow the dye to flow through the punctum, such that the yellow dye disappears from the ocular surface in a matter of minutes. Patients with nasolacrimal outflow obstruction show delayed clearance of fluorescein.
In adults, the lacrimal system should be probed and irrigated. Passage of saline into the nose and throat with ease and no reflux signifies a patent system. Reflux of irrigant signifies obstruction, and the pattern of reflux can reveal where the obstruction is located within the system. Reflux from the same punctum that is being irrigated indicated obstruction within the canaliculus. Reflux from the opposite punctum without mucous indicates obstruction at the common canaliculus. Reflux from the opposite punctum with mucus indicates obstruction in the nasolacrimal sac or duct.
Periocular skin may show erythema, edema, and breakdown of superficial tissues when the discharge or tearing is profuse and constant.
Finally, nasal evaluation should be performed. This may reveal deviated septum, polyposis, or tumors as a cause of obstruction. Nasal mucosa may also show erythema and edema indicating chronic sinus inflammation.
DIFFERENTIAL DIAGNOSIS
Congenital glaucoma: When the only symptom is epiphora in a child, one must always rule out congenital glaucoma. The classic triad for congenital glaucoma is blepharospasm (involuntary squeezing of the eyelids closed), photophobia (uncomfortable sensitivity to light), and epiphora. Other findings suggestive of glaucoma include buphthalmos (enlarged globe and corneal diameter) and Haab striae (breaks in the innermost layer of the cornea, leading to corneal haze). If concern for congenital glaucoma exists, the child should be referred to pediatric ophthalmology.
Dry eye: Epiphora due to dry eye will typically occur when the patient is engaged in a visual task such as reading or computer usage, which decreases their blink rate and exacerbates the dryness of the ocular surface. The patient experiences blurring, burning or foreign body sensation, and then tear flow. Symptoms are worse in hot, dry, or windy conditions.
Trichiasis: Growth of eyelashes from malrotated lash follicles or metaplastic Meibomian oil gland orifices results in lashes rubbing and irritating the ocular surface, which provokes tearing. Penlight exam can locate these lashes, which can be treated with epilation or more permanent methods such as cryotherapy or radiofrequency ablation.
Conjunctivitis: Infection or inflammation of the conjunctiva can cause epiphora and ocular discharge. On examination, patients with conjunctivitis will show injection and papillae or follicles, which appear as fine bumps on the normally smooth conjunctival surface.
Eyelid ectropion or entropion: Poor eyelid position or lax lower eyelid tone can lead to epiphora. An eyelid with normal tone smoothly sweeps the tears across the ocular surface with each blink, pumping them down the punctal drains into the lacrimal sac. Lax eyelids that are rotated outward (ectropion) or inward (entropion) cannot serve this function effectively, so the unpumped tears spill over the lid margin onto the cheeks.
IMAGING
The diagnosis of NLDO is based on patient history, elevated tear meniscus, and obstruction observed when the system is probed and irrigated. Imaging is not often needed for diagnosis.
In select cases, maxillofacial computed tomography (CT) and magnetic resonance (MRI) scans are helpful to evaluate the anatomy after craniofacial injury, in patients with significant sinus or nasal disease, or to evaluate for neoplasia.
Less commonly, two methods for specific mapping of the lacrimal drainage system itself can be employed:
In contrast, dacryocystography, in which dye is injected into the punctum and CT or MRI imaging, is used to define the anatomic details of the lacrimal drainage system outlined by the contrast agent, allowing precise location of the obstructed site(s).
Dacryoscintigraphy uses radionucleotide eye drops to follow tear flow as a gamma camera takes multiple pictures of the outflow system.
SURGICAL MANAGEMENT
As mentioned, most congenital NLDO resolves with nonsurgical management.
Approximately 10% of children with congenital NLDO require probing of the duct. A small subset of those may require repeat probing with balloon dilation of the duct, infracture of the inferior turbinate, and/or placement of silicone stents within the nasolacrimal system to relieve their obstruction.
Because of the high success rate with these methods, dacryocystorhinostomy (DCR) is rarely needed in the pediatric population. It is reserved for children who have persistent tearing following intubation, recurrent dacryocystitis, or craniofacial abnormalities with bony obstruction of the duct.
In adults, however, DCR is the preferred primary surgery for NLDO after the other causes of tearing have been eliminated or addressed.
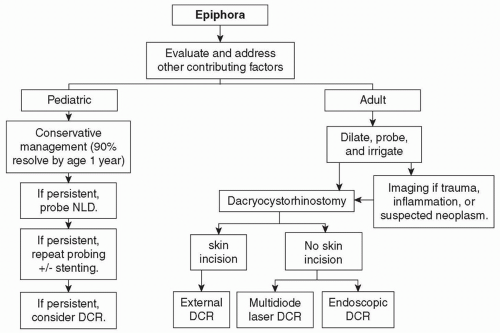
FIG 2 • Algorithm for management of epiphora due to nasolacrimal duct obstruction.
External DCR: An incision is made through the skin overlying the lacrimal sac, allowing external access to the lacrimal sac fossa for bone removal, sac opening, and stent placement under direct visualization without the need for endoscopic camera equipment.
Literature reports a slightly higher success rate with the external approach in certain studies. When appropriately placed, the incision heals with a very subtle and cosmetically acceptable scar.
Internal DCR (also known as endonasal or endoscopic DCR): Attention is brought to the middle meatus, which allows the most direct access to the lacrimal sac fossa so that the nasolacrimal duct can be bypassed. The middle meatus is visualized from within the nasal cavity, allowing removal of the nasal mucosa and the bone encasing the lacrimal sac from the inside, following by opening of the sac and retrieval of the stents.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree