Nasal Tip Hemangioma
Terence Kwan-Wong
Jugpal S. Arneja
DEFINITION
Infantile hemangiomas is a benign, proliferative, vascular tumor of infancy that has a defined, although unpredictable natural history.
Infantile hemangiomas is the most common pediatric benign tumor, affecting between 4% and 10% of children in their 1st year of life.1
Approximately 60% of infantile hemangiomas involve the head and neck regions,2 and of these, a small percentage affect the nose.
Nasal tip hemangioma can cause significant deformity, affecting the psychological and emotional well-being of the patient and the family.
ANATOMY
Nasal contour is determined by draping of the nasal skin over a framework formed by the nasal bones in the cephalic third, by the upper lateral cartilages in the middle third, and by the paired lower lateral cartilages and the caudal septum in the caudal third.
Nasal tip hemangioma usually resides in a subcutaneous plane—although cutaneous manifestations are not uncommon— and can extend between the medial crura of the lower lateral cartilages and occasionally into the columellar region as well.3,4
Hemangioma extending between the lower lateral cartilages tends to splay the medial and middle crura of the lower lateral cartilages from each other and can occasionally dislocate the lower lateral cartilages, by displacing the cephalic edge of the cartilage into the nasal passage.
PATHOGENESIS
Infantile hemangiomas is histologically characterized by proliferating endothelial cells with varying luminal sizes, which tend to be smaller during the proliferative phase, becoming larger during the involutional phase.
Involution is reflected by slowing of endothelial proliferation, apoptosis of existing endothelial cells, and replacement of vascular tissue with adipocytes and connective tissue.
NATURAL HISTORY
Infantile hemangiomas is not present at birth but becomes apparent within the first few weeks of life.
The natural course of infantile hemangioma is relatively predictable:
The proliferative phase (0 to 1 year) is characterized by rapid growth.
The involutional phase (until 7 to 10 years) when the hemangioma shrinks and fades
Nasal tip hemangiomas is slower to regress than those in other parts of the body.
Involutional phase (greater than 10 years) when the involutional process has completed
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough history should be obtained, including information about onset, progression, prior treatments, and symptoms of the nasal tip hemangioma.
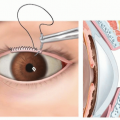
Physical examination (FIG 1)
Local—size, location, distortion of nasal cartilages, involvement of nasal vault, skin quality, presence of any scars, signs of active infection, ulceration.
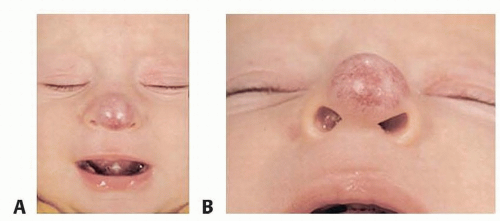
FIG 1 • A,B. A bulbous, pigmented hemangioma is evident at 6 months of age. (Reprinted from Arneja JS, Chim H, Drolet B, Gosain AK. The “Cyrano nose”: refinements in surgical technique and treatment approach to hemangiomas of the nasal tip. Plast Reconstr Surg. 2010;126:1291, with permission.)
Regional—determine presence of any other lesions. Assess for any airway, visual, or auditory involvement that may necessitate earlier intervention.
Systemic—rare with isolated infantile hemangioma of the nasal tip
Beardlike distribution may indicate airway involvement.
Large plaquelike distributions may suggest PHACES syndrome.
IMAGING
Imaging is usually not required.
Ultrasound may be useful to delineate flow within and the depth of the lesion.
MRI may be used to delineate the extent of the hemangioma and its relation to the underlying nasal framework.
DIFFERENTIAL DIAGNOSIS
Hemangioma
Vascular malformation (lymphatic, venous, arteriovenous)
Dermoid cyst
NONOPERATIVE MANAGEMENT
Nonoperative options are usually considered as adjunctive rather than definitive treatments.
Propranolol is first-line medical therapy, and many practitioners feel this medication to be superior to oral corticosteroid treatment alone.
Dosing—1 to 3 mg/kg/d divided into TID dosing
Rare complications include hypoglycemia and limb cyanosis, while almost never bronchospasm and hypotension.
Oral or intralesional steroid therapy ideally is used during proliferative phase (FIG 2). Steroid therapy can be administered for up to three treatment cycles.
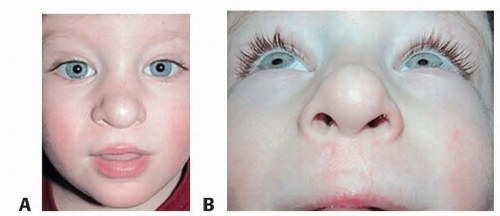
FIG 2 • A,B. After completion of treatment with intralesional steroids and pulsed dye laser therapy, the lesion has decreased in size and cutaneous manifestations have resolved in the patient in FIG 1, shown here at age 3 years. (Reprinted from Arneja JS, Chim H, Drolet B, Gosain AK. The “Cyrano nose”: refinements in surgical technique and treatment approach to hemangiomas of the nasal tip. Plast Reconstr Surg. 2010;126:1291, with permission.)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access