Nasal Septal Hematoma
Whitney Laurel Quong
Jugpal S. Arneja
DEFINITION
Hematoma of the nasal septum is a relatively rare, yet potentially serious consequence of trauma to the nose where blood accumulates between the cartilaginous/bony portion of the septum, and its overlying mucoperichondrium/mucoperiosteum. Any degree of craniofacial trauma should urge evaluation for the condition.
Without prompt recognition and intervention, a septal hematoma may precipitate future cosmetic distortion, including secondary infection, resulting in septal abscess and/or ultimately a saddle nose deformity.
Incision and drainage is the mainstay of treatment, but immediate reconstruction with autograft or homograft is an option if there is structural defect in the nasal septum.
ANATOMY
The nasal septum comprises cartilaginous, membranous, and bony components (perpendicular plate of the ethmoid, vomer, premaxilla, maxillary crest, and palatine crest) covered by mucoperichondrium and mucoperiosteum layers (FIG 1). The septum is typically 2 to 4 mm thick.
The blood supply of the nasal septum is derived from the sphenopalatine and the anterior and posterior ethmoid arteries, along with contributions from the superior labial artery (anteriorly) and the greater palatine artery (posteriorly). These vessels travel in the overlying mucous membrane and penetrate the mucoperichondrium through vascular canals. It is through diffusion that the cartilaginous septum receives its blood supply. The Kiesselbach plexus (Little area) is a region where the chief blood supplies to the internal nose converge and is found in the anteroinferior third of the nasal septum.
Bleeding into the potential space between the cartilage and its overlying mucoperichondrium leads to a septal hematoma (FIG 2), whereas external bleeding from Kiesselbach plexus results in epistaxis.
PATHOGENESIS
Nasal septal hematoma typically results from trauma to the nasal complex, with even minor trauma causing the condition. Rarely, chronic irritation of the septum by nasogastric tube has also been found to precipitate the condition.1
Children are particularly prone to developing septal hematomas, as the pediatric cartilage is soft and prone to buckling,2 and the mucoperichondrium is only loosely adherent to the underlying cartilage.1
The precise mechanism for development of nasal septal hematoma has not been defined, but has been proposed to occur when mechanical force to the nasal cartilage precipitates leakage or rupture of the mucoperichondrial vessels in the septum.
If the mucosa remains intact, extravasated blood strips the mucoperichondrium and/or mucoperiosteum from cartilage/bone as it accumulates within a closed space.
Where vessel compromise is coincident with fracture of the septal cartilage or bony components, blood may dissect through the fracture and form a hematoma.
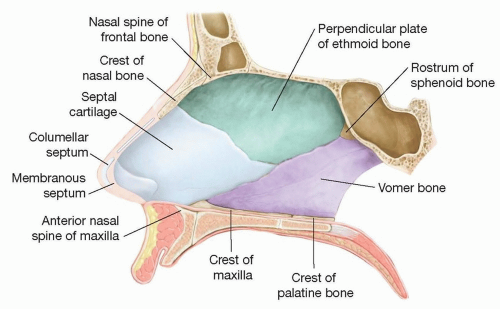 FIG 1 • The nasal septum is formed by cartilaginous, membranous, and bony components. |
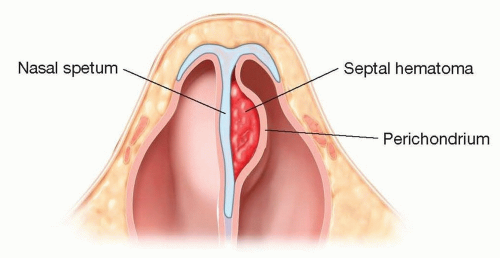 FIG 2 • A septal hematoma is formed when there is accumulation of blood into the potential space between the cartilaginous septum and the overlying mucoperichondrium. |
NATURAL HISTORY
When not promptly recognized, extravasated blood continues to expand between the perichondrium and cartilage. Eventually, the increased pressure causes collapse of the vessels supplying the septal cartilage. Pressure-induced ischemia, avascular necrosis, and liquefaction can result rapidly within 24 to 72 hours.
Where there is significant necrosis and destruction of the septal cartilage, the structural integrity of the septum is compromised, and a saddle nose deformity may be the end result.
Necrosed tissue may also act as a nidus for infection and abscess development. Bacteria isolated from septal abscesses are predominantly those species of the normal nasal flora, which include Staphylococcus aureus, Streptococcus pneumonia, group A β-hemolytic streptococcus, and Haemophilus influenzae.3 Collagenases produced by these bacteria serve to accelerate cartilage liquefaction.
Meningitis, cerebral abscess, subarachnoid empyema, and cavernous sinus thrombosis have also been reported as complications of septal hematomas.3
Because the development of septal hematoma may be delayed up to 48 to 72 hours from initial trauma,1 sequential evaluation is recommended.
PATIENT HISTORY AND PHYSICAL FINDINGS
Though relatively rare—occurring as a consequence to only 0.8% to 1.6% of nasal traumas1—one should be suspicious for septal hematoma when there is any history of craniofacial trauma.
A full head and neck examination should be performed to evaluate for any coincident injuries. In children, the possibility of abuse must be explored.
On history, progressive nasal obstruction is the most commonly reported symptom. Report of facial pain/headache, epistaxis, and fever are also common symptoms. Clinical features elucidated on physical examination that increase the pretest probability include hyperemia of the nasal mucosa, enlargement of the septum, swelling/ecchymoses of the nasal dorsum, external nasal deformity, and purulent rhinorrhea.1 Presence of any of these features should prompt further history about preceding nasal trauma, upper respiratory tract infections, or dental procedures.
With nasal septal hematoma on the differential diagnosis, focused intranasal examination of the nasal septum is required. Direct anterior rhinoscopy to evaluate the nasal septum may be performed with nasal specula. In addition to the septum, the inferior turbinate, a portion of the middle turbinate, and possibly the nasopharynx should be visualized. Both sides of the nasal septum must be evaluated.
The nasal mucosa is normally pink, without ulcerations, crusting, or bleeding. The septal hematoma is visualized as a lateral bulging (unilateral, or bilateral), with purple/dusky fluctuance. Palpation of the septum, by inserting a gloved finger into the nostril, may aid identification of a fluctuance. If such fullness persists even after topical administration of a vasoconstrictive agent such as oxymetazoline, the diagnosis of septal hematoma is highly likely.
IMAGING
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


