Abstract
The nails have several important functions, which become readily apparent when the nails are absent or lose their function. The most evident use of fingernails is adornment of the hand, but we must not underestimate other important functions of nails, such as the protective value of the nail plate against trauma to the underlying distal phalanx, the counter-pressure effect to the pulp which is important for walking and for tactile sensation, the fingernails’ scratching function, and the use of fingernails for manipulation of small objects.
The nails can also provide information about the person’s environmental exposures, emotional state, and overall health status. For example, a number of specific nail changes provide clues to the presence of systemic disease or genetic syndromes. In addition, changes in the nail are associated with a range of inflammatory skin diseases as well as tumors, both benign and malignant, that arise in the distal digit.
Keywords
nail, nail unit, nail matrix, onychodystrophy, longitudinal melanonychia, onychomycosis, Beau’s lines, onychomadesis, nail pitting, onychoschizia, trachyonychia, onychorrhexis, leukonychia, true leukonychia, apparent leukonychia, koilonychia, onycholysis, splinter hemorrhages, green nail syndrome, congenital malalignment of the great toenails, brachyonychia, racquet thumbs, nail–patella syndrome, pachyonychia congenita, acrodermatitis continua, parakeratosis pustulosa, nail lichen planus, clubbing, yellow nail syndrome, paronychia, capillaroscopy, onychotillomania, subungual hematoma, onchyogryphosis, pincer nails, ingrown toenails, onychocryptosis, subungual exostosis, onychomatricoma, onychopapilloma, longitudinal erythronychia
Anatomy
- ▪
Nail matrix → nail plate production
proximal matrix → dorsal nail plate
distal matrix (lunula) → ventral nail plate
- ▪
Proximal nail fold → nail matrix protection
- ▪
Nail bed and hyponychium → nail plate adhesion and distal detachment
- ▪
Nail growth rate: fingernails: 3 mm/month; toenails: 1 mm/month

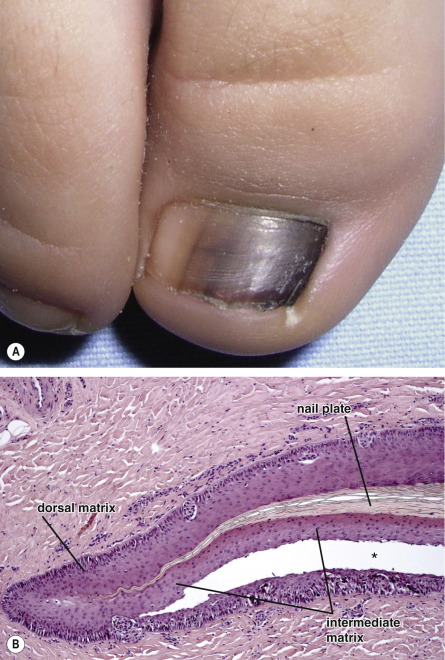
The nail matrix is responsible for the production of the nail plate and consists of an epithelium that keratinizes without the formation of a granular layer. Nail matrix keratinization occurs along an oblique axis, reflecting the upward and distal movement of cells during the process of maturation and differentiation . For this reason, the proximal portion of the nail matrix produces the dorsal portion of the nail plate, while the distal matrix is responsible for the production of the ventral nail plate (see Fig. 149.2 ). The distal portion of the nail matrix is visible through the transparent nail plate as a white, distally convex half moon known as the lunula. The matrix contains melanocytes that are normally quiescent; however, they may become activated and synthesize melanin, which is transferred to the surrounding keratinocytes. Distal migration of melanin-containing keratinocytes then gives rise to a hyperpigmented nail plate (melanonychia).
Nail plate production occurs continuously, proceeding from the 15th week of embryonic life until death. Under normal conditions, the mean growth rate of a fingernail is 3 mm/month and that of a toenail is 1 mm/month. Nail growth rate can be influenced by several factors, including age, systemic diseases, and medications.
Nail Signs
The clinical signs of various nail disorders depend upon the component of the nail apparatus that has been affected: nail plate alterations are due to matrix damage whereas nail plate detachment and/or uplifting arise from dysfunction of the hyponychium or nail bed ( Table 71.1 ). Paronychia represents inflammation of the nail fold, which can lead to secondary matrix damage. The nail plate can develop a wide range of structural changes, from thickening to fissuring to atrophy, in addition to discoloration ( Fig. 71.2 ).
| CORRELATION OF NAIL FINDINGS WITH ANATOMIC SITE OF NAIL DAMAGE | |
|---|---|
| Affected site | Clinical manifestation |
| Proximal matrix | Beau’s lines Pitting Longitudinal ridging Longitudinal fissuring Trachyonychia |
| Distal matrix | True leukonychia |
| Proximal + distal matrix | Onychomadesis Koilonychia Nail plate thinning Onychauxis (nail plate hypertrophy or thickening) |
| Nail bed | Onycholysis Subungual hyperkeratosis Apparent leukonychia Splinter hemorrhages |

Nail signs can be schematically divided into three major categories:
- •
signs due to abnormal nail matrix function
- •
signs due to nail bed disorders
- •
signs due to deposition of pigment within the nail plate.
Nail Signs Due to Abnormal Nail Matrix Function
Beau’s lines
- ▪
Transverse depressions that are more evident in the central portion of the nail plate
- ▪
Most often due to trauma
- ▪
Involvement of multiple digits suggests a systemic cause

Onychomadesis (nail shedding)
- ▪
Proximal detachment of the nail that is most often due to trauma
- ▪
Similar involvement of multiple digits suggests a systemic cause

Pitting
Pitting describes the presence of punctate depressions of the nail plate surface that can have an irregular outline (see Fig. 71.2 ). Pits are due to foci of abnormal keratinization of the proximal nail matrix which result in clusters of parakeratotic cells within the dorsal nail plate. In the proximal plate, these clusters appear as nontransparent collections of scale. Over time, shedding of the parakeratotic cells leads to the appearance of pits. These pits migrate distally with nail growth.
Diseases that produce nail pitting include psoriasis, alopecia areata, and eczema. Fig. 71.2 demonstrates how the patterns of the pits differ.
Onychorrhexis
Onychorrhexis is characterized by longitudinal ridging and fissuring of the nail plate (see Fig. 71.2 ). The depth of the ridges can vary as can the extent of involvement, i.e. a portion versus the entire nail plate. It is often associated with nail thinning, indicating damage to the nail matrix. Diseases commonly responsible for onychorrhexis include lichen planus, impaired vascular supply, trauma, and tumors that compress the nail matrix. The differential diagnosis includes the common phenomenon of age-related ridging of the nail plate.
Trachyonychia (twenty-nail dystrophy, sandpapered nails)
- ▪
Nail roughness
- ▪
Associated with thinning, koilonychia, and cuticular hyperkeratosis
- ▪
Conditions that may cause trachyonychia include alopecia areata (common), lichen planus (uncommon), psoriasis (rare), and eczema (very rare)

True leukonychia
- ▪
White opaque discoloration that is punctate, striate, or diffuse
- ▪
Punctate and striate leukonychia most often due to trauma to distal nail matrix
- ▪
Needs to be distinguished from apparent leukonychia (nail bed discoloration that is usually secondary to edema) and friable pseudoleukonychia due to superficial white onychomycosis
- •
Punctate leukonychia . The nail plate has small opaque white spots that move distally with nail growth and sometimes disappear before reaching the distal nail. It is caused by trauma and is most commonly observed in the fingernails of children.
- •
Striate leukonychia . The nail plate has one or more transverse, opaque white, parallel lines that migrate distally with nail growth. It is frequently observed in the fingernails of women, due to matrix trauma secondary to manicures. Striate leukonychia may also occur in great toenails as a consequence of trauma from shoes. It is also typical of Mees’ lines, the white transverse bands seen in arsenic and thallium poisoning .
- •
Diffuse leukonychia (porcelain nails, leukonychia totalis) . The nail plate is completely or almost completely opaque and white ( Fig. 71.6 ). Diffuse true leukonychia is rare and may result from mutations in PLCD1 (encodes phosphoinositide-specific phospholipase C delta 1 subunit, a key enzyme in phosphoinositide metabolism expressed in the nail matrix) or GJA1 (encodes connexin 43). Patients with GJA1 mutations also have keratoderma and hypotrichosis. Bart–Pumphrey syndrome, in which patients have deafness, knuckle pads and palmoplantar keratoderma in addition to leukonychia, is due to mutations in GJB2 (encodes connexin 26; see Ch. 58 ).

Fig. 71.6
True leukonychia – diffuse variant.
The nail plate is completely or almost completely opaque and white. It may be inherited due to mutations in PLCD1 , GJA1 (also keratoderma and hypotrichosis), or GJB2 (also deafness, keratoderma and knuckle pads); the latter two genes encode connexins 43 and 26, respectively.
Courtesy, Julie V Schaffer, MD.
Koilonychia (spoon nails)
The nail plate is thinned and flattened with upward eversion of its lateral and distal edges, leading to a concave spoon-like shape (see Fig. 71.2 ). Koilonychia, especially of the 2nd–4th toes in young children (1–4 years of age), is physiologic and eventually resolves spontaneously. In adults, koilonychia is rare and occurs in association with severe iron deficiency and systemic amyloidosis. It can also be seen in manual laborers who have contact with irritants and detergents that damage the nail plate.
Nail Signs Due to Nail Bed Disorders
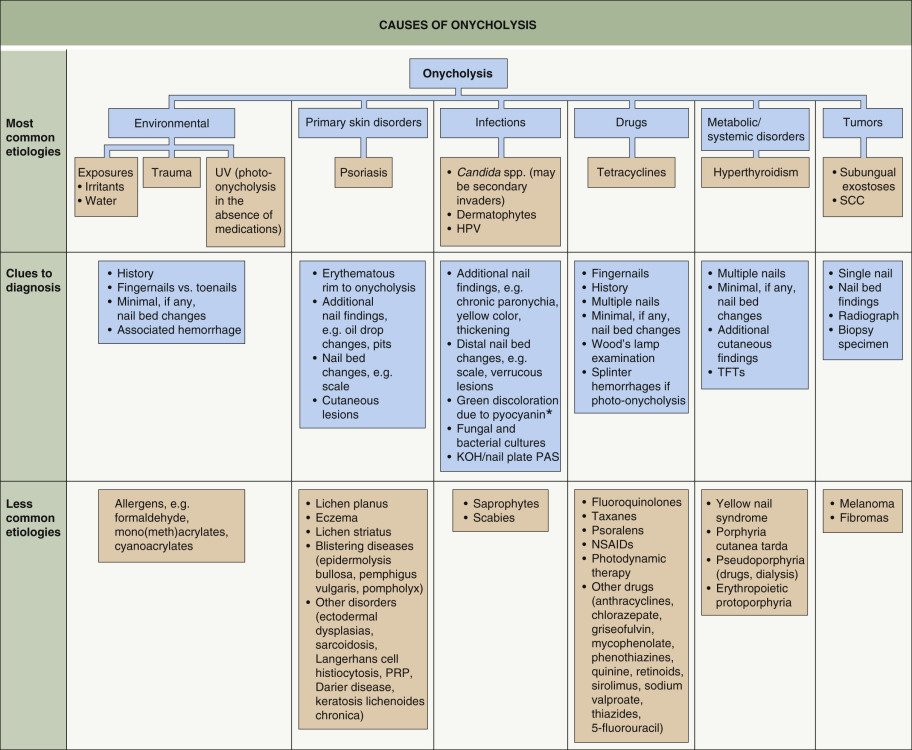
Onycholysis
The distal nail plate is detached from the nail bed and usually appears white because of the presence of air in the subungual space. If an exogenous pigment is present, the nail may appear yellow (fungi and exudate) to green–black (pyocyanin). In addition to environmental trauma, the nail bed disorders that most commonly produce onycholysis are psoriasis and onychomycosis ( Fig. 71.7 ). In drug-induced photo-onycholysis, there is usually involvement of several nails and subungual hemorrhages may also be present .
Subungual hyperkeratosis
The nail plate appears thickened due to an accumulation of subungual scales. Subungual hyperkeratosis results from excessive proliferation of the keratinocytes in the nail bed and hyponychium. It is commonly seen in inflammatory disorders such as psoriasis and contact dermatitis as well as in distal subungual onychomycosis.
Apparent leukonychia
- ▪
White discoloration that fades with pressure
- ▪
Nail plate transparency maintained
- ▪
Often due to drugs (chemotherapeutic agents) or systemic diseases (e.g. hypoalbuminemia)
Splinter hemorrhages
Splinter hemorrhages appear as one or more red–brown to purple–black, thin longitudinal lines in the distal portion of the nail (see Fig. 71.2 ). The shape of the subungual hemorrhages is due to the longitudinal orientation of nail bed capillaries. Dermoscopy allows better visualization of the hemorrhages which typically have a deep red to black color with peripheral fading.
The most common cause of splinter hemorrhages is trauma, followed by psoriasis, onychomycosis, and occasionally medications. Proximal splinters are rare and possible indicators of systemic diseases, including endocarditis (infectious and marantic), vasculitis (including septic vasculitis), trichinosis, and the antiphospholipid antibody syndrome.
Approximately 30% of patients with tuberous sclerosis complex have “red comets”, i.e. short red longitudinal streaks of the nail with an enlarged distal end . They are partially blanchable and are thought to represent telangiectasias plus extravasated blood.
Nail Signs Due to Deposition of Pigment
- ▪
Exogenous → convex proximal border
- ▪
Endogenous → concave proximal border (distally convex)
- ▪
Subungual deposition → nail bed discoloration with a transparent nail plate
Longitudinal melanonychia
- ▪
Longitudinal brown to black band
- ▪
Common in darkly pigmented individuals
- ▪
Single band may be a sign of melanocyte activation or proliferation (nevus, melanoma)
- ▪
Multiple bands point to physiologic, trauma/onychotillomania, drugs or systemic disease
| CAUSES OF LONGITUDINAL MELANONYCHIA | |
|---|---|
| Melanocyte activation | Racial Trauma
Drugs
Radiation Pregnancy Laugier–Hunziker syndrome Peutz–Jeghers syndrome Addison disease HIV infection Postinflammatory
|
| Non-melanocytic tumors | Bowen disease Onychopapilloma Onychomatricoma |
| Melanocyte hyperplasia/neoplasia | Nail matrix lentigo Nail matrix nevus Nail matrix melanoma |
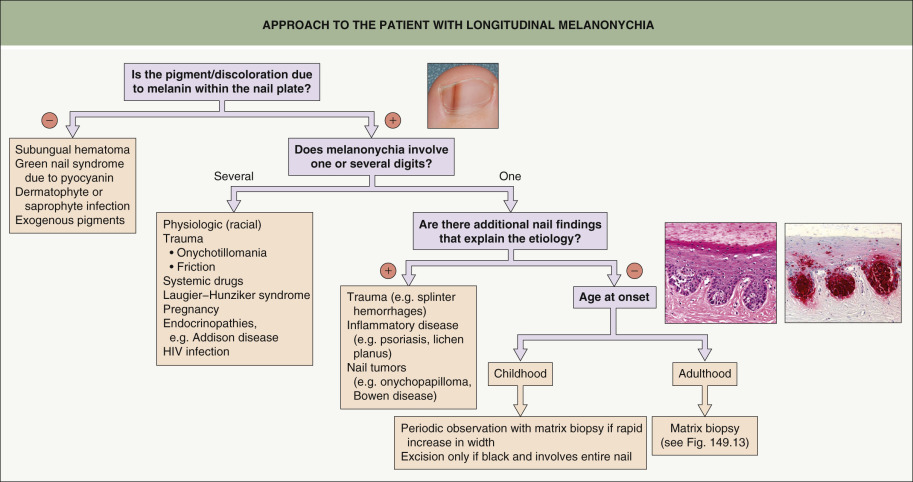
Dermoscopic criteria for benign and malignant nail melanocytic lesions have been proposed , but nail dermoscopy is not always feasible nor is it completely reliable in the evaluation of nail pigmentation . For example, it cannot be performed when the nail is totally black or very thick such that the lines and borders appear blurred. Additionally, dermoscopic evaluation may give false results, as irregular lines may sometimes be seen with benign pigmentation, especially following trauma. In one study, only intraoperative dermoscopy provided reliable clues to the diagnosis of nail melanoma . Histopathologic examination, when clinically warranted, remains the gold standard for the evaluation of nail pigmentation. A detailed description of biopsy procedures for longitudinal melanonychia is found in Chapter 149 .
Green nail syndrome
The yellow–green to green–black nail plate discoloration is due to the production of the pigments pyocyanin and pyoverdin by Pseudomonas aeruginosa (see Ch. 74 ). This discoloration is most often present in the subungual space created by onycholysis and less often in the lateral nail plate. Predisposing factors include prolonged exposure to water, use of detergents and soaps, nail trauma, and other causes of onycholysis or paronychia. Not surprisingly, this disorder is seen in barbers, dishwashers, bakers, and medical personnel.
Pseudomonas colonization can be eliminated from the nail surface by applying a few drops of 2% sodium hypochlorite solution (or household chlorine bleach diluted 1 : 4 in water) and from the subungual space by soaking the affected digits in the same solution for 5 minutes per day for 20–30 days. The underlying nail disorder must also be addressed, e.g. clipping back the detached nail plate if there is onycholysis.
Congenital and Hereditary Nail Diseases
The congenital and hereditary nail diseases include a number of conditions in which nail abnormalities may be present at birth or develop during infancy. A delayed onset can also occur as in Darier disease. In some patients, the nail abnormalities are key features for the diagnosis of genetic syndromes, e.g. congenital anonychia due to mutations in the gene that encodes R-spondin 4 ( RSPO4 ) or PLACK syndrome in which there is peeling skin, leukonychia, knuckle pads, and acral keratoses.
Congenital Malalignment of the Great Toenails
Congenital malalignment of the great toenails is possibly caused by an abnormality in the ligament that connects the matrix to the periosteum of the distal phalanx. The nail plate of the hallux is laterally deviated with respect to the longitudinal axis of the distal phalanx. This results in nail matrix damage with Beau’s lines and onychomadesis ( Fig. 71.10 ). The nail plate is often thickened and transversely overcurved. Congenital malalignment of the great toenails is frequently bilateral and is the most common cause of ingrown toenails in children and adolescents.

Congenital Hypertrophy of the Lateral Fold of the Hallux
Hypertrophic lateral nail folds are usually present at birth. There is an overgrowth of the soft tissue of the internal portion of the lateral nail fold, resulting in a hypertrophic lip that partially covers the nail plate. This abnormal growth may deviate the nail laterally and/or cause nail embedding with an acute inflammatory reaction and pain. The abnormality is usually bilateral and may regress spontaneously after a few years .
Racquet Thumbs (Brachyonychia)
Racquet thumb is a common congenital malformation due to shortening of the distal phalanx. It is usually inherited as an autosomal dominant trait. The nail is shortened and abnormally wide (see Fig. 71.2 ). Racquet nails are usually an isolated finding and radiologic examination demonstrates a short distal phalanx.
Nail–Patella Syndrome (Onycho-Osteodysplasia; Fong Disease)
Nail–patella syndrome is an autosomal dominantly inherited condition due to mutations in LMX1B , which encodes a transcription factor that regulates collagen synthesis. The condition most frequently involves the thumb and may also involve the other fingers but to a lesser extent ( Fig. 71.11 ). The nails are absent or hypoplastic, and the dystrophy is usually more marked on the radial side of the digit. A triangle-shaped lunula is commonly observed. The nail changes are typically associated with bony abnormalities, including absent or hypoplastic patellae, radial head dysplasia, and iliac crest exostoses (“horns”). In children, the diagnosis is best confirmed by the presence of iliac horns on pelvic X-ray.

Nephropathy develops in approximately 40% of patients. This leads to renal insufficiency in up to 8% of patients.
Epidermolysis Bullosa
Nail abnormalities are common in all forms of epidermolysis bullosa (EB), and nail involvement is one of the items scored to assess degree of severity of EB . Repeated, trauma-induced blistering produces onycholysis with shortening and thickening of the nail due to nail bed scarring. Involvement of the matrix can result in nail thinning and atrophy as well as pterygium. Dystrophic or absent nails with periungual granulation tissue are characteristic of junctional EB, generalized, and laryngo-onycho-cutaneous syndrome.
Ectodermal Dysplasias
Nail abnormalities are an important sign in many of the ectodermal dysplasia syndromes, where they are associated with hair, teeth, and/or eccrine gland abnormalities (see Ch. 63 ). Most frequently, the nails are short and thickened with onycholysis. All the fingernails and toenails are usually affected.
Pachyonychia Congenita
Patients with pachyonychia congenita (PC) are currently classified on the basis of the mutated keratin gene ( KRT ). PC-K6a, PC-K6b, PC-K16, and PC-K17 are due to dominant-negative mutations in KRT6a , KRT6b , KRT16 , and KRT17 , respectively. KRT6c mutations can lead to both isolated palmoplantar keratoderma and PC (see Ch. 58 ).
Nail abnormalities are frequently present and in general are more marked in PC-K6a and PC-K16. However, the number of nails affected can vary and in some patients with specific mutations in PC-K16, the fingernails may be spared. The characteristic finding is a thickened nail with an increased transverse curvature due to severe nail bed hyperkeratosis (see Figs. 71.2 & 58.11 ). Affected nails are extremely hard and difficult to trim. Associated findings include hyperhidrosis, oral leukokeratosis, follicular hyperkeratosis, hoarseness, and palmoplantar keratoderma, with pain on ambulation. Multiple pilosebaceous cysts are observed most frequently in PC-K17.
Darier Disease (Follicular Dyskeratosis)
- ▪
Red and white longitudinal streaks
- ▪
V-shaped indentation (notching) of the distal margin
- ▪
Giant cells in the nail bed epithelium

A single, red longitudinal band (longitudinal erythronychia) with distal subungual hyperkeratosis is not sufficient for diagnosing Darier disease of the nails, since single bands may be due to a subungual benign tumor (e.g. onychopapilloma, glomus tumor) and, less often, Bowen disease .
The Nail in Dermatologic Diseases
A number of skin diseases have associated nail abnormalities that often aid in establishing the proper diagnosis.
Psoriasis
- ▪
Several nails affected
- ▪
Diagnostic signs (fingernails only): irregular pitting, “oil drop” sign (salmon patch), onycholysis with an erythematous border
- ▪
In toenails, psoriasis is usually clinically indistinguishable from onychomycosis
- ▪
Often associated with psoriatic arthropathy
- ▪
The Koebner phenomenon worsens nail symptoms










