Myelomeningocele (MMC) is a congenital malformation of the spinal cord in the family of neural tube defects and spina bifida as described in the previous chapter (Myelomeningocele, Postnatal Closure).
Prenatal surgery was first attempted in the 1990s. A randomized controlled trial, the Management of Myelomeningocele Study (MOMS), demonstrated that closure during the prenatal period could be performed relatively safely and can result in significant benefit to the child.1
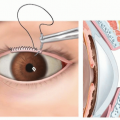
The MMC results from failure of neurulation resulting in an “open book” of distinct elements that are normally closed over the spinal cord (FIG 1) as described in the Myelomeningocele, Postnatal Closure chapter.
During neurulation, normally the neural tube undergoes an ordered process of formation and closure as described in the Myelomeningocele, Postnatal Closure chapter.
MMC leads to irreversible loss of nerve function at the level of the exposed spinal cord as described in the previous chapter (Myelomeningocele, Postnatal Closure).
In addition, a fetus with MMC will progressively develop two associated conditions as the result of the continued cerebrospinal fluid (CSF) leak, a Chiari malformation with hindbrain herniation and hydrocephalus.2
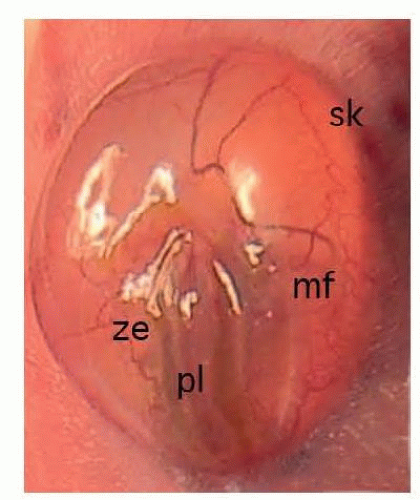 FIG 1 • Appearance of an exposed MMC defect during a fetal repair. The neural placode (pl) is seen at the center. This is surrounded by the zona epitheliosa (ze) and the skin (sk). The myofascial layer (mf) covered by dura can be seen through the translucent arachnoid. |
Expectant mothers receive extensive prenatal testing to determine if they are candidates for prenatal surgery. The inclusion and exclusion criteria in the MOMS trial are still used by most fetal therapy centers (Table 1).3
Ultrasound (US) examination is performed for three reasons: to define the MMC defect and its spinal level, look at associated CNS abnormalities, and evaluate the fetus for other structural abnormalities.
With regard to the MMC defect and CNS-associated conditions, US is used specifically:
To define the level of bone and skin opening
To analyze the posterior fossa, specifically to look for the presence of hindbrain herniation (must be present as it confirms an open neural tube defect)
To determine the size of the lateral ventricles and degree of ventriculomegaly
To look for any associated abnormalities such as a spinal cord syrinx, a split cord malformation, or a significant kyphosis that may affect the eligibility of the patient for fetal MMC repair.
Patients also receive a fetal magnetic resonance imaging (MRI) scan. These scans provide a more detailed anatomic evaluation of the MMC defect and associated abnormalities, particularly the presence of hindbrain herniation.
In addition to imaging, the fetus undergoes an analysis for genetic or chromosomal abnormalities. Also, amniotic fluid analysis is performed to confirm an open neural tube defect.
A detailed medical history for the mother is obtained, specifically looking for significant maternal health issues and risk factors associated with premature delivery.
The overall goal of the surgical repair is to obtain a multilayer closure that is watertight. To provide the greatest possible benefit to the fetus, the closure needs to protect the neural structures from direct trauma, prevent the leakage of CSF, and prevent the exposure of the neural structures to amniotic fluid. Additionally, the closure needs to be done in a manner that is safe for the fetus and the mother, as extreme premature birth can erase all potential gains of the surgical procedure. There are some modifications of the general technique outlined below, but the principles above should not be compromised.
A preoperative US is obtained to confirm the location of the fetus and the placenta.
Table 1 MOMS Trial Inclusion and Exclusion Criteria
Inclusion
Singleton pregnancy
Lesion level T1-S1
Evidence of hindbrain herniation
Gestational age of 19.0-25.9 weeks
Normal karyotype
U.S. residency
Maternal age of 18 years or older
Exclusion
Fetal anomaly unrelated to myelomeningocele
Severe kyphosis greater than or equal to 30 degrees
Multiple gestation
Previous spontaneous preterm birth less than 37 weeks
Short cervix less than 20 mm
Placental abruption or abnormal placentation (placenta previa)
Obesity defined as BMI > 35
Maternal medical condition that would place an additional risk to maternal health/surgical risk or the pregnancy (insulin-dependent diabetes, poorly controlled hypertension)
Documented history of incompetent cervix or planned/current cerclage
Maternal-fetal Rh isoimmunization, Kell sensitization, or a history of neonatal alloimmune thrombocytopenia
Maternal HIV, hepatitis B or hepatitis C positivity
Uterine anomaly such as multiple fibroids or müllerian duct abnormality; previous hysterotomy in the active segment of the uterus
Patient does not have a support person
Inability to comply with the travel and follow-up requirements
Patient does not meet other psychosocial criteria to handle the implications of the trial
Participation in another study that influences maternal and fetal morbidity and mortality or participation in this trial in a previous pregnancy
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree