| Epicanthus with moderate–severe telecanthus |
| Staged repair for blepharophimosis syndrome |
| Associated craniofacial syndromes (i.e., Treacher Collins and Crouzon syndromes) |
| Type and severity of epicanthal fold present |
| Degree of telecanthus |
| Other associated findings of blepharophimosis syndrome (ptosis, vertical skin deficiency, ectropion) |
| History of prior surgeries |
Introduction
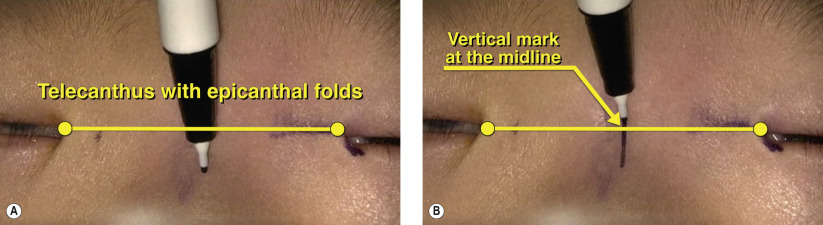
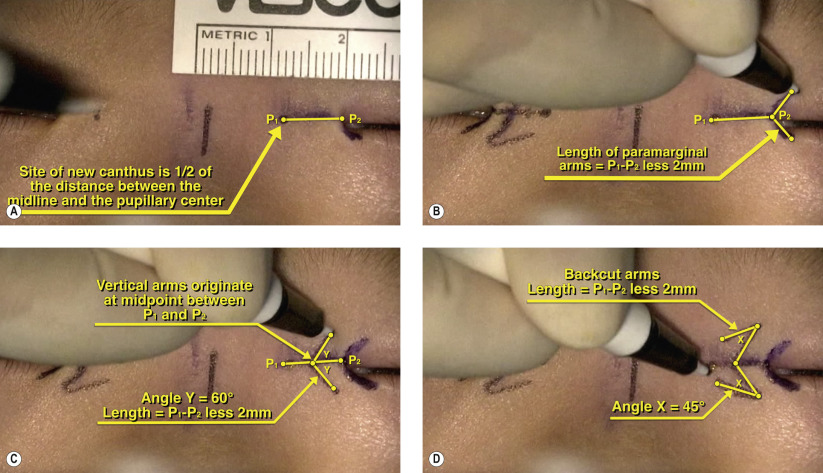
Mustardé’s technique of epicanthoplasty is indicated for the treatment of epicanthal inversus associated with moderate to severe telecanthus. Mustardé’s epicanthoplasty involves transposition of 4 Z-plasty flaps in conjunction with medial canthal tendon anchoring to the periosteum. In contrast, root Z-epicanthoplasty ( Chapter 7 ) addresses the epicanthus but does not alter the position of the medial canthi. Mustardé’s epicanthoplasty involves longer and more complex incisions and places the tissues under more tension, potentially resulting in higher scar-related complications necessitating a discussion with the patient and family.
Mustardé’s epicanthoplasty is often performed in the setting of blepharophimosis syndrome. The treatment of blepharophimosis syndrome is performed in a staged fashion and is best performed after the age of 2 years. The first step is correction of the epicanthus and telecanthus. If the telecanthus is severe, Mustardé’s soft-tissue fixation of the medial canthus alone may not be sufficient to reduce the telecanthus. In this case, placement of a midline transnasal wire is performed concurrently to powerfully reduce the intercanthal distance and allow for tension-free closure of the Z-plasty flaps. Ptosis correction is performed in the next stage and the type of operation depends on the degree of levator function. Typically, levator function is poor, which often necessitates frontalis suspension ( Chapter 15 ). The next stage is correction of any vertical skin shortage and lateral canthal surgery.
Surgical Technique

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


