Intractable recurrent epistaxis secondary to:
|
| History of coagulopathy |
| Anticoagulant medications |
| Nasal endoscopy |
| Vascular imaging of orbit, nose, and sinuses (magnetic resonance or catheter angiography) |
| Hematologic and systemic evaluation, including laboratory coagulation testing |
Introduction
Epistaxis is a very common and often self-limiting condition that the majority of the population has experienced in their lifetime. Even in young healthy patients without pre-existing medical conditions, recurrent epistaxis can occur. Recurrent and intractable epistaxis can occur with heritable coagulopathies, vascular malformations such as hereditary hemorrhagic telangiectasia (Osler–Weber–Rendu syndrome), neoplasms, and the result of naso-orbital trauma. While most treatment is aimed at packing and cautery of bleeding vessels, recalcitrant cases may necessitate adjunct procedures.
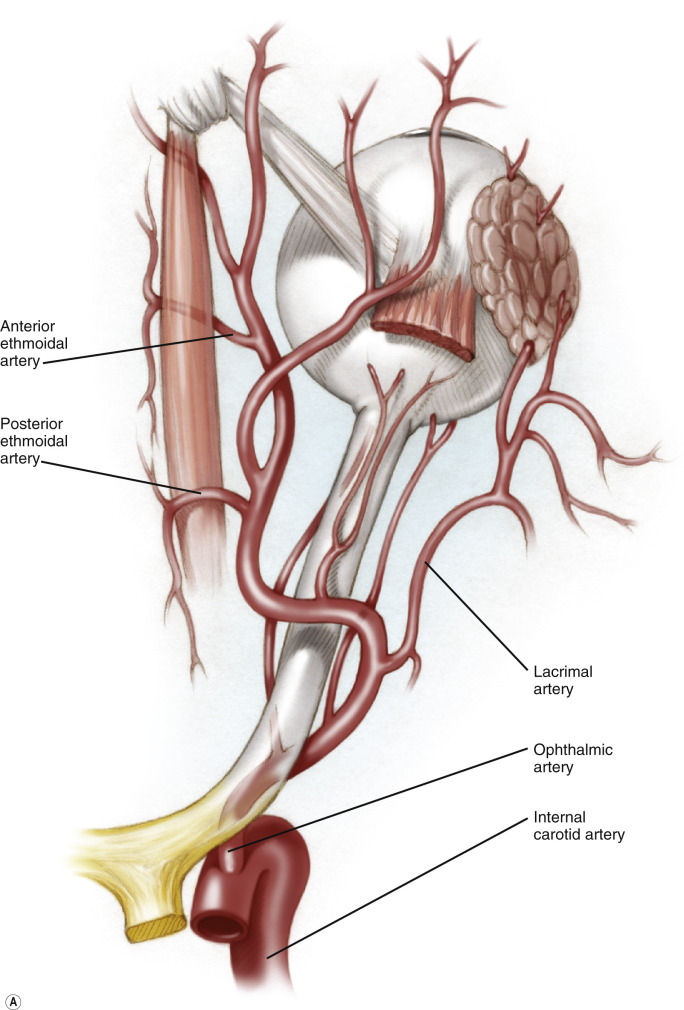
There is a rich vascular supply of the orbits, nose, and paranasal sinuses. Both internal and external carotid arteries supply this important area of the head and neck region. The anterior and posterior ethmoidal arteries arise as branches off the ophthalmic artery, which arises from the internal carotid artery ( Figure 69.1A ). They pass medially through the anterior and posterior ethmoidal foramina, to supply the lateral nasal wall and nasal septum ( Figure 69.1B ). The sphenopalatine artery, a branch of the external carotid artery, together with the anterior ethmoidal artery form Kiesselbach’s plexus, which perfuses the anteroinferior part of the nasal septum ( Figure 69.1B ). Over 90% of nosebleeds occur at Kiesselbach’s plexus.
In severe cases of recalcitrant nasal hemorrhage, particularly with hereditary hemorrhagic telangiectasia, ligation of the anterior and posterior ethmoidal arteries may be a useful adjunct to reduce the incidence and severity of epistaxis. Medial orbitotomy through a trancaruncular approach provides the best and most direct access to the ethmoidal vessels, which can then be clipped under direct visualization.