| Lower eyelid retraction without need for significant volume augmentation |
| Posterior lamellar and/or middle lamellar shortening |
| No history of adverse reaction to porcine xenografting |
| Contraindication or aversion to hard palate or autologous grafting |
| Quantify amount of eyelid retraction according to MRD2 |
| Manual palpation and elevation of lower eyelid to feel for restriction within the middle lamella; if supple elevation is possible, spacer graft may not be required |
| Assess adequacy of anterior lamella; may need cheek lift or skin graft if severe shortening |
| Assess eyelid laxity |
| Assess globe and inferior orbital rim position for presence of negative vector |
| Assess orbicularis strength; weakness on closure may portend high risk of recurrence |
| Prior eyelid, facial surgery or trauma |
Introduction
The use of acellular dermis as a spacer graft for lower eyelid retraction is similar to dermis fat ( Chapter 35 ) and autologous hard palate ( Chapter 36 ) with some distinguishing features. Dermis fat can restore lost orbital volume and provide a large surface area for posterior lamellar grafting with the benefit of being autologous, while hard palate supplies only surface area. Acellular dermis like hard palate provides posterior lamella but requires commercial preparation prior to use.
There are two sources of acellular dermis: the first is an allograft, taken from human cadaveric donors, and the second is a xenograft from porcine sources. Acellular dermis does not have a native epithelial layer but does provide a connective tissue framework for incorporation into host tissues. Conjunctival epithelialization, however, is required from the host.
Many decisions factor into the choice of posterior lamellar grafts. If patients are unwilling to have a second incision for an autologous graft, acellular dermis does provide a suitable option. Some potential downsides are prolonged inflammation and conjunctival injection during the epithelialization phase and the lack of volume that dermis fat provides. One benefit of acellular dermis and hard palate is no risk of ectopic hair transplantation that can be seen with dermis fat grafting. An additional benefit of acellular dermis over hard palate is the consistency of graft thickness and the virtually unlimited size compared to hard palate.
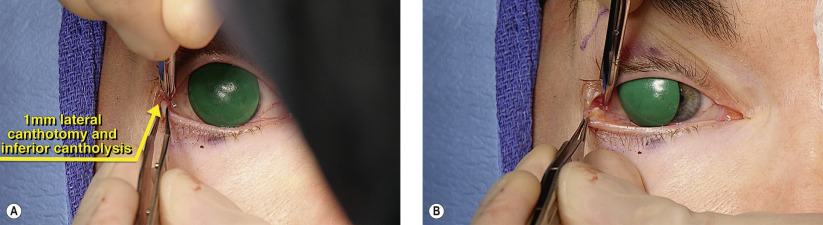
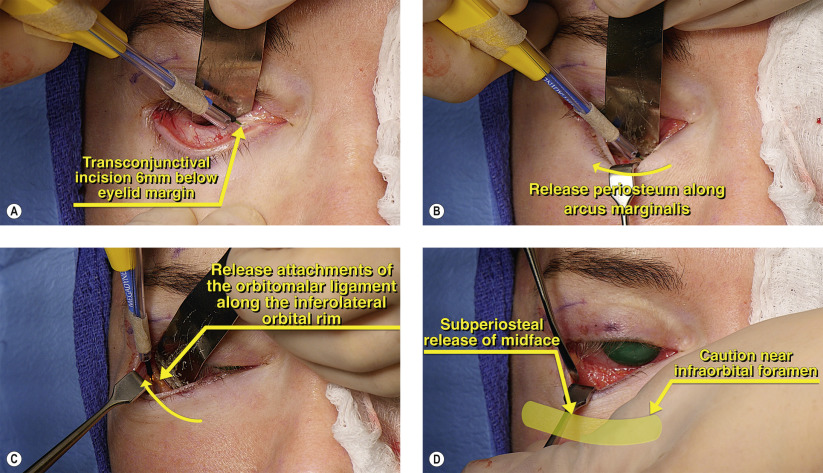
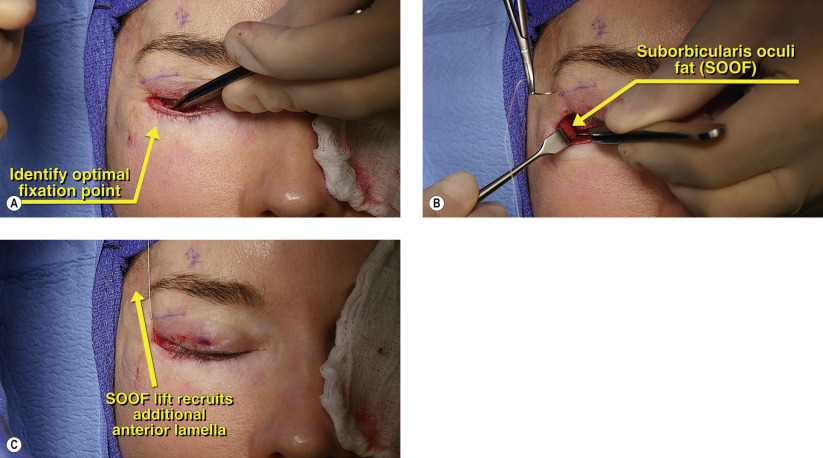
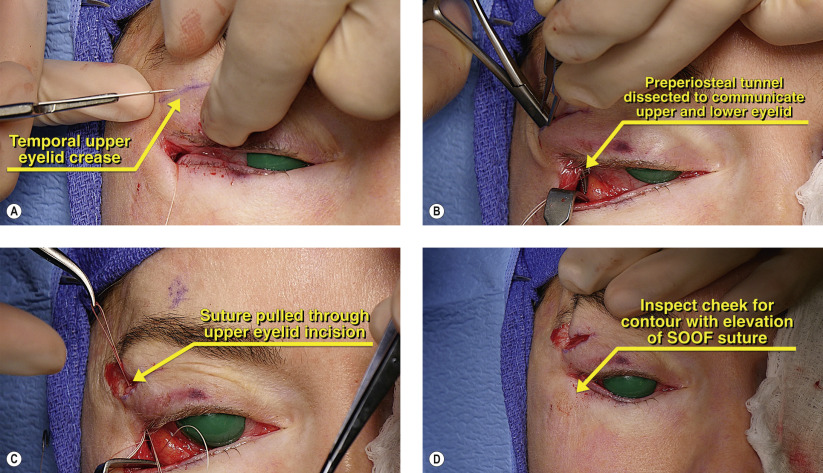
Conceptually, this chapter and the following two ( Chapters 35 and 36 ) are fundamentally similar. The surgery is performed through a transconjunctival approach. The lower eyelid cicatrix is released with an optional subperiosteal midface lift. Orbitomalar suspension can be performed to elevate the midface and to recruit additional anterior lamella. The spacer graft is secured posteriorly and the lower eyelid is tightened. The lower eyelid is then immobilized with Frost sutures.
For adequate surgical repair, slight oversizing of the graft is required as there will likely be some shrinkage postoperatively. Because the posterior lamellar graft can be irritating to the cornea, particularly if a Frost suture is placed, a collagen shield or a large-diameter contact lens can be used for comfort. Also helpful in reducing foreign body sensation are buried knots and fine, non-braided sutures to secure the graft.
Surgical Technique