| Eyelid closure from blepharospasm causing inability to perform activities of daily living |
| Recalcitrant blepharospasm not responsive to maximally tolerated medical therapy, including neurotoxins |
| History of prior neurotoxin use and dosage |
| Orbicularis strength |
| Assess for upper and lower eyelid malpositions |
| Assess for eyelid apraxia |
| Corneal sensation |
| Tear film quality and quantitative tear production |
| Prior eyelid, facial surgery or trauma |
Introduction
Essential blepharospasm is part of a spectrum of disorders referred to as cervicofacial dystonia, affecting approximately 1 in 10,000 individuals. The cause is unknown, but is likely a combination of genetic and environmental that leads to an increase of activity in the basal ganglia, which controls eyelid and facial movements. Neurotoxins provide the mainstay of therapy, although some oral agents have also been shown to be effective in some cases. The symptoms of blepharospasm are bilateral and abate during sleep as compared to hemifacial spasm which is typically unilateral with symptoms that persist at all times.
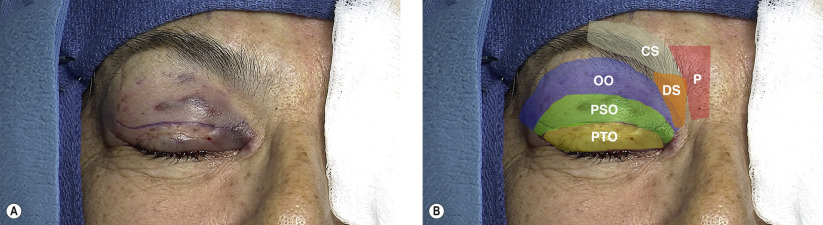
Blepharospasm consists of powerful contraction of the eyelid protractors. These muscles include the orbicularis oculi, corrugator supercilii, depressor supercilii, and procerus. Involuntary spasm of these muscles leads to closure of the eyelids, affecting vision and rendering patients unable to function.
Neurotoxins have revolutionized the treatment of blepharospasm and the vast majority of patients are able to resume normal activities with regular injections. Surgical intervention should be considered when maximally tolerated medical therapy with neurotoxins and oral agents are ineffective in reducing symptoms.
Protractor myectomy offers the opportunity to selectively weaken the muscles directly involved with involuntary forceful eyelid closure. While full myectomy was initially the procedure performed for blepharospasm, it has been associated with side effects, such as prolonged lymphedema, scarring, and lagophthalmos. Our preference is to consider limited upper eyelid protractor myectomy when indicated. Patients should be advised that neurotoxin use will likely continue to be needed after surgery, but will be more effective and that the main goal of the surgery is to improve their functional capacity.
Apraxia of eyelid opening is an associated phenomenon that prevents voluntary eyelid opening in the setting of blepharospasm. It may account for continued inability to open the eyes despite neurotoxin-induced protractor weakness. Limited protractor myectomy may improve symptoms related to apraxia of eyelid opening, but additional help is likely needed in the form of frontalis suspension to assist in eyelid opening ( Chapter 15 ).
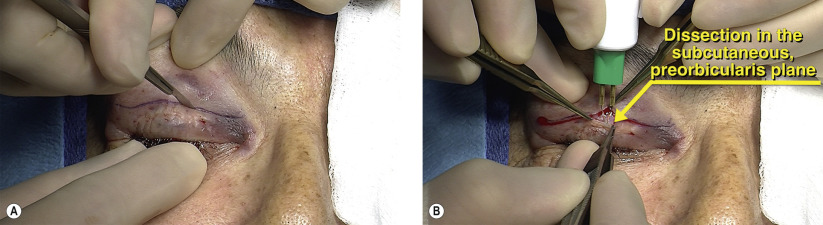
Surgical Technique