| Cosmetically displeasing lower eyelid fat prolapse without significant dermatochalasis |
| Functionally, when glasses rest upon prolapsed lower eyelid fat and causes lower eyelid ectropion |
| Prior facial surgery or trauma (including symblepharon) |
| Dry eye symptoms |
| Prior refractive surgery |
| Degree of dermatochalasis and fat prolapse |
| History of prior fillers to lower eyelid |
| Presence of midfacial ptosis |
| Presence of double convex deformity of lower eyelid |
| Presence of lower eyelid laxity or other eyelid malpositions |
Introduction
Transconjunctival lower blepharoplasty is well suited for patients with lower eyelid fat prolapse and minimal skin redundancy ( Figure 9.1 ). This approach is appealing to many patients as a skin incision is avoided and there is no orbicularis incision and potential for denervation. The drawbacks of this procedure compared to the transcutaneous approach ( Chapter 10 ) are the difficulty with a smaller incision, poorer exposure, potential for conjunctival chemosis and posterior lamellar shortening. Several adjunctive procedures can be performed with transconjunctival blepharoplasty including: skin pinch, chemical peel/laser resurfacing, lateral canthoplasty and fat redraping. With all of these adjuncts, the orbicularis is left intact, minimizing but not eliminating the risk of lower eyelid retraction and ectropion.
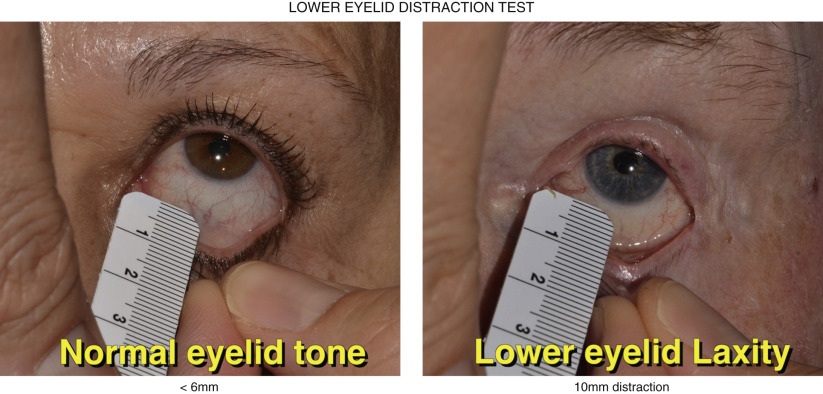
The preoperative evaluation should focus on ruling out co-exist eyelid malpositions such as ectropion, entropion, lower eyelid retraction and lagophthalmos which may predispose to dry eye. A lower eyelid distraction test is performed to assess laxity ( Figure 9.2 ). Normal eyelid tone is 6 mm or less and any laxity greater than 6 mm should be addressed with a lid tightening procedure such as a canthoplasty. Post-LASIK patients should wait at least 3 months after refractive surgery before considering lower blepharoplasty. The conjunctiva should be inspected for any signs of cicatricial changes. Minimal skin redundancy should be noted and if present, a decision to perform concurrent skin pinch or chemical or laser resurfacing should be considered at the time of surgery or postoperatively. Photographs in the frontal, profile, and side planes should be taken before and after surgery.
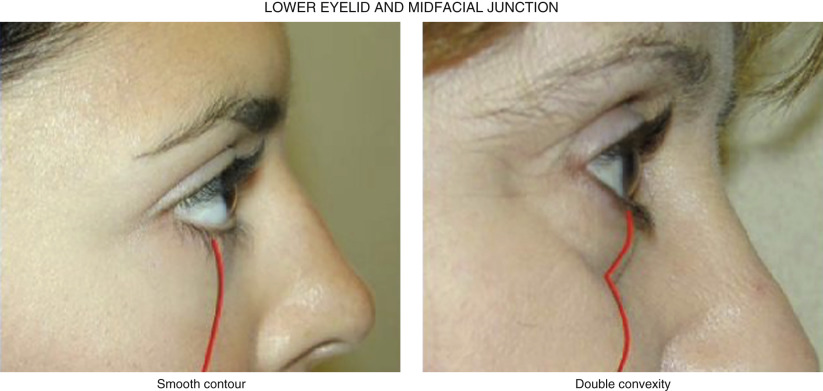
In youth, there is a smooth transition from the lower eyelid to the midface, but with aging, there is unmasking of the inferior orbital rim and generation of the double convex deformity ( Figure 9.3 ). Conservative blepharoplasty with fat redraping should be discussed with younger patients as aged-related fat atrophy may result in a sunken appearance with senescence if subtractive blepharoplasty is performed. Fat redraping can blunt the double convexity and restore a natural eyelid and midfacial transition.
Preoperative Evaluation
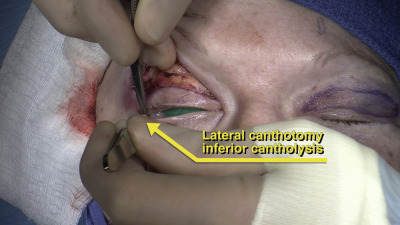
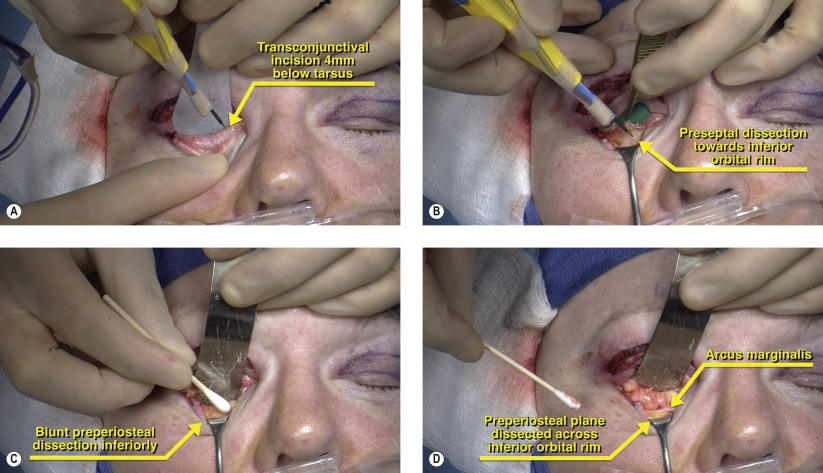
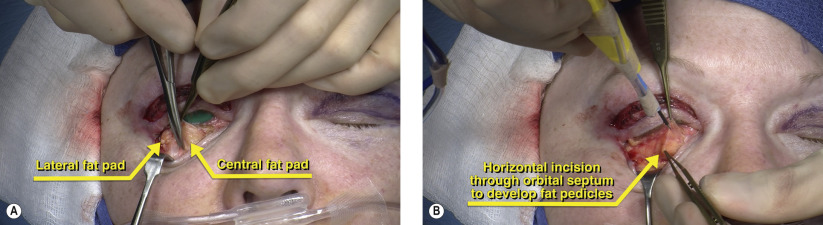
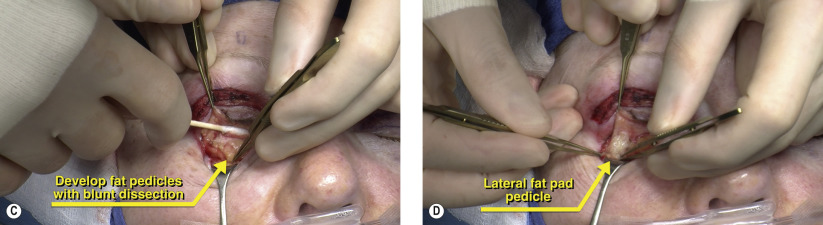
Surgical Technique