Multilevel Surgical Decision-Making for Ambulatory Cerebral Palsy
Benjamin J. Shore
Operative Indications
The majority of children with cerebral palsy who are referred to an orthopedic surgeon will already carry the diagnosis; however, a few children with hemiplegia or mild clinical manifestations will be diagnosed at the time of presentation to their orthopedic surgeon.
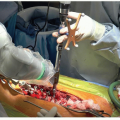
Historically, surgery for children with spastic diplegia used to start at the ankles with tendo-Achilles lengthenings (TALs) for equinus gait. This achieved a flat foot but at the expense of rapidly increasing hip and knee flexion.1 The second stage for surgery was then to lengthen the hamstrings in order to improve knee extension. This resulted in increased hip flexion and anterior pelvic tilt, so eventually the hip flexors were lengthened. Finally, transfer of the recuts femoris was considered for knee stiffness. This approach was caricatured by Mercer Rang as the “birthday syndrome.”2 As children spent most of their birthdays in hospitals, in casts, or in rehabilitation. Over the last 2 decades, single-event multilevel surgery (SEMLS) has become the method of choice for correcting lever arm dysfunction and multiple joint contractures in children with cerebral palsy.3 Typically, that will involve 2 teams of surgeons to facilitate simultaneous multilevel surgery (Figure 36.1).
The decision for SEMLS is often complex and multifactorial, as a result we have adopted the diagnostic matrix, previously described by Jon Davids.4 The diagnostic matrix consists of a standardized approach to clinical history, physical examination, radiology, gross motor function classification system (GMFCS) level, functional scales, and sagittal gait pattern identification. These components can be used in conjunction with either video or instrumented gait analysis (IGA). Once a detailed surgical recipe is developed, a postoperative rehabilitation plan is also scripted for the patient and family to obtain the
maximum functional outcome. It is important for the parent and child to appreciate the degree of time and effort associated with SEMLS rehabilitation. We typically describe a rehabilitation program that requires at least 1 year of intensive therapy and where improvements can continue to develop into the second and third year postoperatively.
maximum functional outcome. It is important for the parent and child to appreciate the degree of time and effort associated with SEMLS rehabilitation. We typically describe a rehabilitation program that requires at least 1 year of intensive therapy and where improvements can continue to develop into the second and third year postoperatively.
 Figure 36-1 ▪ For multilevel bilateral orthopedic surgery, the average number of individual procedures is close to 10; we therefore employ 2 surgeons and 2 residents/fellow to be able to work simultaneously. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
History
A solid understanding of the risk factors associated with development of cerebral palsy is critical for the orthopedic surgeon performing SEMLS surgery. Knowledge of typical motor milestones is helpful when assessing children with cerebral palsy; head control is achieved by 3 months, crawling by 6 months, pulling to stand by 9 months, and independent walking by 12 to 18 months.5 In addition to understanding milestones, the astute orthopedic surgeon will identify what a child’s current function is and their limitations and motivation behind improving gait and function. These questions are important to understand so that outcome and function can be closely aligned.
Physical Examination
A combination of elements defines a comprehensive physical examination including: observation of gait and posture, assessment of motor function (GMFCS and functional mobility scale [FMS]), assessment of muscle spasticity and presence of dystonia, evaluation for the presence of joint contractures, quantification of torsional abnormalities of the long bone including femoral neck anteversion and tibial rotation, selective motor assessment, and sensory examination.
Radiology
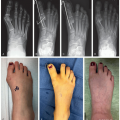
When considering SEMLS, it is important to assess for the presence of hip subluxation or acetabular dysplasia, pes valgus, scoliosis and torsional abnormalities. An anteroposterior view of the pelvis will identify hip pathology related to subluxation. A computed tomography (CT) scan, specifically a murphy protocol can identify torsional abnormalities of the femur (anteversion) and tibia (torsion). Standing scoliosis radiographs should be taken in those children where clinical examination demonstrates pelvis obliquity or concern for scoliosis. In addition, standing foot x-rays are important to demonstrate lever arm dysfunction and significant pes planus.
Sagittal Gait Patterns
Spastic hemiplegia has been classified into 4 patterns by Winters et al.6 These 4 patterns have been used as a template for the prescription of orthoses, spasticity management, and musculoskeletal surgery.
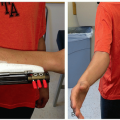
Type I hemiplegia: Characterized by drop foot in swing phase and loss of motor function to tibialis anterior without evidence of contracture. Management here can be with a hinged ankle foot orthosis (AFO) or posterior leaf spring AFO.
Type II hemiplegia: Spasticity of the gastrocsoleus complex and development of contracture are present. First and second rockers of the gait cycle have been disrupted, seen with excessive plantar flexion. Correction of the fixed contracture can be achieved with soft tissue lengthening at the gastrocsoleus complex (typically a Vulpius calf lengthening).
Type III hemiplegia: In addition to gastrocsoleus contracture, there is now cocontracture of the rectus and hamstring muscles. Spasticity management and consideration of lengthening of the medial hamstrings and rectus femoris transfer/lengthening.
Type IV hemiplegia: In this pattern, in addition to the gastrocsoleus and hamstring/rectus spasticity, there is now femoral anteversion, hip adduction, and flexion with the presence of acetabular dysplasia. This pattern typically requires femoral and acetabular surgery in addition to the surgical recipe outlined below.
Spastic diplegia has 4 sagittal gait patterns coined: true equinus, jump gait, apparent equinus, and crouch gait.7
True equinus: Characterized by overactivity of the plantar flexion knee extension couple, with the resultant ground reactive force lying anterior to the knee throughout stance phase. Often single-level surgery for the gastrocsoleus contracture is the incorrect strategy as there is often concomitant contractures of the hamstring and iliopsoas.
Jump gait: This gait pattern is characterized by spasticity of the hip flexors, hamstrings, and gastrocsoleus complex with incomplete hip and knee extension coupled with equinus at the ankle. This is the most common preadolescent pattern of spastic diplegia and these children typically benefit from SEMLS.
Apparent equinus: Many children may walk on their toes, but be wary of falling into the trap of assuming that ankle equinus is driving the observed incomplete heel strike seen with observational gait analysis (OGA). The savvy practitioner must examine the joint above and below the main deviation as often hip or knee flexion contractures may be responsible for the appearance of ankle equinus. The neuromuscular orthopedic surgeon must first recognize this gait pattern and then understand that calf lengthening here will worsen this gait pattern. IGA is helpful to differentiate true versus apparent equinus. Apparent equinus is often a transitional gait pattern from jump gait to crouch gait as lever arm dysfunction progress with growth and worsening spasticity. If you see a child who continues with an incomplete heel strike despite being in AFOs, consider apparent equinus.
Crouch gait: Crouch gait is described as increased hip and knee flexion and excessive ankle dorsiflexion in midstance. The soleus muscle is often overlengthening in this gait pattern and is commonly seen in adolescence. Overlengthening of the Achilles tendon can cause this gait pattern. Hamstring length can be assumed to be short due to this gait pattern but rarely is hamstring lengthening necessary, which will further exacerbate anterior pelvic tilt in this cohort of adolescents.
A series of surgical interventions can be included in the surgical recipe for SEMLS. The overarching theme is to preserve muscle length and strength and improve lever arm dysfunction and torsional abnormalities. It is important not to only focus on the physical deformities or anatomic abnormalities when considering SEMLS surgery. To be successful, one must consider the patient in the context of the World Health Organization—International Classification of Function,8 where we consider not only the body and structural abnormalities of the patient but how the child interacts and functions within their environment. Trying to align the goals of the surgeon and child/family are critical at the outset to have a successful surgical intervention. The goal in SEMLS is not only to improve the anatomic and structural deficits but also to improve the child’s function, mobility, and participation in their current environment. Spend time and identify what is important to your child and the family and make sure that the surgical goals or interventions that you are recommending are aligned with their goals and expectations. This is critical as the rehabilitation after SEMLS is long, challenging, and slow. It is important to outline that most ambulant children undergoing multilevel surgery will continue to see surgical gains 12 to 24 months after surgery. As a result, having an established therapy plan preoperatively is also important to ensure success of your surgical intervention.
Many of the soft tissue procedures utilized in SEMLS have been described elsewhere in the neuromuscular section; however, here we will describe iliopsoas lengthening over the brim, transfer of the semitendinosus around the adductor magnus tendon, and gastrocsoleus lengthening. Furthermore, bony correction for lever arm dysfunction has also been described elsewhere in the NM chapter, but we will outline some elements in the decision-making for isolated femoral and tibial derotation osteotomy.
Iliopsoas Lengthening Over the Brim
Operative Indication
In ambulant children (GMFCS I-III) with hip flexion contracture greater than 10°
Commonly seen in children with crouch or jump gait pattern
Look for the double-bump sagittal gait pattern on IGA
Alternate can be to achieve similar degree of correction via extension through the proximal femoral osteotomy
Equipment
Ragnell retractors or deep Langenbeck retractors to retract the psoas muscle medially
Peanut cotton elements are used to elevate the muscle fibers from the tendon of iliopsoas
Long-handled right-angle clamp
Positioning
Supine; if unilateral, can place a slight bump under the ipsilateral buttock
Avoid muscle paralysis so that you can identify if you are in close proximity to the femoral nerve
Make sure that you prep out the anterior superior iliac spine, pubic tubercle, and greater trochanter
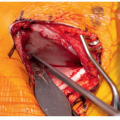
 Figure 36-2 ▪ A small 5-cm incision is centered over the anterior inferior iliac spine (AIIS). Place the incision 2/3 medial to the AIIS and 1/3 lateral in line with a hip flexion crease for cosmesis. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
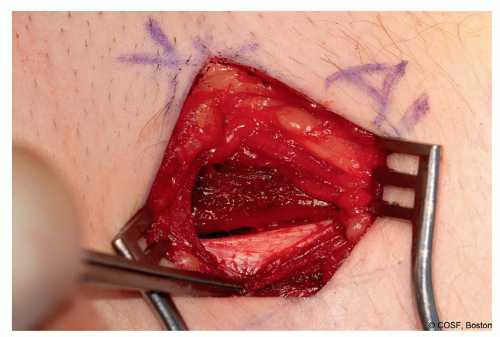 Figure 36-3 ▪ Identify the interval between sartorius and tensor fascia lata (TFL). Open the most medial aspect of TFL and avoid the lateral femoral cutaneous nerve as you dissect deep and just lateral to the direct head of rectus. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Surgical Approach
5-cm incision is centered obliquely over the anterior iliac inferior spine (Figure 36.2)
2/3 of the incision is medial to the AIIS and 1/3 is lateral
Open the skin and subcutaneous tissue
Palpate the interval between tensor fascia lata and sartorius
Open up the TFL just lateral to the interval (Figure 36.3)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree