Key points
• Celebrities’ values and beauty standards are a major influence on patients seeking aesthetic surgery.
• The explosion of social media and reality television has become an ever-increasing motivator for patients to consider aesthetic surgery.
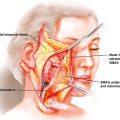
• The K-Pop export of the ideal V-shaped face, achieved often by quite invasive bony surgery and reduction of the angles of the mandible and the zygoma, has led to a rapid rise to these skeletal procedures.
• The impact from media can provoke unrealistic expectations in prospective patients, especially those who already have a low self-esteem and in adolescents.
• Studies have repeatedly shown that exposure to enhanced media images increases body image dissatisfaction which is believed to be the motivational catalyst to seeking aesthetic treatments.
Motivation for patients seeking aesthetic surgery of the face
The motivation for someone to seek out an aesthetic surgical or nonsurgical procedure on their face is complex and multifactorial. This chapter will examine the social value systems and the cultural, racial, and gender issues that contribute in various ways to the decision to seek out change, enhancement, or rejuvenation of the facial mosaic. Cultures differ from nation to nation and are formed by a long history of religious and moral boundaries, institutions, followed by government influence, and finally art, literature, and philosophies, all of which underscore the fact that motivations, for surgery differs from nation to nation and race to race.
History of aesthetic facial surgery
Modern aesthetic facial surgery was really born in the late nineteenth century and owes much to the ravages of syphilis and to the rebuilding of jaws and noses of soldiers surviving shrapnel facial injuries on the Western front in the trench warfare of World War I. From the experience gained from treating over 250,000 facially-injured soldiers, the founding fathers of plastic surgery emerged, including Harold Gillies, Jacques Joseph, Erich Lexer, and Hans Esser. The results of the efforts to reconstruct mangled faces were occasionally very rewarding to patients allowing them to reenter society. However, the majority of the facially-mutilated remained permanently disfigured either because they did not receive the reconstruction or the reconstructive efforts fell short of them being able to participate in gainful employment or meaningful social interaction. In reality most of the facially-mutilated became either charity cases or wards of the state or were employed in workplaces that did not expose them to the scrutiny of the wider population. Yet our specialty was born from these efforts to rehabilitate the facially-mutilated victims of conflict.
Nonsurgical aesthetic procedures such as paraffin injections to the nose and face existed before World War I, and there were fledgling aesthetic surgical practices especially in Germany by Jacques Joseph, Eric Lexer, and Eugene Von Hollander, who were performing facelifts and rhinoplasties.
The performance of aesthetic surgery at the turn of the twentieth century was not endorsed by the general surgical community, and the subspecialty of plastic surgery did not emerge from the control of general surgery until after World War 1. Aesthetic surgery was in the exclusive realm of the wealthy, the privileged, and the elite of Europe at that time.
One hundred years later the American Society of Plastic Surgeons in 2015 reported that there were 15.9 million surgical and nonsurgical aesthetic procedures performed in the United States representing a 115% increase since the year 2000. The enormous growth in the number of patients having aesthetic enhancement needs to be evaluated in the light of what has influenced the public to endorse aesthetic procedures so avidly. The patients themselves can be evaluated by the internal or psychologic state that brings them to seek aesthetic surgery and the external factors, such as the market place and medical environment, which offer the patient a better life through surgical and nonsurgical procedures. The psychologic issues related to aesthetic surgery are dealt with in this book by other authors. This chapter will deal with the nonpsychologic motivating factors.
Ethnocentricity (fitting in)
In large multicultural cities, where immigration expands the population and workforce the availability of rhinoplasty procedure deemphasizing an ethnic facial feature such as a prominent nose has been a strong motivator for immigrants to seek out surgery.
The stigmatization of “the Jewish nose” as a racial stereotype, a large curving nose hanging down like the number six, was a source of antisemitism characterizing a race rather than a religion, and this stigmata was carried by the immigrants into large urban centers such as New York City in the early twentieth century. In the era of antiimmigration in New York in the early twentieth century, Ashkenazi Jews fleeing from the ever-increasing antisemitism of Europe sought out removal of the prominent hump of their nose. European surgeons who acquired the techniques of rhinoplasty from Jacques Joseph included Gustave Aufricht and Jacques Maliniac, who performed thousands of rhinoplasties on Jewish immigrants. Rhinoplasty became the norm for the “Jewish nose,” and a “nose job” up until recent times was given to most Jewish girls by their parents if their parents could afford it.
Recently responding to the pressure of Purim, a Miami plastic surgeon offered free nose jobs to assist in the dating and marriage market. Melvin Kenner, an ex-anthropologist from Emory University, in his book The Jewish Body , says that the need for Jews to blend in was why “rhinoplasty was invented.”
More recently, middle European Jews are not really regarded as “new” immigrants to major American cities. However, wars in the Middle East have continued unabated, and this has caused a new surge of immigration since the 1970s whereby Western cities now have large populations of Lebanese, Syrians, Iranians, and Iraqis. These new immigrants are now highly motivated to fit into the WASP (White Anglo-Saxon Protestant) majority, and a rhinoplasty is considered a priority for young immigrants or the children of first generation immigrants.
Jewish identity has been reinforced by pride of Jewishness as is exemplified by the Jewish actress Barbara Streisand who stood alone in the 1970s, resisting the temptation of a rhinoplasty. Rhinoplasty is one of the most popular procedures globally, and within Turkey and Iran it is almost a rite of passage. The motivation for aesthetic rhinoplasty is strongly influenced by pressure from the family unit and is not discouraged by the Islamic faith. Saudi women are influenced to seek aesthetic surgery by the need to attract a husband or to prevent a husband from seeking another wife. Wearing a veil is not an impediment to seeking surgery.
Male surgery
The proportion of men seeking rhinoplasty has increased; men have always been consumers of aesthetic procedures especially hair transplantations and cosmetic dentistry. Their motivation for seeking surgery is more clearly related to identity, work, relationship, and life events. Holliday noted that the desire for aesthetic surgery in men was to be a “new man” to combat insecurity and “date younger women” enhancing their sexual self-identity. For men, aesthetic surgery has become commonsense rather than effeminate vanity.
The eurasian nose
The rapid growth of commerce in Asia and a burgeoning middle class in China, Korea, Japan, and Thailand has led to a population of mainly females seeking aesthetic facial procedures, particularly the procedure of dorsal nasal augmentation; deepening of the upper eyelid fold, called the “double eyelid operation”; and topical skin treatments to achieve a lighter skin tone. It is recognized by the mass media beauty model industry that the Eurasian features are highly desirable, both to Asian and Western aesthetic sensibilities. The Eurasian nose is more sought after in Western cities by immigrants who take permanent residence in large cities. What is sought after is different from what they might be able to attain in their own homeland. Choe et al. and Hodgkinson have noted respectively that Koreans in New York and Asians in Sydney are looking for enhancement with the Eurasian image in mind. The dorsum should be slightly higher and the supratarsal fold of the eyelid slightly deeper than might be sought by Asians in their cities or countries of origin.
Consumerism—the appetite for aesthetic surgery, beauty through consumption
In the last three decades, especially with the growth of print and digital media, there has been a normalization and sensationalization of aesthetic surgical procedures. Aesthetic surgery has become legitimized by advertising. The Hollywood and MTV star celebrity culture is thought to contribute to this normalization. However, this can provoke unrealistic expectations in prospective patients, especially those who already have a low self-esteem and in adolescents.
Davis studied the motives for aesthetic surgery and put it in the perspective of the general consumer society in which we now live.
“The desire to purchase and wear fashionable clothing (behavior, the assuaging of depression, low self-esteem and general body image dissatisfaction). The lessening of psychic pain (sensation, the ability to envision oneself in a new and different way). The restoration of a nostalgic past life in addition to evaluating risk and making rational and informed decisions about value of body enhancement (cognitive). The ability to relate better to family, friends, and business associations. The wish to be liked or admired more and the ability to be more competitive in areas of sports and making interpersonal relations. The feeling that prior products or procedures did not work or go far enough to achieve the desired effects (drugs). The desire to move toward the cultural ideal of beauty.”
Aesthetic surgery has become globalized just as the Internet and the airwaves have globalized information and online consumption. This has led to commoditization and a commercial orientation of medicine and the growth of medical tourism. By linking “cosmetic” to elective surgical processes there is a connection to particularly safe products, such as lipsticks and fragrances; this encourages patients to think of cosmetic surgery as less painful and with a brief recovery period.
Advertising and aesthetic surgery
In 1975, the American Medical Association (AMA) removed its restriction on advertising. Aestehtic surgery advertising grew out of the advertisements for cosmetic products, and this offered a huge population of potential customers who were dissatisfied with their appearance a chance for renewed youth, beauty, whiter skin, or enhanced sexuality. According to Hennink-Kaminski et al., in cosmetic surgery advertisements, there were four main approaches:
- 1.
Attractiveness
- 2.
Surgeon’s credentials
- 3.
Sexual enhancement
- 4.
Information
Sexual enhancement accounted for 25.2% of advertisement mostly suggesting increased sexual attractiveness.
At this time, plastic surgeons faced increasing competition from other subspecialty groups such as: otolaryngologists, ophthalmologists, “cosmetic surgeons,” and non–board-certified surgeons. This interspecialty competition fired up the advertising and media exposure aspirations of surgeons to compete for the lucrative aesthetic surgical patient, at the same time as insurance coverage became increasingly limited and the financial rewards for reconstructive surgery diminished. Advertising aesthetic surgery further exploits the youth and beauty centered culture in which we live despite statistics showing that the biggest population growth is in the aging population. This cultural emphasis suggests that without youth and beauty the person is less likely to get work opportunities and sexual partners. Advertising is increasingly aggressive, enticing, and widespread with statutory guidelines having low compliance rates. Advertising involves the narcissistic self-absorption of the insatiable consumer society in which we live, and aestehtic surgery indulges the impulse for consumer happiness.
Reality television
An extraordinary phenomenon of the early 2000s was the reality television show, streaming a variety of surgical procedures into Americans’ living rooms. Aestehtic surgery became entertainment, and the surgeons became stars. “Extreme Makeover,” “The Swan,” and “Botched,” among other reality TV shows, were then exported internationally to over 35 countries.
“Nip Tuck,” a popular drama involving professional actors as plastic surgeons, fantasized the profession and graphically over exaggerated the surgeons lives and surgical procedures for prospective patients. The show “90210” further extended this by focusing on the life of a young Beverley Hills plastic surgeon in his daily surgical practice and intimate home environment. This distorted portrayal was entertainment, but this did coincide with a huge upsurge in aesthetic surgical procedures, a 44% increase in 2004. Although unrealistic expectations by potential patients was a concern for the rank and file surgeon, they were benefitting vicariously from the actor–surgeon superstars.
Senior surgeons who shied away from the makeover show feared the nonpaying patient participant as a source of future angst and dissatisfaction but watched in awe as the media exposure blossomed as did the practices of the neophyte surgeons who participated in the shows. Indeed, the television exposure represented an endorsement for prospective patients of all genders.
Digital media mania
The power of mass media exposure in the living room creates a para-social interaction where the perennial viewer sees popular figures as part of their social world. This explains the persuasiveness of these characters and celebrity personalities. Specific facial features of actors and actresses are studied by prospective patients knowing that transformation is possible through surgical and nonsurgical techniques and technology. The “consumer” now referred to more so than the “patient” now carries with them a notion of how their lips, eyes, nose, cheek, neck might be transformed by the idealized digitally enhanced appearances of socialites, supermodels, and actresses. A particular interest in lips was generated by the exposure of the Kardashian/Jenner sisters, Kim, Khloe, Kourtney, Kendall, and Kylie. Kim Kardashian, Angelina Jolie, and Jennifer Lopez were poignant models for luscious lips, voluminous buttocks, and bulging breasts.
Younger people are more likely influenced by media’s fascination with the beautiful and the fact that their superheroes and celebrities such as Heidi Montag now openly endorse aestehtic surgery, which influences the younger age group’s (less than 21 years of age) views surrounding beauty. Unrealistic standards of beauty entice women to believe that they must work to attain true beauty.
The glossy social media presence of celebrities acts as a catalyst in young women to seek aestehtic enhancement; 82% of surveyed surgeons reported that celebrities were a major influence on patients seeking aesthetic surgery. The American Academy of Facial Plastic Surgeons in its publication “Facial Plastic Surgical Trends” noted that the “Kardashian Effect” and “Selfie Mania” were real and powerful effects on impressionable teens and younger adults. Nonsurgical procedures, such as Botox, peels, and enhancement injections to plump up the lips, were the first dip into the aesthetic surgery enhancement life journey for young people.
Surgeons have a vested interest in the endorsement of the celebrity aestehtic surgery outcomes, and this helps keep business buoyant. Persuasive videos are popular in advertising the benefits of surgery, and the message is pervasive, while rarely addressing the risks associated with surgery.
Our online image
The term ‘Zoom gloom’ has entered into the popular vernacular due to the reaction of the public and professionals who now during the COVID-19 pandemic are communicating with co-workers and colleagues in their own environment at home rather than in the office or clinic setting. The over explosion of our own face on a screen in a gallery on the Zoom meeting or face to face with Skype, FaceTime or Google Hangouts, confronts us, adding to the already stressful environment and we are faced with in the era of social distancing, isolation or lockdown.
Self perception is highlighted in real time without the means of alteration of our image either by Photoshop or filters as is commonly done for Facebook and social media platforms. The only ways of altering our self image is the positioning of light and our position within the focus of the camera. Compounding the difficulty of this communication is the reliance on Wi-Fi, internet reception, and issues of privacy.
Plastic surgeons have noted an upsurge in patients seeking to improve their on-screen personal face image. Many surgeons report an increase in injectables, including Botox and fillers, however more invasive procedures such as facelifts, eyelids and rhinoplasties are also frequently requested.
Video conferencing in businesses has been with us for about 25 years since the introduction of Webex. However Zoom, the most popular online platform, was launched in 2012 and has made the inventor, Eric Yuan, an overnight billionaire. Zoom is now used for family gatherings, happy hours, birthdays, and is a substitute for real contact family meetings, weddings and social events, as well as professional and business conferencing.
Heightened anxiety and depression as a noted consequence since the COVID-19 pandemic and exacerbated by the tsunami of statistics in media regarding cases, mortality and closures, coupled with the inability of human contact basic to the human condition, the lack of spontaneous smile or hug, understandably many in society are suffering a trial of confidence due to their imposed social isolation. This lack of confidence is mirrored when their appearance is challenged by their on-screen facial appearance.
Plastic surgery can offer a boost in confidence to correct long held anxieties about appearance issues and aging.
Patients’ retail habits have altered from mall shopping to online purchases through Amazon, eBay and many private major companies. For consumers of plastic surgery the consultation is also altered to a more virtual one due to recommendations by State health authorities to limit elective surgery and face to face consultations. Knowing that the pandemic is likely to be prolonged, prospective patients are planning for the future, bringing forward procedures they have been contemplating, not knowing what the future will bring but wishing to appear fresher, friendlier and younger whilst lockdown and isolation persists.
Zoom gloom is a new “Selfie Dissatisfaction,” a motivation for prospective patients to seek out aestehtic surgical consultations and procedures.
Plastic surgery before and after galleries
A potent source of images available to prospective patients is “before and after” images of surgical results posted by aestehtic surgeons and surgical societies on Internet sites and social media outlets. These may be accompanied by testimonials on review sites, giving star status to the surgeons involved. These images reinforce the benefits attained by aesthetic surgery especially in the realm of improved self-esteem. Marketing companies employed by many surgeons to promote their practice stress the importance of not only before and after pictures but also videos and testimonials.
In some countries, such as Australia, even though testimonials are in fact banned there is very little reason for surgeons not to continue posting them because there is no real way of enforcing the ban. Review sites are a substitute for testimonials. Google ratings, RealSelf ratings, and the clinic’s Internet presence through physician advertising and search engine optimization (SEO) companies aim to propel the image of the surgeon into the digital realm of the inquisitive prospective patient. The web images, when assessed critically, are usually of the more spectacular result, using the most flattering angles of the images while often overexposing the after photo whereas the before photo is underexposed or of normal exposure. Aestehtic surgical magazines and journals expose the reader to only the best results in advertorials. The concern about false and deceptive advertising in aestehtic surgery has been ever-present even before the advent of social media. Twenty-five percent of Yellow Pages advertisements in 2002 by aestehtic surgeons were considered to be appealing to the fears, anxieties and emotional vulnerability of the general public whilst 18% were considered objectionable.
Financial incentives
With medical credit cards, surgeon financing, doctor payment plans, layaway plans, and bank loans, aestehtic surgery is seemingly becoming affordable to everybody, but it may require overseas travel to fit into one’s budget. Aesthetic surgery is seen by consumers as preferable to some luxury items and a good place for disposable income to be invested. The older age group seeking facelift and body contouring procedures after completing their childbearing responsibilities are likely to have excessive disposable income compared with the younger group seeking rhinoplasty and breast augmentation procedures. With bank interest rates at all-time lows, personal loans that are typically paid off in 1 to 5 years are a popular source of capital for lower budget procedures, such as breast augmentation and rhinoplasty. The return on investment is the improved self-image and perhaps improvement of quality of life. Daniel Hamermesh, an economist from the University of Texas, Austin, estimates the return on investment to be 15%. The middle-aged, the out of work, or the retrenched regard aesthetic surgery as an opportunity to perhaps reenter the workplace, and so facelift or rhinoplasty, especially in males, is sought by this group. When affordability becomes a factor, then motivation outweighs the potential risks of traveling to an emerging country for aestehtic surgery and the prospective patient enters a new area of risk, not knowing the standards of the facilities or surgeons to whom they are entrusting their health and appearance.
The medical tourism industry
The supply-and-demand gap in health care provision has fueled rising costs of medicine in the developed world and has resulted in a great opportunity for emerging countries such as Mexico, Thailand, Philippines, Turkey, Poland, Hungary, and Dubai for medical tourism, which is now a $60 billion international business. It is estimated that 1.6 million patients will leave the United States a year for medical procedures performed elsewhere. The cost factor is a major driver of aestehtic surgical tourism, and affordability is the major motivator for the prospective patient.
Unfortunately, the after care of the medical tourist is often left to surgeons in the country from which they departed, and if complications occur postoperatively this burdens the local medical fraternity. They feel “jilted” by patients who have come from overseas and other surgeons, carrying with them problems that are difficult to resolve often with inadequate medical history records, implants that they are not sure what has been inserted, and infections with antibiotic-resistant bacteria.
An ethical issue also arises when an emergent country with insufficient medical resources for their own citizens starts to treat wealthy overseas patients in preference to their own citizens who require medical assistance. In medical tourism, a group mentality (posse-type mentality) exists for young women traveling with supportive friends having a holiday and surgery together, and this peer pressure supports perhaps less well researched aestehtic surgery. Meredith Jones explained that because aesthetic surgery relates to ideas of self-love, body maintenance, and psychologic well-being it easily is coupled with the indulgence of holidays. Visiting Thailand for a luxury spa holiday and a facelift seems perfectly logical as is visiting South Africa for liposuction and a safari. Domestic surgeons whose practices are in popular tourist locations promote their services in a very similar manner as to have patients come to a fun place with beach and cafe subcultures and enjoy the tourist destination while having aestehtic surgery
The globalization of aesthetic surgery
The United States certainly is the capital of aesthetic surgery, however, with the explosion of aesthetic surgery within the United States the power of their media has led also to globalization and acceptance of aesthetic surgery throughout the world, particularly most recently in emerging Asian countries. Japan, Korea, and most recently China all have come into the spotlight. Sociologists see aesthetic surgery as playing a significant role in identity “construction” and the pressure to constantly modify oneself in the current surgical and make over society. ,
Wealthier patients from the former Soviet Bloc countries or the Middle East travel to large European cites or to Dubai where high-end plastic surgery flourishes. The unavailability of a service or procedure or the distrust in the medical system in their own countries is a motivator to seek services in another country. So, a fashion shopping trip may be combined with a rhinoplasty for their son or daughter or a blepharoplasty for a patient with aging eyelids. A number of centers in Asia are plastic surgery hubs, including Seoul and Singapore. In South America, Buenos Aires, Rio De Janeiro, and Mexico City are also hubs for patients traveling from adjacent emerging local economies.
Japan
In Japan, since 2000, exposure to aestehtic surgery has been profuse in the media, magazines, and television shows. “Seikei Bijin” (Plastic Surgery Beauty) was a popular television series featuring a Japanese actress, Yonekur Raoko, who was born into a family with ugly ancestors. She transforms her life into a celebrated model after undergoing an extreme makeover. The final happy conclusion is that her marriage to a Japanese ikebana master. This “Cinderella transformation” was a highly popular series strongly endorsed by working middle-class Japanese women.
Skin whitening has been an aestehtic procedure engrained in the Japanese culture for hundreds of years. It is associated with aristocratic aspirations, not an attempt to emulate Western ideals.
Korea—plastic surgery capital of the world
Aesthetic surgery in South Korea has been a subject of much conjecture because it appears to be intertwined with the Korean pop culture and the musical phenomenon of K-Pop. The artists are usually young pubescent androgynous boys with a specific hairstyle and fashion sense appealing to a younger audience, and many of these stars reach idol status.
South Korea has been labeled the beauty capital of the world as an ever-increasing percentage of the population endorses the K-Pop ideal and proceeds to emulate the facial appearances of their idols.
In one district alone in Seoul (Gangnam), there are 300 aesthetic surgical clinics in the one small defined urban area, all with very provocative names, including “Cinderella,” “Beauty Line,” “Face Plus,” and “Small Face,” emphasizing facial contouring procedures, such as chin, jaw, and cheek areas. The underlying notion that physical features are an indicator of social class and disposition is ingrained in the Korean psyche. In light of this, pale skin is also an important female beauty standard in Korea. K-Pop stars endorse skin lightening and aestehtic surgery, which they have endured. The obtaining of beauty enhancement by surgery is seen as a weapon to win school admission, job applications, promotions, and romantic success.
The K-Pop export of the ideal V-shaped face, achieved often by quite invasive bony surgery and reduction of the angles of the mandible and the zygoma, has resulted in skyrocketing medical tourism to the Gangnam district. The downside of the standardization of appearance to the idol “module” is at a decrease in individual identity. This conformity is not as well accepted in the West, where individualism and customization of the existing features and the desire for a more natural-looking result is the usual surgical objective. This conformity leads to uniformity.
“In the quest for what is desirable and enviable, people find themselves locked in the oblivion of sameness.”
Even though the Korean Association of Plastic Surgeons has voiced concerns over the consumerism of aesthetic surgery by advertising, they are benefitting from it, and their protests do nothing to stem the tide of Korean patients and overseas patients chasing the K-Pop beauty idea.
Buying beauty in china
The booming economy of China has resulted in a frenzied consumer consumption mentality, and the aestehtic and plastic surgery industry is experiencing parallel dramatic increase in demand for their services.
Coupled with a patriarchal society women have an opportunity to transform themselves into the physical objects that they perceive the opposite sex will find desirable. A highly eroticized milieu now exists in China. Wen Hua noted that in the “one child policy” era, female Chinese infants invariably grew up playing with the Barbie doll, a symbol of hedonistic consumer culture and an ideal of Westernized female beauty. One such icon most recently reported is Ivanka Trump.
Market research of aesthetic surgery revealed that 50,000 aesthetic surgical procedures were carried out at the public Ninth Hospital in Shanghai in 2012. The most common procedures are rhinoplasty, blepharoplasty, and liposuction.
China is also home to a unique voyeuristic television series called “Miss Plastic Surgery,” where contestants can only compete if they have undergone plastic surgery.
The unbridled growth of the aesthetic surgery industry in China is now valued at $62.6 billion, and as China continues to grow and the middle-class ages, rejuvenation surgery will also grow, particularly facelift and nonsurgical techniques of facial tightening. The social media craze in China has also paved the way for an estimated $122 billion industry by 2019.
Gender issues
The liberation of social attitudes to gender dysphoria over the last 25 years has resulted in centers of excellence carrying out “sex change” operations. Social media and the powerful word of mouth advertising of satisfied sex reassignment patients has resulted in a steady growth of clinics specializing in gender reassignment.
Female-to-male surgery patients rarely undergo any facial aesthetic surgery; however, male-to-female surgery patients typically undergo a variety of surgical procedures, including bone contouring of the forehead, rhinoplasty, hair grafting, and reduction of the prominence of the thyroid cartilage. The images of such dramatic transformations are powerful visual stimuli for those aspiring to transform themselves. These patients seek out a surgeon or clinic that they hope can achieve the results that they see on various websites and social media outlets.
Feminist literature toward aesthetic surgery is polarized between personal choice and women being victims of a male-dominated beauty system.
Summary
Patient motivation to undergo a surgical or nonsurgical facial procedure is multifactorial and complex. Subconscious, religious, cultural, ethnic, and social factors interplay in various ways in all patients. For the surgeon, only a glimpse of what has motivated the patient might be obtained by an interviewing style consultation. Surgeons will likely not know all of the motivating factors influencing the patient in the vast majority of cases.
Most patients, we can surmise, are not clear on their own motivational factors and hence cannot transmit them either to themselves or to others. Aesthetic values are perpetrated by the media and are in a rapid ongoing flux with the new and ever-increasing tsunami of still and video digital imaging they are exposed to. The explosion of social media and reality television has become an ever-increasing motivator for patients to consider aesthetic surgery. This trend seems to be worldwide and has specific effects in prospective patients from different countries and racial groups.
Appreciating that value systems are different in different ethnic subgroups and differ from nation to nation and being aware of the media’s influence are paramount. Ignorance of these differences, often combined with communicating with patients who speak different native languages, can result in a situation fraught with the potential for miscommunication. This is an unideal situation for the surgeon who intends to operate on the most aesthetically sensitive area of the human body—the human face.
Surgeons need to show understanding of the myriad of different influences that the patient brings to them in their consultation. Through understanding the patient’s motivations for surgery, as much as possible, the surgeon is more likely to avoid a dissatisfied postoperative patient.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


