Monobloc Distraction
Peter J. Taub
Vincent A. Chavanon
DEFINITION
Craniofacial dysostosis syndromes result in disproportions of the skull and facial bones leading to reduced intracranial volume, midface retrusion, exorbitism, airway obstruction, and malocclusion.1,2
The midface hypoplasia associated with these syndromes may lead to corneal exposure that threatens vision, sleep apnea, and malocclusion, as well as deformities.
ANATOMY
A combination of cranial vault and facial growth disturbances exists among multiple craniofacial syndromes.
Monobloc advancement separates the anterior portions of the skull base, orbits, maxilla, and dental arch, which remain in continuity and are moved anteriorly.
The scalp is composed of five layers: the skin, subcutaneous tissue, galea aponeurotica, loose areolar subgaleal tissue, and pericranium.
Dissection may proceed at different levels in different approaches.
The temporal branch of the facial nerve (cranial nerve VII) lies immediately above the superficial layer of the deep temporal fascia and must be preserved when elevating the soft tissues of the forehead to avoid injury.
The anterior ethmoidal artery exits the medial orbital wall approximately 24 mm deep to the orbital rim, and the medial wall osteotomy should be planned anterior to this landmark.
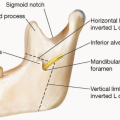
The bones of the cranium and the facial skeleton articulate at the frontal bandeau, the floor of the anterior cranial fossa anterior to the cribriform plate, the lateral orbital wall (greater wing of the sphenoid), the zygomatic arch, the medial orbital wall (ethmoid complex), the nasal septum, the orbital floor, and the pterygomaxillary fissure.1
The palpebral complex is anchored by the medial and lateral canthal tendons, which insert onto the posterior lacrimal crest and Whitnall tubercle, deep to the orbital septum.
PATHOGENESIS
A number of genetic, molecular, cellular signaling pathways, as well as mechanical forces, interact to produce the craniofacial dysostosis syndromes.
Patients with the same genotypes may have a broad variety of penetrance, influencing the level and severity of expression of the syndrome in individual patients.
Different mutations in the fibroblast growth factor receptor-2 (FGFR-2) gene may lead to either Crouzon or Apert syndrome, which both display autosomal dominant inheritance.
The restricted skull base growth in these syndromes leads to brachyturricephaly and elevated intracranial pressure (ICP). Facial hypoplasia results in orbital retrusion and narrowing of the nasopharynx and Angle class III malocclusion.3
NATURAL HISTORY
Cranial vault restriction may lead to elevated ICP, which has negative consequences on long-term cognitive, psychological, and functional outcomes.
Chronic sleep apnea has an additional deleterious effect on psychosocial outcomes.3
Reduced orbital volume may cause exorbitism, which may lead to corneal exposure and loss of vision.1
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough evaluation of the patient’s cognitive, psychological, functional, and aesthetic status is required.
Evaluation by a multidisciplinary team permits a 360-degree assessment of the patient and improves preoperative planning. The team comprises plastic surgeons, neurosurgeons, ophthalmologists, otolaryngologists, oral surgeons, pediatricians, geneticists, psychologists, speech-language pathologists, orthodontists, and pediatric dentists.
The neurosurgical member of the team helps to identify Chiari malformations and is needed for exposure of the anterior cranial vault.
An ophthalmologic exam identifies papilledema secondary to elevated ICP, increasing the urgency for surgery.
A neuropsychological exam identifies baseline functional deficits that may improve with early surgical intervention.
Genetics evaluation confirms the diagnosis, uncovers other potential medical problems in the child, and identifies risks for future family planning.
IMAGING
True or reformatted lateral cephalograms may assist with advancement planning.
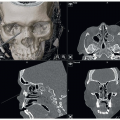
Computed tomography (CT) with three-dimensional reformatting may show evidence of suture fusion, hydrocephalus, and signs of ICP elevation (copper-beaten skull).
Magnetic resonance imaging is not usually necessary unless a brain abnormality requires evaluation.
NONOPERATIVE MANAGEMENT
Continuous positive airway pressure (CPAP) or supplemental oxygen can be used for mild obstruction or tracheostomy for severe airway obstruction.
Patching, moisturizing eye drops, and tarsorrhaphy are useful to protect the cornea against orbital exposure.1
The benefit from tarsorrhaphy may be self-limited and ultimately ineffective due to tissue stretch and dehiscence.
Herniation of the globe after tarsorrhaphy may impede reduction of the globe resulting in loss of vision.1
SURGICAL MANAGEMENT
Indications for monobloc distraction:
Exorbitism with corneal exposure or visual loss
Upper airway obstruction
Malocclusion
Midface retrusion
Patients with facial retrusion and a brow or infraorbital rim to cornea relationship of 5 mm (FIG 1) or 5 mm of negative overjet in occlusal relationship are optimal candidates for advancement.2Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree