All patients with postparalytic facial paralysis are at risk of developing synkinesis due to aberrant nerve regeneration. Synkinesis can result in smile dysfunction, tension, and eyelid aperture narrowing due to overactive and uncoordinated muscle activity. When the synkinesis causes an asymmetric smile, there are several treatment modalities including neurotoxin, neuromuscular retraining, and surgery. Modified selective neurectomy of the facial nerve is a treatment option that potentially can improve the smile mechanism by reducing the activity of counterproductive facial muscles while preserving the natural neural pathway.
Key points
- •
There are several techniques and approaches to treat facial synkinesis.
- •
Modified selective neurectomy is the only treatment of synkinesis that preserves the natural neural pathway while maintaining long-lasting results.
- •
The patient regains their natural smile without sacrificing cosmesis.
- •
The depressor anguli oris, platysma, buccinator, and mentalis are the synkinetic muscles that prevent a natural smile.
Introduction
Postfacial paralysis with synkinesis presents with a multitude of facial movement disorders. In addition to smile dysfunction, patients can present with unintentional motion of the face when a voluntary motion is attempted. The most common unintentional movements are that of the oral commissure with eye closure (oculo-oral) and eye closure with talking or smiling (oro-ocular). Although the cause of synkinesis is poorly understood, aberrant nerve regeneration has been considered as the most likely cause. Aberrant regeneration describes the regrowth of a motor nerve following nerve injury, producing multiple terminal axons that innervate nonnative muscle groups. , The physical manifestations of synkinesis has not been clearly elucidated. However, recent studies have confirmed that the smile dysfunction is likely secondary to overactivity of counterproductive muscles that cause downward and lateral oral excursion such as the depressor anguli oris, platysma, buccinator, mentalis, and orbicularis oris. These counteractive muscles concurrently contract with variable strength leading to synkinesis. In addition to smile dysfunction, this involuntary and variable muscular contraction can also cause the patient to experience oral incompetence.
Initial treatment of postparalytic synkinesis has been focused on chemodenervation with botulinum toxin type A (BTA) with or without concurrent physical therapy. This treatment approach has produced objective and subjective results, including improved facial symmetry, reduced involuntary muscle contractions, and enhanced quality of life. The role of physical therapy should not be understated; neuromuscular retraining with BTA injections can lead to persistent improvement in synkinesis and imbalance after the chemodenervation wears off.
Static and dynamic surgical options have been used extensively to treat patients with facial nerve disorders to improve oral competence and increase oral commissure excursion. Of note, orthodromic temporalis tendon transfer, gracilis functional free muscle transfer, and masseteric and/or hypoglossal to facial nerve transfer have found success and are the widely used methods of treatment. Although the indications for each procedure depend on the surgeon’s preference as well as the cause and timing of the facial palsy, all of these procedures were developed to address complete flaccid paralysis.
Although the existing dynamic reanimation options have clearly improved patient outcomes over the past 2 decades, none addresses the underlying cause of synkinesis. Furthermore, utilization of the motor nucleus of the trigeminal nerve (temporalis tendon transfer and masseteric-facial nerve transfer) as the driving force of smile mechanism results in a nonspontaneous mimetic movement. Dynamic treatment methods such as gracilis muscle free flaps and temporalis tendon transfers further distance the patient from their natural smile by bypassing the native muscles of facial expression for oral commissure elevation. If cross-face nerve grafts are used, the muscles of facial expression are subject to different motor nuclei and variable overall axonal innervation, causing variable strength and timing of contraction. To improve on current treatment methods, the senior author (BA) has shifted the paradigm in the management of smile dysfunction in facial palsy with synkinesis by developing a denervation technique called “modified selective neurectomy” that addresses the underlying cause of smile synkinesis, thereby achieving long-term natural and spontaneous outcome. , This operation results in the most natural treatment of synkinesis, as it preserves the entire neural pathway from the facial motor nucleus in the pons to the muscle fibers. By preserving the innate efferent neural pathway, modified selective neurectomy enables patients to maintain their natural spontaneous smile.
Selective surgical denervation of synkinetic muscles is particularly helpful around the mouth where there is a convergence of muscles around the oral commissure at the modiolus as well as in the upper and lower lip. The synkinetic “tug of war” between these muscles causes smile dysfunction in affected patients. Therefore, reducing muscles that negatively affect the smile at the nerve level can allow the appropriate muscles to activate unencumbered. Chemodenervation in this area has yielded poor smile outcomes because the muscles are in such close proximity that it is very difficult to selectively reduce the activity of counterproductive muscles.
Technical details used in the modified selective neurectomy have resulted in outcomes that are long term. Permanent denervation is completed by excising segments of aberrant facial nerve branches and placing titanium clips to the nerve ends to prevent regrowth. In addition to studies using blinded observers validating long-term results, patients undergoing modified selective neurectomy were also found to have decreased BTA requirements over time. , , Previous denervation techniques to address ocular synkinesis did not yield long-term results likely due to the fact that a singular muscle (orbicularis oculi) is responsible for narrowing eyelid aperture. , There are no counteractive muscles that cause that, and and extensive denervation would be required to avoid recurrence.
Surgical procedure
Preparation/Incision
- •
Patient is transorally intubated and placed under general anesthesia without paralytics.
- •
A standard retrotragal rhytidectomy incision is planned.
- •
The incision and subcutaneous plane of the face is injected with 1:100,000 epinephrine. Lidocaine is not recommended as to avoid inadvertent decrease of neural activity.
- •
Facial nerve monitoring electrodes are placed in the periorbital and perioral regions.
- •
Incision is made with a #15 blade down to the subcutaneous layer.
- •
Dissection
- •
Starting at the temporal hair tuft, subcutaneous dissection is extended medially for 4 to 6 cm from the incision.
- •
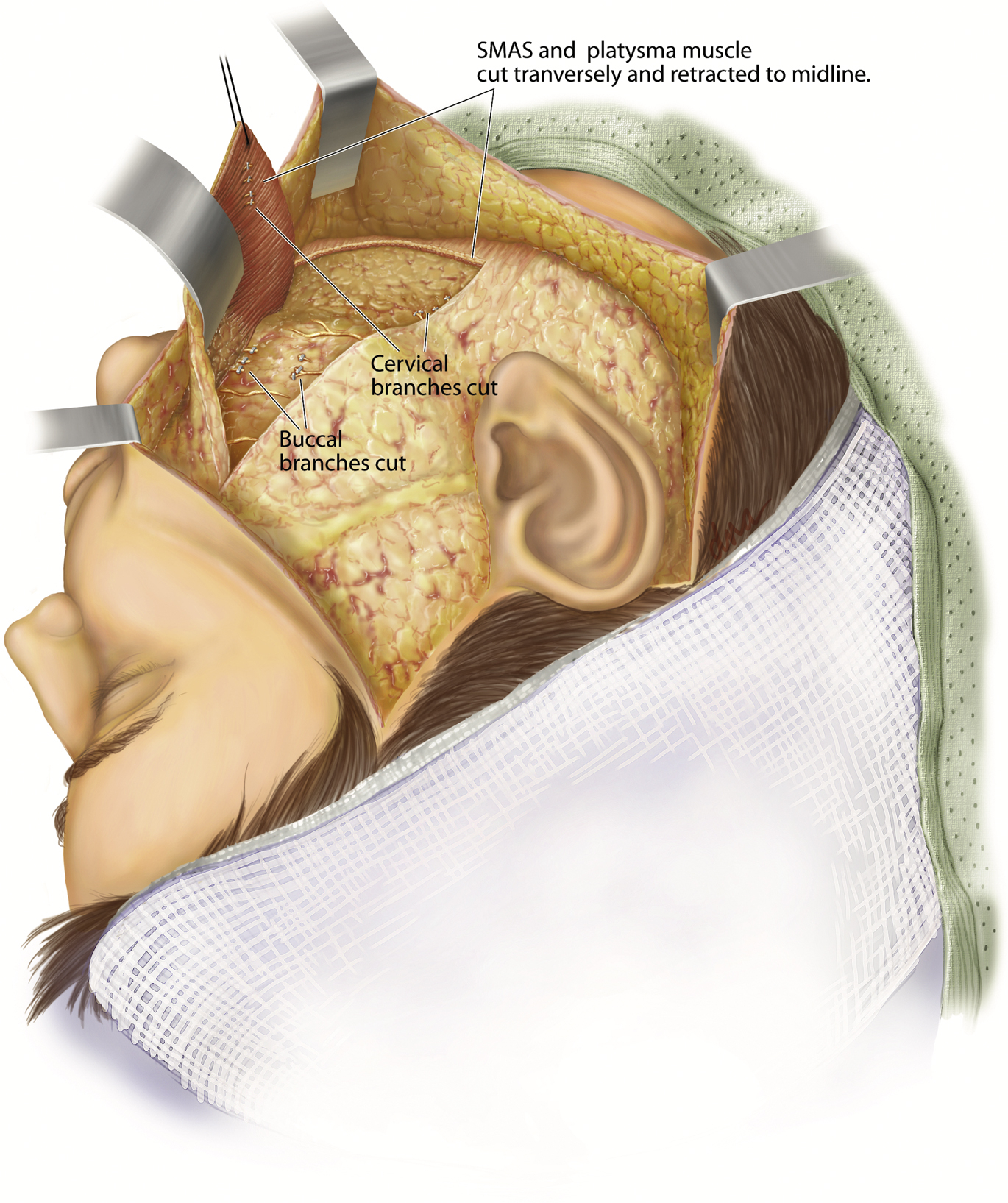
An incision is then made in the superficial musculoaponeurotic system (SMAS) and platysma and in an oblique vector from the lateral zygomatic arch to the cervical region passing through the angle of the mandible.
- •
The SMAS and platysma are elevated as a single flap for 3 to 6 cm.
- •
Dissection is carried out deep to the masseteric and subplatysmal fascia in order to identify the branches of the facial nerve as they exit the parotid capsule ( Fig. 1 ).
Related posts:
 Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
 Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
 Dual Nerve Transfer for Facial Reanimation
Dual Nerve Transfer for Facial Reanimation
 Reinnervation with Selective Nerve Grafting from Multiple Donor Nerves
Reinnervation with Selective Nerve Grafting from Multiple Donor Nerves
 Treating Nasal Valve Collapse in Facial Paralysis
Treating Nasal Valve Collapse in Facial Paralysis
 Facial Reanimation and Reconstruction of the Radical Parotidectomy
Facial Reanimation and Reconstruction of the Radical Parotidectomy

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


- •
