Abstract
In the disorders described in this chapter, the erythema is confined to discrete lesions and is localized to a small area of the body surface. Characteristically the epidermis is spared, but the dermal inflammation may extend into the subcutaneous fat. The three most common examples of localized erythema are: cellulitis , an indurated plaque; abscess and furuncle , each of which is a fluctuant mass; and erythema nodosum , a nodule ( Table 15.1 ).
Chapter Contents
Uncommon Causes of Localized Erythema
| Frequency (%) a | Etiology | History | Physical Examination | Differential Diagnosis | Laboratory Test | |
|---|---|---|---|---|---|---|
| Abscess and furuncle | 0.4 | Staphylococcus aureus (usually) | – | Red, tender, fluctuant mass | Nodular acne Hidradenitis suppurativa | Culture |
| Cellulitis | 0.1 | Group A streptococci (usually) | Fever | Red, warm, indurated, tender area of skin | Contact dermatitis Superficial thrombophlebitis | Culture: Skin aspirate Blood |
| Erythema nodosum | 0.3 | Hypersensitivity reaction | Search for associated conditions, including drug history | Red, tender, deep nodules, usually on lower legs | Thrombophlebitis Pancreatic panniculitis | Chest radiography Throat culture Antistreptolysin-O titers PPD skin test ± skin biopsy |
a Percentage of new dermatology outpatients with this diagnosis seen in the Hershey Medical Center Dermatology Clinic, Hershey, PA.
Abscess and Furuncle
- 1.
Staphylococcus aureus is a common pathogen
- 2.
Recurrent furunculosis often is associated with nasal colonization of S. aureus
- 3.
Check bacterial culture and sensitivity for methicillin-resistant S. aureus
Definition
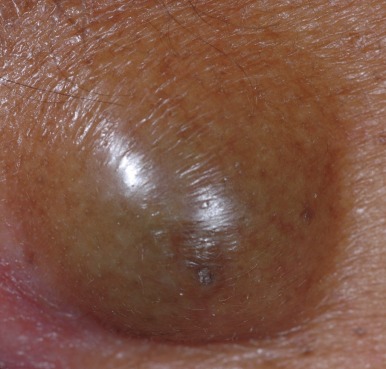
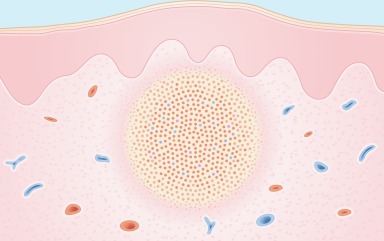
Abscesses and furuncles (boils) are pus-filled nodules in the dermis. S. aureus is the usual pathogen, but Gram-negative organisms and anaerobic bacteria may also be causes. Abscesses often arise from traumatic inoculation of bacteria into the skin, whereas furuncles arise from infected hair follicles. The clinical lesion is a red, tender, fluctuant nodule ( Fig. 15.1 ).
Staphylococcus aureus is the usual pathogen.

Incidence
In one survey, cutaneous abscesses accounted for 2% of all patient visits to the emergency department of a large city hospital. Patients with recurrent furuncles are seen more often by a dermatologist.
History
Patients with abscesses may give a history of preceding trauma, including surgery. Some patients with furuncles give a history of recurrent lesions. Immunodeficiency, intravenous drug abuse, history of atopic dermatitis, and perhaps diabetes mellitus predispose some patients to bacterial infections, but most patients with a furuncle or an abscess have no underlying medical disease.
Physical Examination
Furuncles and abscesses often begin as hard, tender, red nodules that become more fluctuant and more painful with time. Abscesses tend to be larger and deeper than furuncles. Regional lymph nodes are sometimes enlarged, but fever is rarely present.
Differential Diagnosis
Abscesses and furuncles are rarely confused with other entities. Acne and hidradenitis suppurativa can cause pus-filled nodules and cysts. In both conditions, the distribution of the lesions usually provides the diagnostic clue. In nodular acne , multiple lesions are distributed on the face and upper trunk, and other acne lesions (e.g., comedones, papules, pustules) are usually present. In hidradenitis suppurativa , draining nodules are present in the axillary, inguinal, and perineal areas. These nodules are often accompanied by open comedones and scars ( Fig. 15.2 ).

The most commonly mistaken diagnosis for an abscess is a ruptured epidermal inclusion cyst . The intense inflammatory reaction to keratin, usually contained by the cyst lining, creates a fluctuant nodule, most commonly located on the back. Lack of fever, prior history of a cyst, and the presence of a punctum on top of the cyst are distinguishing factors. Primary treatment includes incision and drainage ( Fig. 15.3 ).
- ●
Nodular acne
- ●
Hidradenitits suppurativa
- ●
Ruptured epidermal inclusion cyst
Laboratory and Biopsy
The diagnosis is usually made clinically and confirmed by routine culture of the purulent material that has been obtained from incision and drainage. Methicillin-resistant S. aureus (MRSA) is an emerging pathogen in hospitals and communities, and needs to be checked by requesting a culture and sensitivity. In immunocompromised patients, anaerobic cultures may be desired. Blood cultures are rarely positive and are not indicated unless the patient has signs of sepsis.
Biopsy is rarely indicated. If biopsy is performed, a large, dense collection of neutrophils will be found in necrotic dermis ( Fig. 15.4 ).
Therapy
The principal therapy consists of incision and drainage. In a study of 135 patients, this approach resulted in complete healing in all patients, including those who did not receive systemic antibiotics. Systemic antibiotics, however, may result in involution of early lesions, may prevent progression of nodular lesions to fluctuant ones, and may decrease contagiousness. Because S. aureus is the organism usually responsible, the antibiotic of choice is cephalexin (Keflex) or dicloxacillin, in doses of 250 to 500 mg four times daily for 1 week. Choice of antibiotic is also based on the culture and sensitivity of the organism, especially with the emergence of MRSA. If the clinical response is poor, a change in antibiotic therapy can be considered. For this, culture results are helpful.
Initial
- ●
Incision and drainage
- ●
Antibiotics:
- ●
Beta-lactamase-resistant penicillin (e.g., dicloxacillin 250 mg q.i.d.)
- ●
First-generation cephalosporin (e.g., cephalexin 250 mg q.i.d.)
- ●
Alternative – for MRSA Most Commonly
- ●
Antibiotics:
- ●
Trimethoprim-sulfamethoxazole
- ●
Doxycycline
- ●
Parenteral antibiotics
- ●
Course and Complications
Untreated lesions often rupture and drain spontaneously. After surgical or spontaneous drainage, healing usually occurs. Large lesions may leave scars.
In patients with recurrent furunculosis, an underlying predisposing systemic defect may be considered, but usually is not found. Many such patients, however, harbor S. aureus in sequestered mucocutaneous sites, the most common of which is the nose. Other sites of colonization include the axillae and groin. Of U.S. citizens, 1.5% are carriers for MRSA, harboring the bacteria in the anterior nares. In such patients, the regular use of antiseptic agents may decrease bacterial colonization and thereby prevent furuncles from recurring. The authors recommend a total body scrub every other day with an antiseptic cleansing agent such as chlorhexidine or benzoyl peroxide wash and daily nasal application of an antibiotic ointment such as mupirocin.
Patients with recurrent furuncles are often staphylococcal carriers.
Pathogenesis
For abscesses and furuncles, the bacteria usually gain entry to the dermis by an external route. For abscesses, this may be a traumatic inoculation such as a puncture wound, laceration, or surgical incision.
For furuncles, the bacteria enter by a hair follicle, in which they form deep folliculitis and extend into the surrounding dermis. In both instances, the presence of a large number of bacteria in the dermis elicits a vigorous inflammatory response and eventuates in a massive collection of inflammatory cells, primarily neutrophils.
In atopic dermatitis, low levels of the innate immune system’s antimicrobial peptides, beta defensins and cathelicidins, predispose patients to infections, such as abscesses from S. aureus ( Fig. 15.5 ).










