(1)
Department of Anatomy, Medical School Democritus University of Thrace, Alexandroupolis, Evros, Greece
Abstract
The area surrounding the mouth is constituted by two anatomically and surgically related subunits: the lips and the chin. The lips are important structures that dominate in facial aesthetics but are also valuable in function being a motile organ. Its shape and thickness differs between the upper and lower lip and varies significantly from individual to individual. Structurally each lip is composed of the orbicularis muscle that is invested extraorally by the skin and subcutaneous tissue, intraorally by mucosa and submucosa, and over its free edge by the vermilion. The chin is the round-shaped area just inferior to the lower lip and corresponds to the osseous chin. Its skin, the subcutaneous tissue, and the chin muscles structure the chin. The perioral area provides flaps that mainly reconstruct only the lips and the chin. These flaps are largely based on an arterial circle that surrounds the mouth.
The area surrounding the mouth is constituted by two subunits: the lips and the chin. These are examined together because anatomically they share almost the same structures and from a surgical point of view the excision of lower lip lesions and the reconstructive flaps that are designed very often involve both areas.
The lips are not only an important structure that dominates in facial aesthetics but also a valuable in function, motile organ that plays a major role in food intake, speech, and facial expression. Its shape and thickness differs between the upper and lower lip and varies significantly from individual to individual and among the ethnic groups. The chin is the round-shaped area just inferior to the lower lip and corresponds to the osseous chin (mental protuberance and mental tubercles of the mandible).
6.1 Subunits-Topographic Landmarks
The lips and the chin are bounded (Fig. 6.1) from the cheek superiorly by the nasolabial crease and inferiorly by the labiomandibular crease. Both creases correspond to the line where the cheek muscles attach to the orbicularis oris. In young persons, they are shallow and they deepen during aging process becoming more obvious. Superiorly the upper lip is separated from the nose by the alar facial sulcus and the nasal base. Inferiorly the inverted U-shaped mentolabial crease separates the lower lip from the chin. All of the perioral creases are ideal sites for placing and hiding the incisions of many flaps designed for lip reconstruction.
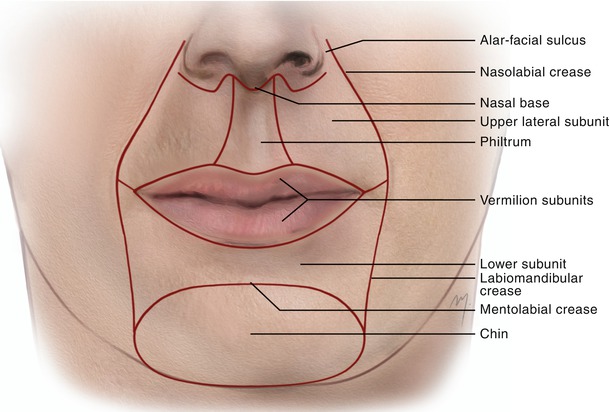
Fig. 6.1
Boundaries and subunits of the lips and chin
Both lips are divided into the upper and lower vermilion subunit (mucosal lips) and the upper and lower cutaneous lip (skin lips) subunits. The upper lip is further divided into a central subunit: the philtrum and two lateral subunits.
The chin constitutes a single unit and is bounded superiorly by the mentolabial crease, inferiorly by the inferior border of the osseous chin, and laterally by the rounded and shallow lateral extensions of the mentolabial crease.
The philtrum of the upper lip (Fig. 6.2) constitutes an aesthetically important anatomic area in the upper lip. This shallow groove exhibits a width that is about one-fifth of the total width of the upper lip and is bounded in both of its lateral sites by two columns, the philtrum columns. The columns are formed by a thickening of the orbicularis muscle and an increase of connective tissue (Latham and Deaton 1976; Briedis and Jackson 1980). Garcia de Mitchell et al. (2008) implied that the columns coincide with ascending arterial branches that originate from the superior labial arteries and a membrane extending from the underlying muscle to the dermis. Superiorly the philtrum attaches to the columella and inferiorly at the free lip edge forms the tubercle. Corresponding to the tubercle, a shallow dimple is presented in the lower lip, where the tubercle rests in lip closure. The junction between the skin and the red part (vermilion) in the upper lip forms in its middle a double curved line, the Cupid’s bow (Cupid: Roman God of love). The two peaks of the bow concur with the lower end of the philtrum columns. The normal cutaneous-vermilion junction is a result from the anterior projection of the pars marginalis of the orbicularis oris muscle (Mulliken et al. 1993). The vermilion of the upper and the lower lips join at the corner of the mouth and form the oral commissure (labial commissure).
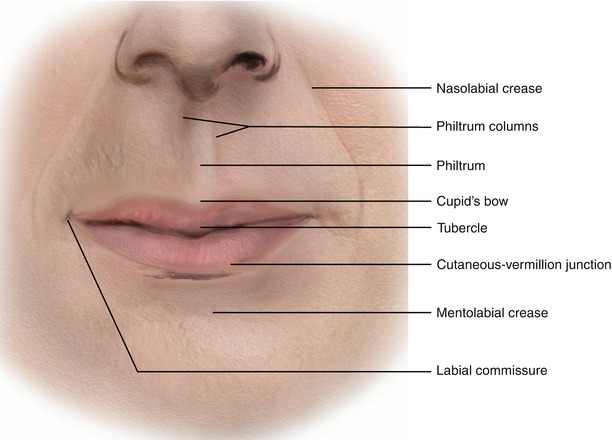
Fig. 6.2
Topographic landmarks of the lips
The above aesthetic subunits and anatomic landmarks should be taken into account when planning and performing reconstruction of the lips to achieve optimal functional and cosmetic results as far as at the lips any distortion of them is very obvious.
6.2 Anatomy
Structurally each lip (Fig. 6.3) is composed of a muscle, the orbicularis muscle that is invested extraorally by the skin and subcutaneous tissue, intraorally by mucosa and submucosa, and over its free edge by the vermilion. The orbicularis muscle is the muscular component of the lip that occupies great amount of the structure creating its bulk. This component provides the lips with a great elasticity allowing them to be stretched in a considerable degree that facilitates in the closure of lip defects. The chin (Fig. 6.3) is structured by its skin, the subcutaneous tissue, and the chin muscles.
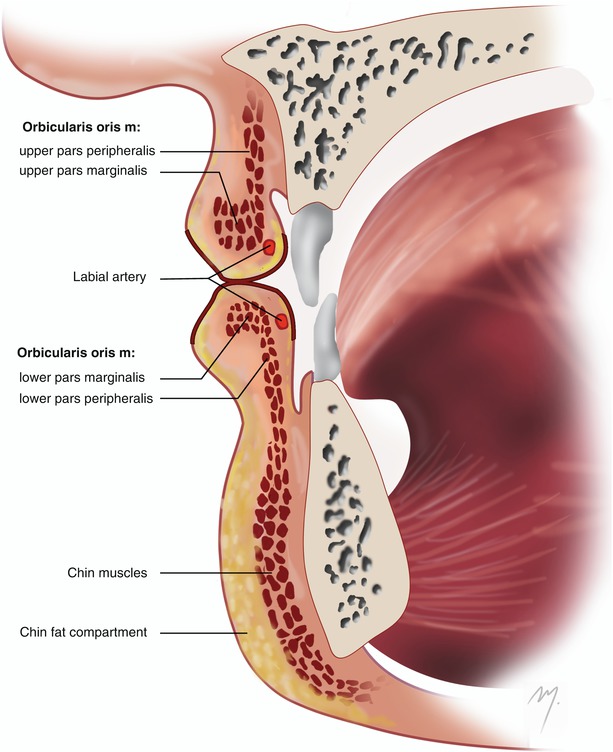
Fig. 6.3
Cross section of lips and chin
6.2.1 Skin and Subcutaneous Tissue-Mucosa-Vermilion
The skin surrounds the outer surface of the lip whereas the mucosa its inner surface. A transition area that differs in the keratinization pattern surrounds the free external lip surface and is named the vermilion (or the vermilion border).
The skin of the lips is similar but slightly thinner (mean 1.9 mm) to that of the adjoining cheek, containing hair follicles, predominantly in the male, and sebaceous and sweat glands. The subcutaneous tissue consists of connective tissue and muscular fibers. Subcutaneous adipose tissue is almost absent in the lips. The subcutaneous tissue is firmly attached to the underlying orbicularis oris muscle. The skin of the chin constitutes the continuation of the lip skin containing also hair follicles predominantly in the male and sebaceous and sweat glands but becomes much thicker. It is the thickest skin of the face, with an average thickness of 2.6 mm. Although subcutaneous fat is almost absent at the lips, at the chin area, it fills a distinct subcutaneous compartment, the chin fat compartment (Fig. 6.3). The relaxed skin tension lines (RSTLs) on the perioral area run in a curved vertical direction as they descend to the mandibular border (Fig. 6.4).
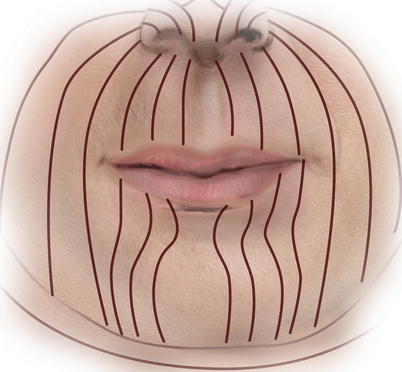
Fig. 6.4
Relaxed skin tension lines (RSTLs) at the lips and chin
The lip mucosa is similar to the neighboring buccal mucosa. The submucosa layer contains numerous minor salivary glands and is loosely connected to the underlying muscle. This provides an easy surgical plane that separates the mucosa from the muscle and can be used as an advancement mucosal flap.
The vermilion consists of very thin mucosa, with no or only few glands beneath it. The numerous underlying blood capillaries impart its red color. It is of various breadth and narrows to the commissures. The transition from vermilion to mucosa usually occurs just posterior to the line of lip closure. Vermilion continuity must be ensured in every lip reconstruction; especially in the vermilion-skin junction, as well as every asymmetry above 1mm of this line is very obvious.
6.2.2 Muscles
6.2.2.1 Orbicularis Oris Muscle
The orbicularis oris muscle (Fig. 6.5) is a round-shaped, circumferential muscle constituting the muscular substance of the lips and being the primary mediator of oral competence. This multilayered muscle is divided in two parts, the large pars peripheralis located posteriorly and the small pars marginalis located anteriorly. The muscle fibers that constitute each part differ not only in their anatomic location but also in their immunohistochemical characteristics (Hwang et al 2007a). The small pars marginalis is limited to the vermilion, although it has been reported that in the upper lip, it extends for a few millimeters above the vermilion border (Hwang et al. 2007a, b).
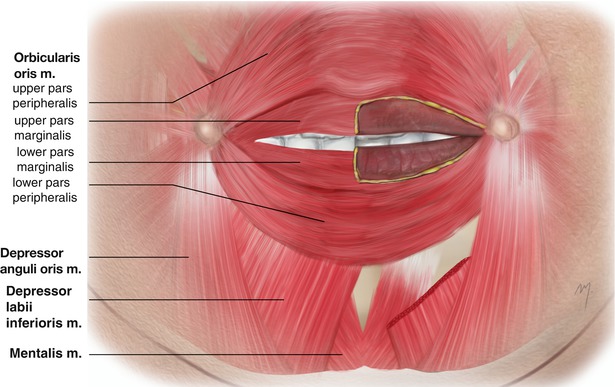
Fig. 6.5
Muscles of the lips and chin. The orbicularis oris muscles are divided in the pars marginalis and the pars peripheralis
Strictly anatomic the orbicularis muscle differs from a “real” sphincter (e.g., the orbicularis oculi muscle) with the manner of undisrupted running fibers that surround an opening. The pattern of its complicated micro-architecture has been controversial over the years (Lightoller 1925; Nairn 1975; Latham and Deaton 1976; Briedis and Jackson 1980; Williams and Warwick 1980; Mooney et al. 1988; Namnoum et al. 1997; Hwang et al. 2007b). However, the old detailed description of Lightoller (1925) is still accepted (Standring 2008). According to this description, the orbicularis oris muscle consists of a left and a right upper pars peripheralis segment, a left and right lower pars peripheralis segment, and the corresponding pars marginalis segments. Each of the parts is fan-shaped with their stem attached to the modiolus (see below), where these constituents are open in the pars peripheralis and closed in the pars marginalis.
The fibers of the pars peripheralis originate within the modiolus and are reinforced by fibers of buccinator, zygomaticus major, and levator anguli oris muscles in the upper lip and by the fibers of buccinator and depressor anguli oris muscles in the lower lip. The fibers of the pars peripheralis travel in various directions (transversally, longitudinally, and obliquely) (Rogers et al. 2009). They enter the free lip and aggregate toward the medial plane for a few millimeters, where they intermingle with their corresponding opposites, and continue to their dermal insertions. Upper fibers of the upper lip traverse near the nasolabial sulcus and proceed to adhere to the sulcus, the nasal ala, and the septum, whereas the lower fibers of the lower lip attach to the mentolabial sulcus. Fibers of the pars marginalis also originate from the modiolus and they traverse anteriorly to the fibers of the pars peripheralis. They integrate with their contralateral pairs and extend a few millimeters past the midline and attach to the vermilion zone (Latham and Deaton 1976; Standring 2008).
6.2.2.1.1 Incisivus Labii Superioris and Incisivus Labii Inferioris Muscles
Two muscular slips are associated as accessory muscles of the orbicularis oris: the incisivus labii superioris and the incisivus labii inferioris muscles. These muscles actually connect the orbicularis oris to the maxilla and the mandible.
The incisivus labii superioris muscle is attached to the incisive fossa of the maxilla, deep to the orbicularis oris. Its fibers run lateral, parallel to the fibers of the orbicularis oris muscle blending with them. They attach at the modiolus and blend with fibers of the levator anguli oris muscle (Standring 2008).
The incisivus labii inferioris muscle is attached to the incisive fossa of the mandible, lateral to the mentalis and initially deep to the orbicularis oris. Its fibers curve laterally and superiorly to the angle of the mouth and attach to the modiolus (Standring 2008). The muscle is present in approximately 98 % and merges with fibers of the orbicularis oris and buccinator muscles (Hur et al. 2011).
Deep to the orbicularis muscle, both in the upper and lower lips, the presence of a submuscular fat layer has been described that its volume seems to play an important role to the appearance of the youthful lip and its atrophy results in the aging lip (Rohrich and Pessa 2009).
The orbicularis oris muscle receives its blood supply from the superior and inferior labial arteries, the mental artery, the infraorbital artery, and the transverse facial artery. The buccal and the mandibular branches of the facial nerve supply the motor innervation to the orbicularis oris.
The main function of the orbicularis oris is to close the lips sealing the mouth. The orbicularis oris muscle in association with other muscles is used for the production of labial elevation and depression. These abilities enable the production of speech, the pressing of the labia against the teeth, and the ability to hold food within the mouth during mastication.
6.2.2.2 Depressor Anguli Oris Muscle
6.2.2.3 Depressor Labii Inferioris Muscle
The depressor labii inferioris muscle is a muscle quadrilateral in shape that lies beneath the depressor anguli oris (Fig. 6.5). The muscle originates from the oblique line of the mandible, in an area between the symphysis and the mental foramen, where its fibers blend with fibers of the platysma muscle. The muscle fibers run superomedially and insert into the skin of the lower lip. They blend with fibers of the orbicularis oris muscle. Its action pulls the lower lip downward and laterally. The muscle is supplied by the inferior labial and the mental artery. The marginal mandibular branch of the facial nerve innervates the muscle.
6.2.2.4 Mentalis Muscle
The small mentalis muscle (Fig. 6.5) is located close to the midline. It lies beneath the depressor labii inferioris muscle being the deepest muscle in that area. Immediately deep to each of the mentalis muscle, a layer of fat has been noted that might influence the depth of the mentolabial sulcus (Rohrich and Pessa 2009).
The muscle arises from the mandibular incisive fossa. Its muscle fibers run inferiorly and medially to the midline and insert to the skin of the chin. The muscle directly elevates the chin and wrinkles the skin of the chin. Indirectly it protrudes the lower lip. The muscle is supplied by the inferior labial and the mental artery. The marginal mandibular branch of the facial nerve innervates the muscle.
6.2.2.5 The Modiolus
The modiolus (Fig. 6.6) is a nodular, palpable, and mobile anatomic structure located slightly lateral to each oral commissure. It is formed by several different muscles that are derived from a common embryological origin and converge to the oral commissure (Pélissier et al. 2000).
The modiolus actually appears as a dense, fibromuscular mass formed by the multiple converging fibers of the levator anguli oris, the depressor anguli oris, the pars marginalis of orbicularis oris, the risorius, the buccinator, and the zygomaticus major muscles. Lateral fibers of the depressor labii muscle and medial fibers of the platysma muscle (platysma pars modiolaris) also converge to the modiolus. Not only muscle fibers but also fasciae, like SMAS and parotidomasseteric fascia, contribute to the formation of the modiolus (Al-Hoqail and Abdel Meguid 2009).
The modiolus has a cone-like configuration, with its base adjacent to the buccal mucosa extending to the dermis of the skin (Demiryurek et al. 2003). Its base extends vertically about 20 mm above and 20 mm below a horizontal line through the oral commissure, while its apex is centered about 12 mm lateral to the oral commissure (Standring 2008). Being attached firmly at the dermis, it functions as scaffold that transmits the multiple muscle actions to the oral commissure.
The modiolus plays a very important role not only in function but also in aesthetics, a fact that was portrayed even from the classic ancient Greek era, as Zufferey (2002) has emphasized: “The modiolus has been a well-known morphologic structure since antiquity. No other school of sculpture has better portrayed the modiolus of young adults than the sculptors of classic Hellenic beauty, who recognized the importance of the modiolus.” This small structure should be taken into account in reconstruction in this area so as not to imperil its functional and aesthetical integrity (Fig. 6.6).
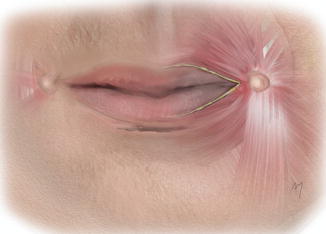
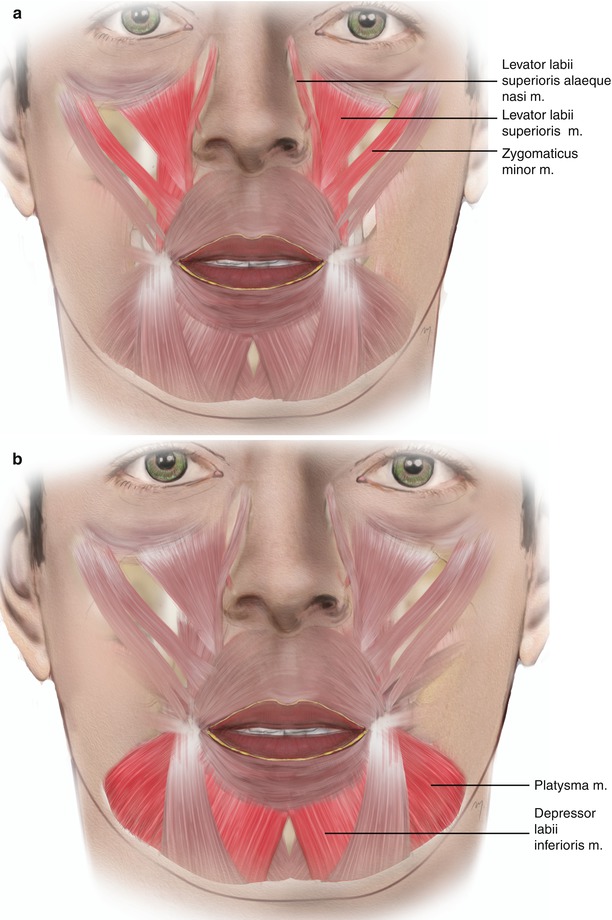
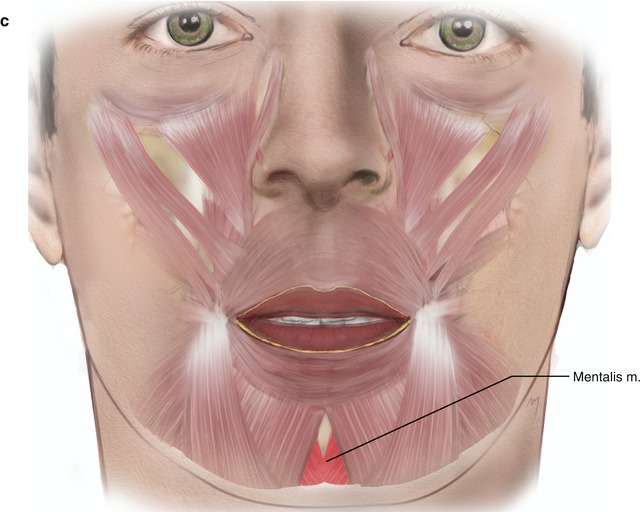
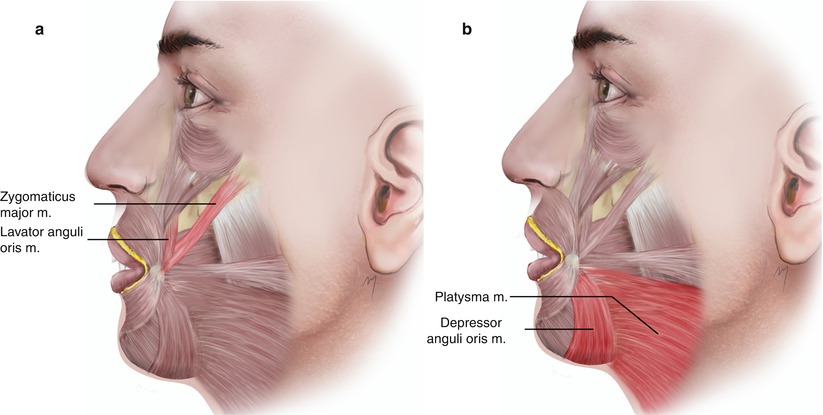
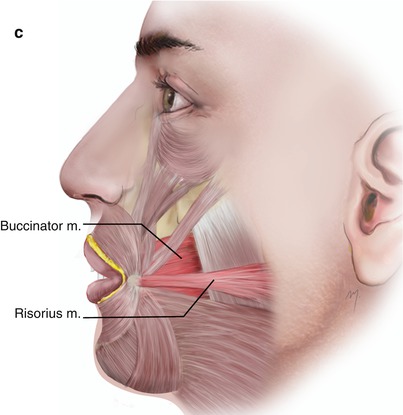
Fig. 6.6
The modiolus
Fig. 6.7
Muscles that act on the lips. (a) Upper lip elevators. (b) Lower lip depressors. (c) Lower lip protruders
Fig. 6.8
Muscles that act at the labial angle. (a) Labial angle elevators. (b) Labial angle depressors. (c) Labial angle retractors
6.2.2.5.1 Muscles that Act on the Lips
All of the cheek and chin muscles, the platysma, and one nasal muscle, the levator labii superioris alaeque nasi, act on the lips. These muscles integrate with the orbicularis oris and work synergistically to allow the full range of lip movement. According to the basic action they induce to the lips, they are distinct in elevators, depressors, protruders, and retractors (Figs. 6.7 and 6.8). Their action can be detected either on the entire lip or on the mouth corner. The upper lip elevators are the levator labii superioris alaeque nasi, the levator labii superioris, and the zygomaticus minor. In the lower lip depressors, the depressor labii inferioris and the platysma are included. The lower lip protruder is only the mentalis muscle. The levator anguli oris and zygomaticus major muscles achieve elevation of the labial angle. The angle of the mouth is depressed by the depressor anguli oris and by fibers of platysma muscle. Lateral retraction of the labial angle is accomplished by the buccinator and risorius. These basic muscle actions to the lips are summarized in Tables 6.1 and 6.2.
Table 6.1
Muscles that act on the lips
Upper lip elevators (Fig. 6.7a) | Lower lip depressors (Fig. 6.7b) | Lower lip protruders (Fig. 6.7c) |
|---|---|---|
Levator labii superioris alaeque nasi | Depressor labii inferioris | Mentalis |
Levator labii superioris | Platysma | – |
Zygomaticus minor | – | – |
6.2.3 Arterial Supply
The arterial distribution of the lips and chin is not constant, showing a great degree of variability in the location, course, and dimensions of these arteries. The lips are supplied mainly by the superior and inferior labial arteries with the contribution of the infraorbital, the mental, the labiomental, and the submental arteries. The chin is supplied mainly by the mental artery, the labiomental artery, and the terminal part of the submental artery, while small branches of the inferior labial artery contribute to the vascularization of its upper part.
6.2.3.1 Superior Labial Artery
The superior labial artery (Fig. 6.9) originates from the facial artery at most times superior or at the level of the labial commissure and occasionally inferior to it. The diameter of the superior labial artery at its origin ranges from 1 to 1.8 mm (Park et al. 1994; Crouzet et al. 1998; Magden et al. 2004; Pinar et al. 2005; Al-Hoqail and Meguid 2008).
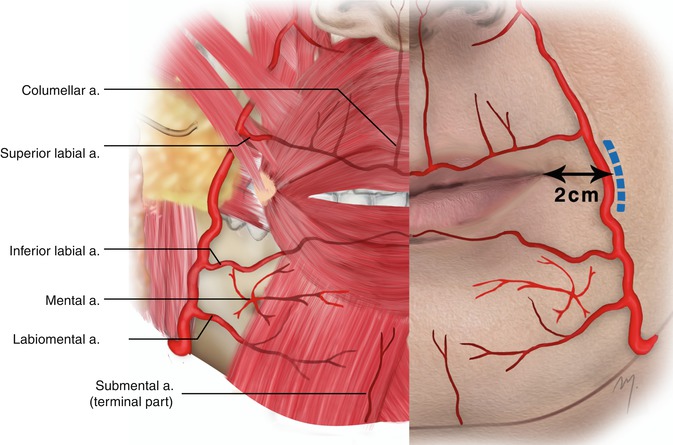
Fig. 6.9
Arterial supply to the lips and chin (the depressor anguli oris muscle has been removed)
The point at which the superior labial artery branches from the facial artery and the distance between its origin and the labial commissure is highly variable (Fig. 6.10) ranging from 0.4 to 2.5 cm, with a mean distance between 1.0 and 1.8 cm (Schulte et al. 2001; Loukas et al. 2006; Magden et al. 2004; Al-Hoqail and Meguid 2008). This point depends on the branching pattern of the facial artery and on the distance that the facial artery passes from the labial commissure. Thus, accurate landmarks cannot be determined.
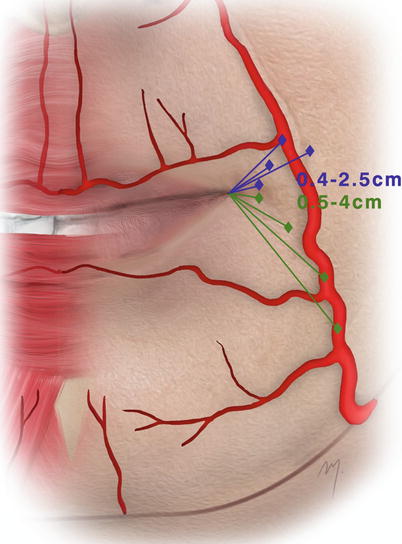
Fig. 6.10
Range of the distances of emerging points of the superior labial artery (blue lines) and the inferior labial artery (green lines) from the oral commissure
The superior labial artery travels forward in a tortuous course to the upper lip, passing deep to the zygomaticus major muscle. The superior labial artery is usually larger and more tortuous in its course than the inferior one. Into the upper lip, it enters the orbicularis oris muscle and travels between the muscle and the mucosa, along the edge of the upper lip. In about 15–20 %, the artery runs partially invested by the muscle (Schulte et al. 2001; Loukas et al. 2006).
Several small branches ascend contributing to the vascularization of the nostril base. A larger artery that branches at the philtrum and ascends to the columella of the nose is named the columellar artery (see Chap. 4). Finally the superior labial artery anastomoses with its contralateral forming the upper lip arterial arc.
6.2.3.2 Inferior Labial Artery
The inferior labial artery (Fig. 6.9) is branched from the facial artery generally below or at the level of the labial commissure and seldom above it. Its mean diameter in its origin ranges from 1.2 to 1.4 mm (Edizer et al. 2003; Pinar et al. 2005; Al-Hoqail and Meguid 2008). As with the superior labial artery, the point at which the inferior labial artery branches from the facial artery and the distance between its origin and the labial commissure exhibit a high variability (Fig. 6.10) ranging from 0.5 to 4 cm with a mean distance between 2 and 2.5 cm, whereas there are cases where it originates even at the lower margin of the mandible (Edizer et al. 2003; Pinar et al. 2005; Al-Hoqail and Meguid 2008).
After branching from the facial artery, it runs tortuously upward and forward deep to the depressor anguli oris muscle in its course to the lower lip. The artery penetrates the orbicularis oris muscle and runs tortuously along the edge of the lower lip lying between the muscle and the mucous membrane. In about 13 %, the artery can be found traveling within the orbicularis oris muscle (Schulte et al. 2001).
6.2.3.3 Mental Artery
The mental artery (Fig. 6.9) is a terminal branch of the inferior alveolar artery (which in turn is a branch of the maxillary artery). As the inferior alveolar artery runs within the mandibular canal, together with the inferior alveolar nerve, at the premolar teeth root level, it divides into the incisive and the mental arteries. The mental artery emerges onto the chin area through the mental foramen, while the incisive artery continues to the midline, below the lower incisors. Its branches supply the chin muscles and the overlying skin and anastomose with the terminal part of the submental artery and the inferior labial arteries.
6.2.3.4 Labiomental Artery
The labiomental artery (Fig. 6.9) is an inconstant branch of either the facial or the inferior labial arteries. It contributes to the vascular supply of the mental area and the lower lip. After emerging it runs horizontally between the depressor anguli oris and the depressor labii inferioris muscles to the midline. It anastomoses with branches of the mental artery and the terminal part of the submental artery.
6.2.3.5 Terminal Part of Submental Artery
The central part of the chin is mainly vascularized by the terminal part of the submental artery (Fig. 6.9). The submental artery is a cervical branch of the facial artery that initially courses below the mandible and as it reaches the midline turns and ascends vertically to the chin (see Chap. 8). It anastomoses with the mental, the labiomental, and the inferior labial arteries. It mainly supplies the skin of the chin and contributes to the supply of the lower lip.
6.2.4 Venous Drainage
Although in the classic anatomic textbooks a superior and an inferior labial veins are mentioned, from a surgical point of view, the lip venous system does not exhibit any sizable and distinguish vessel. A diffuse network of small venae comitantes coalesces into the facial vein draining the lips (Carty and Pribaz 2010) (Fig. 6.11). In a similar manner, the chin is drained by a network of unnamed small veins. The mental vein contributes to the venous system of the chin draining into the pterygoid venous plexus.
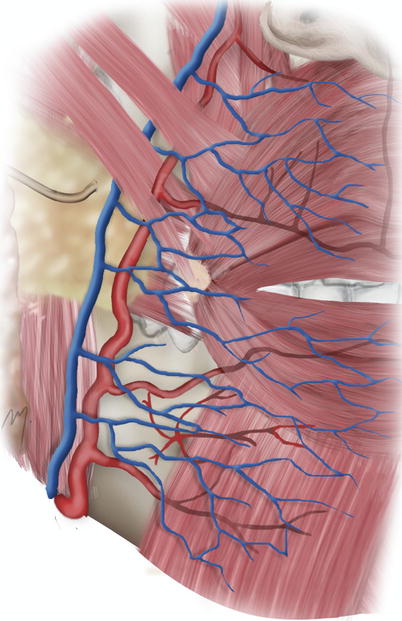
Fig. 6.11
Venous drainage of the perioral area
6.2.5 Innervation
6.2.5.1 Motor Innervation of Lips and Chin
The motor innervation to the lips and chin (Fig. 6.12) is provided by the zygomatic, the buccal, and the marginal branches of the facial nerve that innervate all of the perioral muscles.
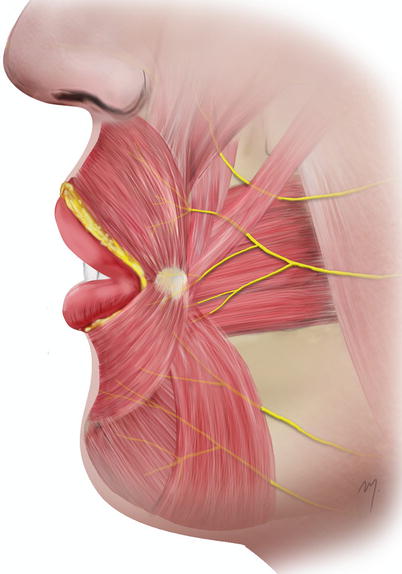
Fig. 6.12
Motor innervation to the lips and chin
The lip elevators are supplied by the zygomatic and buccal branches, the lip depressors by the marginal mandibular branches, and the lateral retractors by the buccal branches. The fibers of the facial nerve branches enter the perioral muscles usually in a radial form from their undersurface.
6.2.5.2 Sensory Innervation of the Lips and Chin
Sensation to the upper lip is mediated by the superior labial branches of the infraorbital nerve (V2). The lower lip and the chin derive sensibility from branches of the mental nerve (V3).
6.2.5.2.1 Superior Labial Branches of the Infraorbital Nerve
The superior labial branches of the infraorbital nerve (Fig. 6.13) (see also Chap. 5) originate from the infraorbital nerve immediately after it exits through the infraorbital foramen to the face. They run inferiorly beneath the levator labii superioris muscle and distribute to the skin and the mucosa of the upper lip.
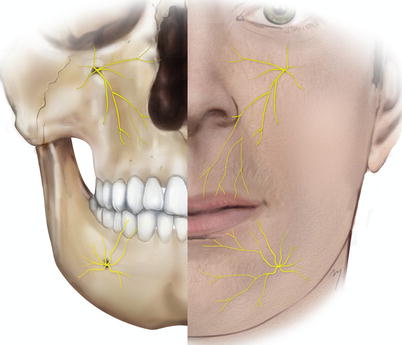
Fig. 6.13
Sensory innervation to the lips and chin
6.2.5.2.2 Mental Nerve
The mental nerve (Fig. 6.13) is the terminal part of the inferior alveolar nerve. The inferior alveolar nerves run through the mandibular canal, in company with the mandibular vessels. They exit in the chin through the mental foramen and upon exiting are termed mental.
Mental Foramen
The mental foramen shows a great variability in its position. It shows differences among ethnic groups and between genders (Greenstein and Tarnow 2006; Santini and Alayan 2012










Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
