(1)
Department of Anatomy, Medical School Democritus University of Thrace, Alexandroupolis, Evros, Greece
Abstract
The forehead could be considered as the hairless frontal elongation of the scalp. Being an anatomical continuity of the scalp, it consists of the same five distinct layers: the skin, connective subcutaneous tissue, galea aponeurotica, loose areolar connective tissue, and periosteum. The forehead arterial system consists of a latticework of anastomoses supplied from the supraorbital and the supratrochlear arteries and the frontal branches of the superficial temporal vessels. Additionally, the dorsal nasal artery contributes to the blood supply of the mid-forehead area. The forehead constitutes a wide donor site of flap material that can be harvested in great quantity. Flaps derived from the forehead can be used in closing its own defects, but the forehead is also the ideal donor site of regional flaps in order to reconstruct medium and large nasal defects.
The forehead is a prominent element that constitutes the upper face. In its midsection, it is slightly convex, flatters laterally, and becomes concave as it transitions to the temple.
The anatomic boundaries of the forehead (Fig. 3.1) are the anterior hairline superiorly and inferiorly the nasion, the glabella, and the eyebrows. The lateral ends of the eyebrows determine the lateral borders of the main forehead. The temporal area extends beyond this borderline.
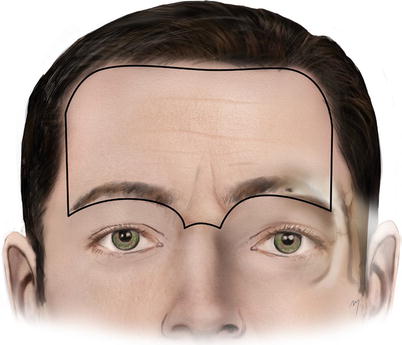
Fig. 3.1
Boundaries of the forehead
The anterior hairline defines the upper limit of the forehead and is the boundary between it and the scalp, but in the presence of alopecia, it cannot be a stable landmark. In this case, the superior border is determined by the superior edge of the frontalis muscle.
The glabella is a bony structure in the smooth elevation between the superciliary arches. As forehead subunit, glabella is the smooth and hairless area between the eyebrows. However, during the aging process, transverse and vertical glabellar rhytides begin to appear.
The supraorbital rims are palpable along their whole length as a sharp prominence in the lateral two-thirds and rounded in the medial third. At the junction of the medial third and lateral two-thirds, the supraorbital notch can also be felt.
The eyebrows are two arched, hair-covered skin ridges lying over the supraorbital rims, protecting the eyes from flowing forehead sweat and sunlight. The position and contour of this minor forehead anatomic feature play a major role in the aesthetic appearance and must be taken into great account, to avoid its distortion when planning forehead flaps. Eyebrow shape and position change depending on gender. In males, the brow is more horizontal and thicker and is found in a lower position at the level of supraorbital rim. In females, the brow is more arched, thinner, and in a somewhat higher position, above the level of the supraorbital rim. Approximately 200–250 short and thick hairs (without having arrector pili muscles) are set in the eyebrows. The number of eyebrow hair remains almost stable during life, with the exception of older males where, during the aging process, growth of eyebrow hair increases. When making incisions to the eyebrow and elevating a flap in this area, it is very important to know the direction of the hair in order to cut parallel to them. In the medial eyebrow part, hair follicles are all directed superiorly; in the upper portion of the central and lateral parts of the brow, follicles are directed inferiorly; and in the lower portion, follicles are directed superiorly (Lemke and Stasior 1982). Muscle fibers insert into the dermis of the eyebrow, moving it in several directions. The eyebrow mobility is significant in creating the full range of emotional expressions of the face. The frontalis muscle acting as a brow elevator achieves these movements, while the antagonistic procerus, corrugator, orbicularis oculi, and depressor supercilii act as brow depressor muscles.
3.1 Layered Anatomy of Forehead
The forehead could be considered as the hairless frontal elongation of the scalp. Being an anatomic continuity of the scalp, it consists of the same five distinct layers: the skin, connective subcutaneous tissue, galea aponeurotica, loose areolar connective tissue, and periosteum (Fig. 3.2).
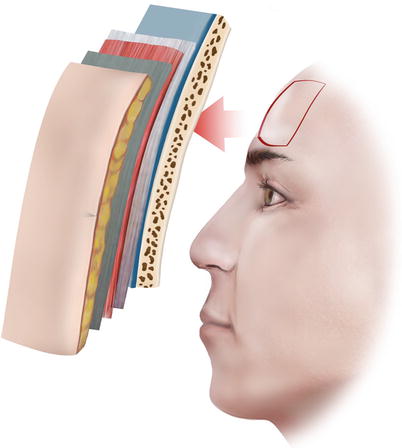
Fig. 3.2
The forehead consists of the same five layers of the scalp
3.1.1 Skin and Subcutaneous Tissue
The skin and subcutaneous tissue of the forehead (first and second layer, respectively) are very firmly attached, and therefore it is very difficult to work with it individually from a surgical perspective.
The forehead skin, rich in sebaceous and sweat glands, is one of the thickest skins of the face with an average thickness of 2.4 mm. It varies from one individual to other but also changes by age and sun exposure. The skin of the forehead decreases progressively in thickness and sebaceous gland concentration, when moving from the suprabrow area toward the anterior hairline. This occurs in the same manner in the temporal region when moving from the lateral canthus to the scalp hairline. The central forehead skin is densely adherent to the abundant underlying subcutaneous tissue forming a soft tissue layer that is relatively thick, rigid, and minimally mobile. From the medial to lateral regions, the mobility increases. In the temporal area, the connections are loose, to the underlying temporalis fascia, which results in enhanced skin mobility over this area. Thus, the lateral forehead temporal region may act as a tissue reservoir for reconstruction of more medially located defects (Vuyk 2006; Sykes 2009).
The relaxed skin tension lines (RSTLs) on the forehead run horizontally slightly curving in a vertical direction laterally. At the glabellar region, they are vertically oriented (Fig. 3.3).

Fig. 3.3
Relaxed skin tension lines (RSTLs) at the forehead
The subcutaneous tissue is richly vascularized containing a homogenous layer of adipose tissue. The subcutaneous fat of the forehead attaches to the underlying galea aponeurotica by fibrous septa, which contain vessels, nerves, and lymphatics. Also numerous transverse fibrous septa from the frontalis muscle to the dermis are found within this layer in the forehead (Sykes 2009). These septa are partially responsible for the deep, horizontal forehead lines providing excellent camouflage of scars (Seline and Siegle 2005).
3.1.2 Epicranial Aponeurosis-Forehead Muscular Layer
3.1.2.1 Galea
The epicranial aponeurosis named also galea or galea aponeurotica, as mentioned in the previous chapter, is the thin tendinous sheet of connective tissue that encompasses the entire dome of the skull, joining both the paired frontalis and occipitalis muscles. The galea at the forehead joins the two frontalis muscles but also fills the gap between them sending a short, narrow prolongation between their two bellies (Fig. 3.4). On its course from the upper to the lower forehead, the galea splits several times in various layers, which reunite again to the supraorbital margin (Tarbet and Lemke 1997; Knize 2001, 2007; Sykes 2009). In actuality, the galea is the fibromuscular extension of the superficial musculoaponeurotic system (SMAS), which becomes continuous with the temporoparietal fascia in the temple (Mitz and Peyronie 1976). The galea is loosely connected to the underlying pericranium by the layer of loose areolar connective tissue enabling it to be mobile, thus moving and sliding freely over the pericranium.
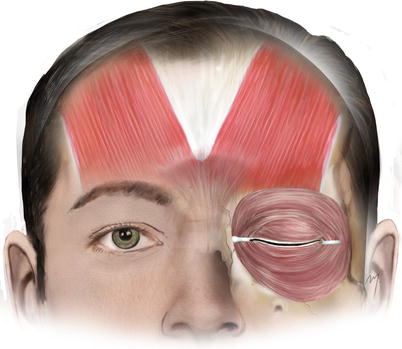
Fig. 3.4
Galea and frontalis muscle
As the galea passes into the upper forehead, it splits into two layers, the superficial galea layer and the deep galea layer which encompass the frontalis muscle.
The superficial layer of galea is thin and lies anteriorly to each frontalis muscle. It covers the surface of the frontalis muscle and continues over the surface of the orbicularis oculi muscle, as a single, filmy layer.
The deep layer of galea is thicker than the superficial and lies under the muscle. As the deep galea layer runs to the supraorbital area, it splits again and envelops a fat pocket, the retro-orbicularis oculi fat (ROOF).
3.1.2.2 Forehead Muscular Layer
The muscular layer of the forehead is composed of frontalis, procerus, corrugator supercilii, depressor supercilii, and the orbital part of the orbicularis oculi muscles. These muscles are arranged in three levels: the superficial level (frontalis, procerus, and orbicularis oculi muscles), the intermediate level (depressor supercilii muscle), and the deep level (corrugator supercilii muscle).
3.1.2.2.1 Frontalis Muscle
The paired frontalis muscles are the frontal parts of the two occipitofrontalis muscles. The frontalis muscles are thin, quadrilateral, and broader with longer fibers than the occipital part that extend from the anterior edge of the epicranial aponeurosis to the eyebrow (Fig. 3.4). The two bellies of the frontalis muscle are placed symmetrically and are vertically oriented, but they leave the mid-forehead region free of muscle fibers. The superior side of the muscle, which is its origin field, lies adjacent to the coronal suture line of the skull. The lateral side of the muscle extends slightly more cephalad than the medial side, and the lateral margin of frontalis muscle is thinner along the superior temporal line (Knize 1996a, b).
The frontalis muscle has no bony attachments and originates from the anterior edge of galea aponeurotica. Its muscle fibers extend toward the supraorbital rim where they merge with those of the adjacent muscles, entering the deep orbicularis oculi muscle surface. The medial fibers of the frontalis blend with those of the procerus muscle. Under the brow, the lateral fibers of the frontalis muscle interdigitate with the corrugator supercilii and the orbital portion of orbicularis oculi muscles.
The insertion of the frontalis muscle fibers represents more of a blend with the other muscle fibers than a direct dermal insertion.
Frontalis muscle receives its arterial supply from branches of the superficial temporal supraorbital and supratrochlear arteries and is innervated by the temporal branches of the facial nerve from its undersurface.
The frontalis muscles, with its fibers offering no true bony insertion but blending with neighboring muscles, are the primary elevators of the brow. Acting from above, they raise the eyebrows and the skin over the root of the nose (expression of surprise, fright, horror). These muscles are antagonistic to the brow depressor muscles (procerus, corrugator, orbicularis oculi, and depressor supercilii), which do have real bony insertions. Acting from below, they draw the scalp forward. Due to the multiple attachments of the vertically oriented fiber septa to the dermis of the forehead skin, they are responsible for the formation of horizontal forehead rhytides. Acting alternately with the occipital muscles, they move the entire scalp backward and forward.
3.1.2.2.2 Procerus Muscle
Procerus is a vertical, flat, thin, and pyramidal shape muscle (Fig. 3.5). Although the procerus belongs anatomically in the group of nasal musculature, functionally it is much more a forehead muscle, involved in eyebrow movement.
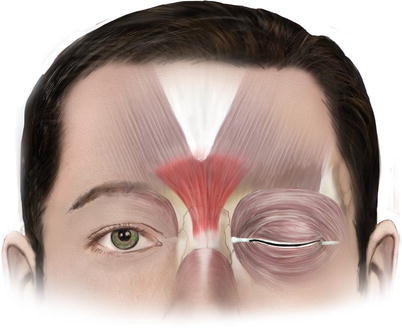
Fig. 3.5
Procerus muscle
It originates at the nasal bone and arises from the tendinous fibers attached to a fibrous fascia that covers the lower part of the nasal bones, the upper part of the lateral nasal cartilage, and the aponeurosis of the transverse part of nasalis (Keller and Mashkevich 2009). All these anatomic elements from where procerus originates are parts of the nasal SMAS (see Chap. 4). The muscle courses superiorly with its fibers oriented vertically, medial to the depressor supercilii muscle and the medial head of the orbicularis oculi muscle. As it courses superiorly, above the nose, the fibers of the procerus become continuous with the medial fibers of the frontalis muscle. The muscle fibers insert into the glabellar skin, in a varied width, over the lower mid-forehead and between the eyebrows.
Procerus receives its arterial supply mainly from branches of the facial artery. It is innervated by the facial nerve and more specifically the angular nerve (the buccal branch of the facial nerve, after receiving a contribution from the zygomatic branch; see Chap. 5) (Caminer et al. 2006). The frontal branch of the facial nerve contributes also to the innervation of the upper portion of the muscle.
The procerus is a brow depressor that draws down the medial angle of the eyebrow (frowning, “concentration,” reduces the glare of bright sunlight) and forms horizontal glabellar furrows.
3.1.2.2.3 Orbicularis Oculi Muscle
The orbicularis oculi is a broad, elliptical, and flat muscle sheet that is regarded as a component of the superficial musculoaponeurotic system (SMAS). The muscle surrounds the circumference of the orbit sealing it (Fig. 3.6). Although it belongs in circumorbital and palpebral musculature group, it spreads into the forehead region interdigitating with the forehead muscles.
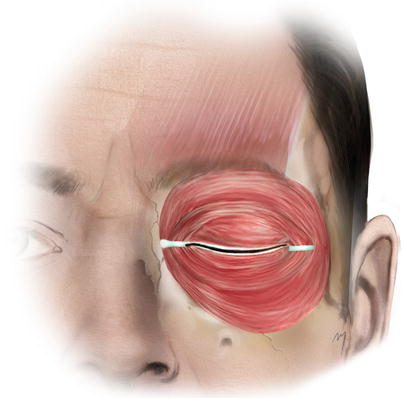
Fig. 3.6
Orbicularis muscle
It consists of three parts, the palpebral, the lacrimal, and the orbital part. The palpebral part (divided topographically in a preseptal and a pretarsal portion), thin and pale, arises from the superficial surface of the medial canthal ligament and from the bone immediately above and below the ligament. The fibers sweep across the eyelids anteriorly to the orbital septum and interlace at the lateral commissure to form the lateral palpebral raphe. The lacrimal part lies behind the lacrimal sac, attached to the lacrimal fascia, to the upper part of the crest of the lacrimal bone, and adjacent part of the lateral surface of the lacrimal bone. The orbital part, thicker than the other two, is the part involved in the lower forehead. It lies over the supraorbital rim and interdigitates with the neighboring forehead muscle fibers.
Orbital Part of the Orbicularis Oculi Muscle
The muscle fibers of the orbital part arise from the superior edge of medial canthal ligament, the nasal component of the frontal bone, and the frontal process of the maxilla. The fibers arc superiorly and inferiorly over the orbital rim, without interruption on the lateral side, where there is no bony attachment. The upper muscle fibers extend superiorly and intermix with the frontalis and corrugator supercilii muscles. The fibers from the medial part are fixed to dermis under the medial head of the eyebrow (Knize 2000). Some of the medial or lateral fibers of the orbital part of the orbicularis oculi may form distinct muscle bands (medial, lateral muscular bands of orbicularis oculi muscle) that are attached to the cheek skin, to the frontal muscle, or to the zygomatic arch (Park et al. 2011, 2012).
The fibers of the orbicularis, after completing their circular course, insert medially at the inferior edge of medial canthal ligament, just below their points of origin.
The orbicularis attaches only medially to the medial orbital margin and the medial canthal ligament. Elsewhere, the orbicularis is attached by retaining ligaments from the periosteum to the fascia on its undersurface (Keller and Mashkevich 2009).
The orbicularis oculi is innervated from the temporal, zygomatic, and buccal branches of the facial nerve. The nerves are horizontally oriented and gather to the undersurface of the muscle from its temporal and inferior side. The anterior and middle rami of the frontal branch run deep to the undersurface of orbicularis muscle and innervate the upper and superolateral part of orbicularis. The zygomatic branch innervates the lower and inferolateral part of the muscle. The buccal branch receives a contribution from the zygomatic branch and forms the angular nerve. The angular nerve, running cranially to the medial canthal ligament, sends rami to the undersurface of the low and medial part of orbicularis, on its way to reach the procerus and the oblique head of corrugator supercilii (Caminer et al. 2006). The innervation takes place by means of anastomotic neural plexuses formed by the involved nerves (Nemoto et al. 2001; Ouattara et al. 2004).
The orbital part of the muscle is used in forced eyelid closure. Furthermore, the medial head of this part acts by depressing the medial brow, along with the oblique head of the corrugator supercilii and the depressor supercilii (depressor muscle group for the medial eyebrow) (Knize 2000).
Just under the superolateral portion of the orbicularis muscle is situated a deep fat facial pocket, the retro-orbicularis oculi fat (ROOF).
Retro-Orbicularis Oculi Fat (ROOF)
The retro-orbicularis oculi fat (ROOF) is a transverse band of 5 mm thick fibroadipose tissue, which extends under the orbicularis muscle and the lower part of frontalis muscle enveloped by a split of the deep galea layer (Fig. 3.7). It extends above the orbital rims having a vertical height of approximately 1 cm and across the forehead for an additional 2–5 cm lateral to the supraorbital notch (foramen) (May et al. 1990; Hwang et al. 2007). It is situated superiorly to the orbital septum and the thinner, preseptal fat. In contrast with the orbital fat, which consists of fatty tissue, ROOF contains more fibrofatty tissue (May et al. 1990; Hwang et al. 2007). Through this fat pocket, run the lacrimal nerve and anastomotic veins to the supraorbital vein (Zide 2006). Within ROOF lies the lateral part of the transverse head of corrugator muscle. It plays an important role in eyebrow ptosis, as it slips downward during the aging process and is resected or reduced in aesthetic blepharoplasty operations. The ROOF is considered a part of the overall galea fat pad (which extends cranially for about 2–3 cm beneath the frontalis muscle and between the subdivisions of the deep galea layer) (Knize 2001; Zide 2006). These fat pads act as a brow pillow, allowing it to move freely.
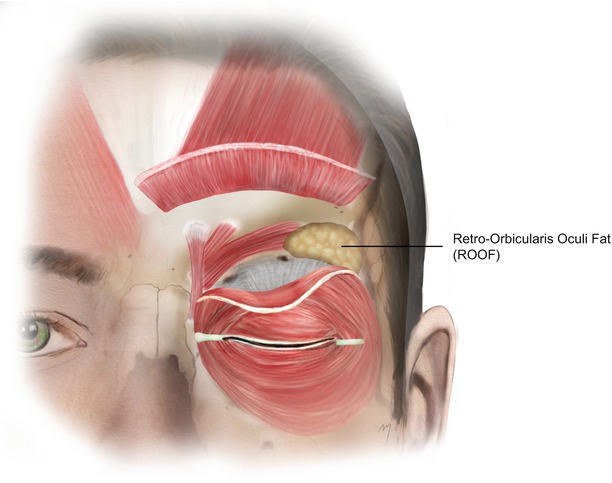
Fig. 3.7
Retro-orbicularis oculi fat (ROOF)
3.1.2.2.4 Depressor Supercilii Muscle
There has been much confusion pertaining to the depressor supercilii muscle, because of the fact that it is difficult to discern whether or not the muscle is an extension of the medial head of the orbicularis oculi muscle or if it is a distinct muscle on its own (Lemke and Stasior 1982; Zide and Jelks 1985; Abramo 1995; Flowers 1998; Macdonald et al. 1998). Just in the late 1990s, Daniel and Landon (1997) confirmed that the depressor supercilii muscle is a distinct entity. Their findings reasserted later on, by Knize (2000, 2001) and Cook et al. (2001) who provided a description and a clear detailed schematic of the muscle.
According to these studies, the depressor supercilii lies anteriorly to the corrugator supercilii muscle and arises from the frontal process of the maxilla approximately 10 mm above the medial canthal tendon, near the edge of the bony medial orbital rim which is slightly posterior and superior to the posterior lacrimal crest, approximately 2–5 mm below the frontomaxillary suture line (Daniel and Landon 1997; Cook et al. 2001) (Fig. 3.8). After its origin, the muscle travels superiorly, toward the glabellar area, for 4–5 mm in the subcutaneous tissue. Its fibers are more vertically oriented than those of the corrugator. At its anterior side, the muscle comes in contact with the angular vessels. Cook et al. (2001) observed that the depressor supercilii appears to originate from two distinct heads in half of the cases studied. The two heads of the depressor supercilii muscle are located superiorly, while the angular vessels pass between them and merge before inserting in the dermis. The muscle fibers insert in the dermis near the medial eyebrow, at a point approximately 13–15 mm superior to the medial canthal tendon (Cook et al. 2001). The dermal insertion of depressor supercilii lies a few millimeters medial to the dermal insertion of the oblique head of the corrugator supercilii muscle (Knize 2000, 2001).
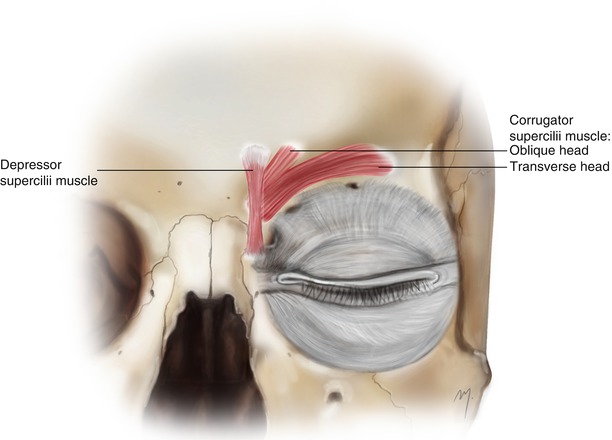
Fig. 3.8
The depressor supercilii and the corrugator muscles constituting the intermediate and the deep muscle layer of the forehead muscles, respectively
The depressor supercilii receives innervation from the angular nerve. It depresses the medial brow belonging to the depressor muscle group for the medial eyebrow.
3.1.2.2.5 Corrugator Supercilii Muscle
The corrugator supercilii muscle is comprised of two muscle bands (heads) that lie below the upper border of the superciliary arch and are located beneath the eyebrow. The corrugator muscle lies deep in the frontalis and orbicularis oculi muscles composing the deep muscular layer of the forehead (Fig. 3.8). It arises from the frontal bone at the superomedial orbital rim, slightly cranially to the trochlea. The origin has a wide base, with an average width of 10 mm being also 10 mm above the medial canthus. After arising from its origin, the muscle divides into its two heads, the small oblique head and the large transverse. The average thickness of the transverse head is 7.5 mm, while the oblique head 2 mm (Walden et al. 2005).
The small oblique head is situated underneath the depressor supercilii muscle. Its fibers run superiorly, parallel to the fibers of the depressor supercilii, across the glabellar region. After a short distance and interdigitation with neighboring muscle fibers of orbicularis and frontalis, it inserts in the dermis along the medial brow at a point approximately few mm, lateral to the insertion of the depressor supercilii muscle. A clear discrimination of the oblique head of the corrugator is not always possible, because occasionally, after its origin, its muscle fibers quickly parallel with the fibers of the larger transverse head (Janis et al. 2007).
The large transverse head passes laterally and slightly upward along the superior orbital rim and runs for about 3.5–4 cm lateral to the midline. The muscle lies beneath the orbicularis muscle, within the galea fat pad, between the layers of the deep galea plane. On the way to its dermal insertion, it becomes more superficial, piercing the frontalis and orbicularis oculi muscles (Knize 1996a, b).
The muscle fibers of the corrugator pierce and interdigitate with the fibers of the frontalis and orbicularis oculi muscles. The fibers of the transverse head usually insert into the deep surface of the middle eyebrow skin although more lateral extension has also been described (Isse and Elahi 2001). The fibers of the oblique head insert into the deep surface of the medial part of the eyebrow.
Corrugator supercilii has a dual nerve supply from both the frontal branch of the facial nerve and the angular nerve. The transverse head is innervated from the terminal branches of the frontal branch of the facial nerve. The oblique head receives its nerve supply from the angular nerve (Caminer et al. 2006). The angular nerve passes in front of the medial canthus reaching the muscle inferiorly.
The corrugator muscle is a brow depressor, which cooperates with the orbicularis oculi to draw the eyebrows medially and inferiorly (frowning, shielding the eyes in sunlight). The combined action of the two muscles produces vertical glabellar wrinkles.
This muscle is resected in forehead rejuvenation procedures and surgical treatment of migraine headaches.
3.1.3 Loose Areolar Tissue
The loose areolar tissue layer continues from the scalp to the forehead as the same subgaleal space, connecting the galea aponeurotica with the forehead pericranium. It also continues laterally at the temporal area as already examined, situated below the temporoparietal fascia and over the temporalis fascia. It receives blood from all the major forehead vessels due numerous tiny branches. The supraorbital and supratrochlear neurovascular bundles traverse this space within the supraorbital margin. Although this subgaleal space is vascular (as in the scalp) an effortless injection of a vasoconstrictive solution transforms it to an avascular dissection plane. Also here the areolar space is of great importance in forehead surgery because it can be easily dissected, creating a surgical dissection plane for large forehead flaps or allowing combined scalp-forehead flaps to be raised at the same plane.
3.1.4 Forehead Periosteum
The periosteum of the forehead is the same dense connective tissue layer over the frontal bone, which as pericranium covers the entire skull. In the frontal area, it is slightly thinner than in the other skull parts. It is loosely adherent to the outer surface of the frontal bone and lies just beneath the loose areolar layer. It becomes densely adherent to the bone over a transverse, 2.5 cm wide area, just above the orbital rims, and in a 6 mm wide band, medial to the superior temporal line (Knize 1996a, b, 2001).
Anteriorly, the periosteum becomes continuous with the periorbita (the inner lining of the orbital bones) at the orbital rims. The transition between the outer periosteum and the inner periorbita of the orbit is known as the arcus marginalis, a thickened connective tissue layer densely adherent almost to the entire orbital rim. Along the supraorbital rim at the arcus marginalis, the periosteum merges with the orbital septum (Zide and Jelks 1985).
At the forehead, Sullivan et al. (2006) described the presence of four retaining ligaments located around the orbit: an inferomedial (just medial to the supraorbital notch), a superomedial (13 mm lateral to the midline and 11 mm above the supraorbital rim), a superolateral (23 mm lateral to the midline and 10 mm above the rim), and a broad lateral one across the lateral aspect of the supraorbital rim.
3.2 Arterial Anatomy
The forehead arterial system consists of a latticework of anastomoses mainly supplied from three pairs of arteries. These arteries are the supraorbital and the supratrochlear arteries and the frontal branches of the superficial temporal arteries. Additionally, the dorsal nasal artery (although anatomically belongs to the nasal arteries) contributes to the blood supply of the mid-forehead area.
The supraorbital and the supratrochlear arteries constitute facial branches of the ophthalmic artery.
3.2.1 Ophthalmic Artery
The ophthalmic artery arises from the cerebral part of the internal carotid artery (rarely it arises from the middle meningeal artery). After entering the orbit, through the optic canal, it gives off many small branches (posterior ciliary artery, muscular branches) and one large branch (the lacrimal artery) to the contents of the orbit.
The lacrimal artery runs forward at the junction of orbital roof and lateral wall and supplies the lacrimal gland. It is then distributed to the eyelids and conjunctiva. Terminal branches of the lacrimal artery are branched as superior and inferolateral palpebral arteries. They anastomose with the medial palpebral arteries. Within the orbit, the lacrimal artery gives also rise to the zygomatic artery, which subdivides further into the zygomaticofacial and the zygomaticotemporal arteries. In 1 %, the lacrimal artery rises from the middle meningeal artery via the superior orbital fissure, and in 2 % it arises from an abnormal ophthalmic artery.
Continuing its course, the ophthalmic artery passes over (or sometimes under) the optic nerve and gives off the supraorbital artery. It then reaches the medial orbital wall, in an anterior direction, below the superior oblique muscle, and gives off the anterior and posterior ethmoidal arteries. Anteriorly to the trochlea, the medial palpebral arteries arise, and the ophthalmic artery divides into its two terminal branches, the supratrochlear artery and the dorsal nasal artery.
The supratrochlear, supraorbital, lacrimal, medial palpebral, and dorsal nasal arteries are the branches of the ophthalmic artery that supply the face.
3.2.2 Supraorbital Artery
The supraorbital artery, after arising from the ophthalmic artery, runs anteriorly, between the orbital roof and levator palpebrae superioris and in company of the supraorbital nerve. The supraorbital artery is slightly wider than the supratrochlear artery. Its mean diameter ranges from 0.84 to 0.87 mm (Erdogmus and Govsa 2007).
It exits the orbit (Fig. 3.9), through the supraorbital notch or foramen, together with the supraorbital nerve and supraorbital vein, which lies anterior to the artery. In 13 % of cases, the supraorbital artery and the supratrochlear artery exit the orbit as a single vessel and separate immediately after exiting from the foramen (notch) (Erdogmus and Govsa 2007).
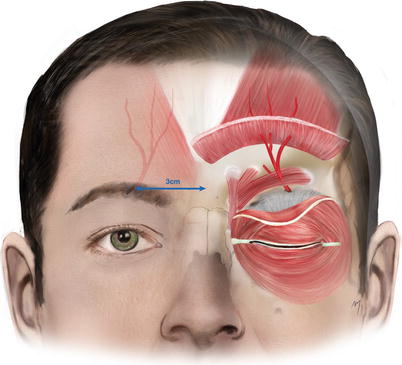
Fig. 3.9
Exit point of the supraorbital artery and the course of its superficial branch
3.2.2.1 Supraorbital Notch (Foramen)
The supraorbital notch (foramen) is situated approximately 2.5–3 cm from the midline (Webster et al. 1986; Miller et al. 2000; Park et al. 2003). Bilateral notches are present more often (60–90 %) than bilateral foramina (Webster et al. 1986; Chung et al 1995; Saylam et al. 2003; Cuzalina and Holmes 2005). Rarely, one notch may be found on one side and one foramen on the other side. The foramen often represents the exit of a small supraorbital canal from where the neurovascular bundle passes from the orbit to the forehead. When a foramen is present, it is located and usually palpated up to 15 mm in relation to the supraorbital rim. In cases where palpability is questionable, an additional landmark can be used; the vertical location of the foramen is situated approximately on the midpupillary line. Great diversity and variants of these notches (foramina) exist from one individual to the other due to sex and race differences (Chung et al. 1995; Kimura 1977; Cheng et al. 2006; Agthong et al. 2005; Jeong et al. 2010; Chrcanovic et al. 2011). In cases where a supraorbital notch is present, it transforms into a “foramen” by a ligament (supraorbital ligament).
The supraorbital artery continues running over the supraorbital rim slightly from medial to lateral and enters the corrugator muscle where it divides into a superficial branch, which supplies the superficial layers of the scalp, and a deep branch supplying the pericranium. The division of the supraorbital artery in 80–90 % of individuals happens at the level of the supraorbital rim or below. In the remainder, division occurs approximately 8.5 mm above the orbital rim (Yoshioka and Kishimoto 1991; Yoshioka and Rhoton 2005).
3.2.2.2 Superficial Branch of the Supraorbital Artery
The superficial branch of the supraorbital artery (Fig. 3.9) enters the corrugator, the orbicularis oculi, and the lowest part of the frontalis muscle, traveling for a short distance within these muscles and divides into 2–4 subbranches. In a distance approximately 2–3 cm above the supraorbital rim, they pierce the frontalis muscle and the galea, becoming more superficial, and travel within the subcutaneous tissue layer.
The superficial branch of the supraorbital artery does not have as long a course as the accompanying supraorbital nerve.
3.2.2.3 Deep Branch of the Supraorbital Artery
After dividing from the main trunk, the deep branch (Fig. 3.10) gives off 2–4 branches, with a mean diameter of 0.6 mm (Yoshioka and Rhoton 2005). These branches run axially as independent tiny vessels above the pericranium within the loose areolar tissue layer, for a distance of about 1.5–4 cm (Erdogmus and Govsa 2007).
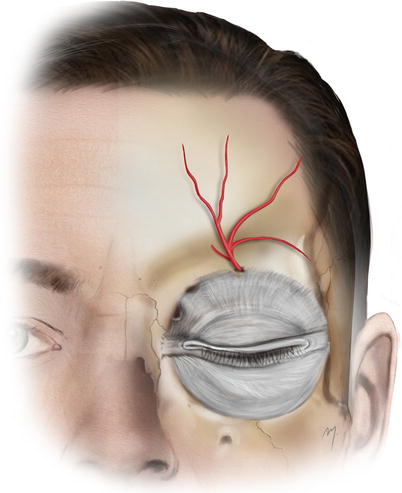
Fig. 3.10
Deep branch of the supraorbital artery
Kleintjes (2007) demonstrated a detailed branching pattern of the deep supraorbital artery. According to his study, three branches usually exist: vertical branches, which run anteriorly and almost parallel; the oblique branch running anterolaterally over the periosteum, which anastomoses with the frontal branch of the superficial temporal artery; and the horizontal branch which runs laterally and above the orbital rim.
One vessel of the deep branches supplies the diploe of the frontal bone and the mucoperiosteum of the frontal sinus (Cormack and Lamberty 1994).
Both branches of the supraorbital artery supply the skin and the muscles of the upper eyelid, the forehead and scalp, the diploe and the periosteum of the frontal bone, and the mucous membrane of the frontal sinus.
3.2.3 Supratrochlear Artery
The supratrochlear artery, after having divided from the ophthalmic artery, runs in the superomedial orbit to the orbital rim. It is usually the largest terminal branch measuring about 0.8 mm in diameter.
It exits the orbit (Fig. 3.11) approximately 2 cm from the midline through the supratrochlear notch, piercing the orbital septum, together with the supratrochlear nerve and vein. At this point, occasionally the artery bends sharply before getting under the muscles. In a small percentage (13 %), the supratrochlear and supraorbital arteries exit the orbit as a single vessel as mentioned above (Erdogmus and Govsa 2007).
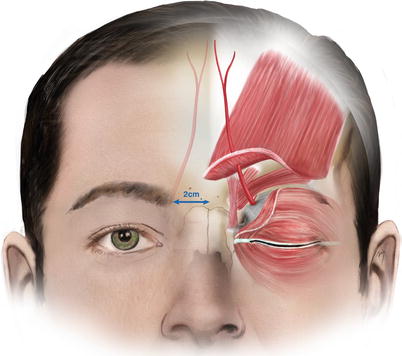
Fig. 3.11
Exit point of the supratrochlear artery and the course of its superficial branch
3.2.3.1 Supratrochlear Notch
Medial to supraorbital notch/foramen lies a small notch, the supratrochlear notch, which represents the point where the supratrochlear nerve and artery exit the orbit. In about 2 %, this exit point is present not as a notch, but as foramen, known as the supratrochlear foramen. The supratrochlear notch is located approximately 2 cm lateral to the midline of the forehead and medial to the supraorbital notch/foramen.
3.2.3.2 Superficial Branch of the Supratrochlear Artery
The superficial branch (Fig. 3.11) initially lies over the corrugator muscle and deep to orbicularis and the lower part of frontalis muscle. Approximately 1.5 cm above the supraorbital rim, it pierces the muscles and becomes subcutaneous. From this point, it runs superiorly and slightly medially in the subcutaneous plane. The superficial branch travels for about 7–10 cm above the supraorbital rim. When terminating its course, axial final branches sometimes slightly extend beyond midline while starting to communicate with the contralaterals.
3.2.3.3 Deep Branch of the Supratrochlear Artery
The deep branch of the supratrochlear artery, being its periosteal branch, continues on the periosteum for at least 3–4 cm (Fig. 3.12).
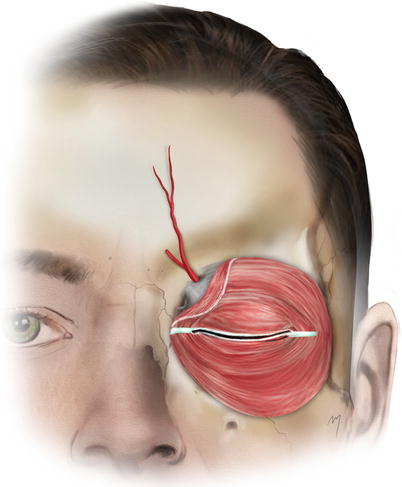
Fig. 3.12
Deep branch of the supratrochlear artery
The supratrochlear artery, by both of its branches, supplies the central forehead skin, the forehead muscles, and the pericranium of the central forehead.
3.2.4 Frontal Branch of the Superficial Temporal Artery (Terminal Part)
The frontal branch of the superficial temporal artery after originating from the bifurcation of the superficial temporal artery runs at the temple tortuously upward and forward.
As it enters the forehead (Fig. 3.13), it usually gives a transverse branch, as the main continuation ascends superomedially. Its final part reaches the forehead at the inferior or middle forehead level, at the orbital rim vertical line (Kleintjes 2007). The artery travels superficially to the frontalis muscle, becoming shallow up to the subdermal level as it approaches the midline. The frontal branch is the main vascular supply for the temporal subunits of the forehead.
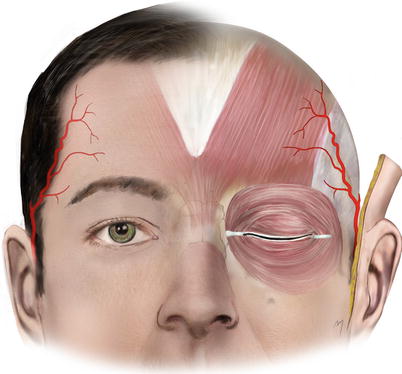
Fig. 3.13
Frontal branch of the superficial temporal artery
3.2.5 Glabellar Branch of the Dorsal Nasal Artery
The dorsal nasal artery (see Chap. 4) contributes in the forehead vascular supply by a superior glabellar branch (Fig. 3.14). The glabellar branch arises from the dorsal nasal artery, after its exit from the orbit, and extends cephalad to the glabella or even up to the inferior central forehead. This branch supplies the skin and periosteum of glabella and anastomoses with the supratrochlear artery and its contralateral. The dorsal nasal artery also gives off, from its initial part, small deep ascending branches that supply the glabellar periosteum. The superior branch of the dorsal nasal artery anastomoses with the supratrochlear artery and its contralateral.
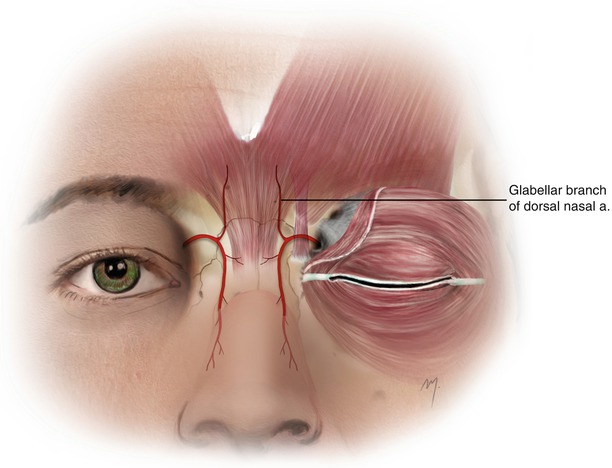
Fig. 3.14
Glabellar branch of the dorsal nasal artery
3.3 Venous Drainage
The venous anatomy of the forehead exhibits significant variations, and the following description regatds those being relatively more constant (Fig. 3.15).
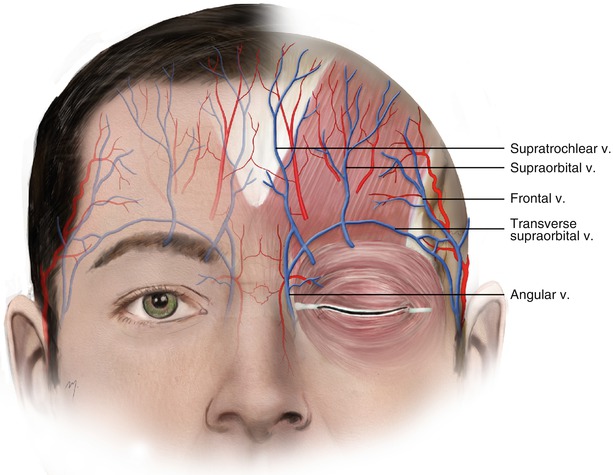
Fig. 3.15
The veins of the forehead
Venous drainage of forehead starts from a rich venous plexus that extends wide from the forehead to scalp. Small veins converge, forming gradually larger venous trunks. These trunks found in the middle forehead are the supratrochlear vein and the supraorbital vein, and in the lateral forehead the frontal vein.
3.3.1 Supratrochlear Vein
The supratrochlear vein starts from the venous plexus, near the forehead midline, and descends to the root of the nose, parallel with its contralateral. Across the nose, the two supratrochlear veins are connected with the transverse nasal arch, a small vein that drains the dorsum of the nose in this area and the glabella. It then divides, and one branch penetrates the orbital septum and enters the orbit through the supratrochlear notch, while the other subdivision joins the supraorbital vein near the medial canthus to form the angular vein.
The supratrochlear vein runs a course parallel and medially to its artery, but a distance between them exists that sometimes can range up to 10 mm. This is very important when designing paramedian forehead flaps. To ensure catching both artery and vein into the flap, the width, especially in its base, should not be narrower than 1.5–2.0 cm.
3.3.2 Supraorbital Vein
The supraorbital vein starts from the forehead venous plexus and descends to the supraorbital rim accompanying the supraorbital artery. Before entering the orbit through the supraorbital notch (foramen), it divides, and one branch runs medially to join the supratrochlear vein and form the angular vein. The intraorbital branch along with the intraorbital branch of the supratrochlear vein forms the superior ophthalmic vein that runs to the cavernous sinus.
The supraorbital vein is connected to the frontal branch of the superficial temporal and the middle temporal veins, through a transverse venous trunk, the transverse supraorbital vein. This venous arch courses in about 60 %, at the level of the supraorbital rim. The remaining 40 % lies approximately 9 mm above it (Erdogmus and Govsa 2007). This limb of venous drainage of the frontal region has the best chance of being preserved, with the condition that the dissection of the galea frontalis layer from the pericranium does not extend into 10–15 mm above the supraorbital rim (Yoshioka and Rhoton 2005).
3.3.3 Frontal Vein
The frontal vein starts from the converged veins of the frontolateral venous scalp plexus. Above the zygomatic arch, it joins with the parietal vein and forms the superficial temporal vein. The frontal branch of the superficial temporal vein is also connected to the supraorbital artery through the transverse supraorbital vein.
3.4 Nerves
Sensory innervation of the forehead and anterior scalp is supplied by the supraorbital and supratrochlear nerves, which are branches of the frontal nerve.
The frontal nerve is the largest branch of the ophthalmic division (V1) of the trigeminal nerve. It enters the orbit through the superior orbital fissure above the annulus of Zinn and runs forward between the levator palpebrae superioris muscle and the periorbita. About halfway between the apex and the orbital rim, it divides into its terminal branches, the small supratrochlear and the large supraorbital nerve. The motor nerve that is encountered to the forehead is the frontal branch of the facial nerve.
3.4.1 Supraorbital Nerve
After arising from the frontal nerve, the supraorbital nerve runs forward nearly to the midline of the orbit. It exits the orbit through the supraorbital notch (foramen) (Fig. 3.16). This point is marked grossly on the orbital rim at the junction of the medial and middle thirds of the supraorbital margin and as mentioned approximately 2.5–3 cm lateral to the midline. Sometimes the supraorbital nerve can leave the orbit with several branches through separate periosteal canals (Fatah 1991). In an extensive anatomic study of 1014 orbits, Beer et al. (1998) concluded that “(1) the exit point(s) of the supraorbital nerve are not at all constant; (2) the supraorbital nerve leaves the orbital rim either undivided or in its two branches via two separate exit points; (3) the exit point(s) can be either a notch or a foramen; (4) the exit point(s) can be located along the whole orbital rim and even laterally of it; and (5) the exit point(s) can be significantly cephalad to the orbital rim.” Due to these numerous variations and despite the mentioned supraorbital notch/foramen landmarks, it is very important when dissecting in this area during forehead or brow surgery to identify the notch (foramen) under vision in order to avoid nerve injury.
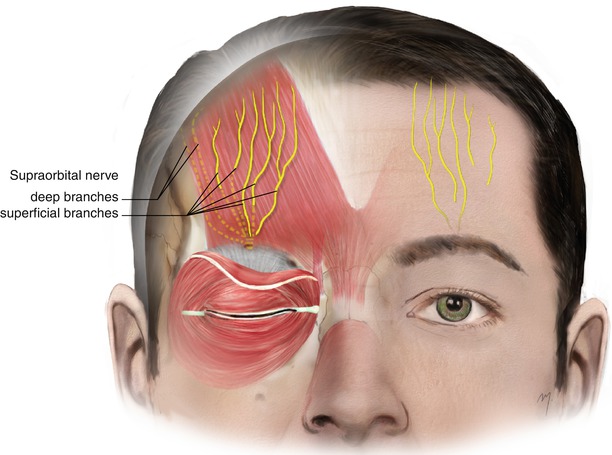
Fig. 3.16
The supraorbital nerve entering the forehead divides into its superficial and its deep branches
As the supraorbital nerve exits the orbit, it gives off small palpebral filaments to the upper eyelid and conjunctiva. Also, small branches supply the mucous membrane of the frontal sinus entering it through foramina in the floor of the supraorbital notch (foramen). After leaving the orbit, the supraorbital nerve trunk divides into a large, lateral deep branch and a smaller, medial superficial branch (Fig. 3.16). In 15 %, the supraorbital nerve leaves the orbital cavity already having those two branches (Beer et al. 1998). A variation to the above, is that the lateral deep branch exits the orbit from a separate foramen, located up to 1.5 cm, cephalad to the supraorbital notch (Erdogmus and Govsa 2007; Keller and Mashkevich 2009). Initially, these branches lie in the submuscular plane, deep to the orbicularis, frontalis, and corrugator supercilii muscles, in close approximation to the periosteum of the supraorbital ridge, in a position respectively in the middle third of the corrugator.
3.4.1.1 Superficial Branch of the Supraorbital Nerve
The superficial branch of supraorbital nerve quickly divides into multiple smaller branches. As they ascend, they pass through the corrugator supercilii and frontalis muscle, becoming more superficial. In 22 %, branching occurs more cephalad, close to the superior margin of the corrugator muscle (Janis et al. 2008). After perforating the frontalis muscle at various points from the orbital rim to the mid-forehead level, they run over its surface, along with the supratrochlear nerve branches, reaching and traveling into the subcutaneous plane. These smaller branches form a wide fan pattern, before entering the frontal scalp (Knize 1995). The length of the medial branches has been reported to be from 1.5 to 11.7 cm (Malet et al. 1997; Erdogmus and Govsa 2007; Andersen et al. 2001).
According to their length, they supply sensation to the forehead skin and to the frontal scalp in various ranges.
3.4.1.2 Deep Branch of the Supraorbital Nerve
The deep branch of the supraorbital nerve exits the orbit as one branch in 34 %, as two branches in 60 % and in the remaining 6 % of cases, as multiple branches (Knize 2001; Erdogmus and Govsa 2007). The one or two branches (being parallel each other) at first run laterally, above the periosteum and along the orbital rim or occasionally up to 1.5 cm superior to the rim. At the level of the lateral third of the eyebrow, they turn cephalad. After turning cephalad, the deep branch (single or double) runs in a superolateral direction, parallel and 0.5–1.5 cm medial to the superior temporal line (Knize 1995). It courses in the loose areolar tissue, beneath the frontalis muscle and the galea, and above the pericranium and gives off very small branches, which innervate the periosteum. In the cases where the deep branch presents two branches, one is larger than the other, and together they run without any further branching (Erdogmus and Govsa 2007). At the level of the hairline, near the coronal suture, it turns medially and pierces the galea becoming more superficial and then divides to its terminal rami (Knize 1995). The deep branch is longer than the superficial with a length ranging from 35 to 145 mm (Malet et al. 1997; Andersen et al. 2001). These branches supply scalp sensation to the frontoparietal region occasionally reaching the vertex of the skull.
The presence of a small, horizontal, additional branch of the deep branch of the supraorbital nerve has recently been described (Vestal et al. 1994; Hwang et al. 2005; Janis et al. 2008). This horizontal branch exits the supraorbital foramen (notch) as 1–2 rami. It runs upward about 10 mm and turns laterally parallel to the supraorbital rim, along the undersurface of the corrugator muscle, ending at the end of the brow. It supplies sensation in a skin area of 3 cm at the lateral mid of the eyebrow. In approximately half of individuals, this horizontal branch anastomoses with the temporal branch of the facial nerve (Hwang et al. 2005).
Both of the branches of the supraorbital nerve supply sensation to the skin of the lateral forehead, the anterior scalp, the frontoparietal scalp, the mucous membrane of the frontal sinus, and the pericranium of the forehead and anterior scalp region.
3.4.2 Supratrochlear Nerve
The supratrochlear nerve is smaller than the nearby supraorbital nerve. After dividing from the frontal nerve, it courses anteromedially in the roof of the orbit, passes above the trochlea of the oblique superior muscle, and gives off a descending filament to join the infratrochlear branch of the nasociliary nerve.
It exits the orbit at the superior orbital rim, between the trochlea and the supraorbital foramen through the supratrochlear notch (Fig. 3.17). At the supraorbital rim, it first pierces the orbital septum; then curves up on to the forehead close to the bone, in company with the supratrochlear artery; and ascends at first beneath and through the corrugator supercilii muscle. Within the corrugator muscle, the supratrochlear nerve divides into one to three branches. These branches as they run upward, these branches become more superficial, piercing the corrugator and frontalis muscle, and then enter the subcutaneous tissue of the central forehead. The terminal branches never cross the midline. The length of the supratrochlear nerve ranges between 23 and 70 mm (Andersen et al. 2001).
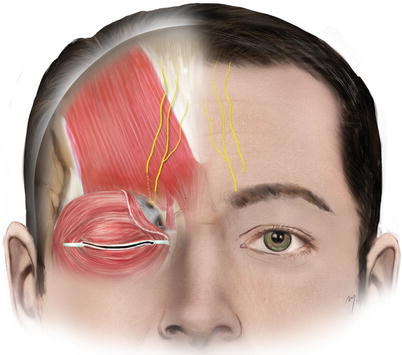
Fig. 3.17
Supratrochlear nerve
The supratrochlear nerve supplies cutaneous sensation to a central vertical strip of forehead and to the medial one-third of the upper eyelid skin and conjunctiva. There is an overlap of the supratrochlear nerve sensory area by the sensory area of the superficial division of the supraorbital nerve.
3.4.3 Forehead Regional Anesthesia
A great number of small to medium lesions at the forehead can be excised, and minor flap reconstruction is achieved by a forehead block. The supraorbital nerve is blocked by its exit from supraorbital foramen (notch). The foramen (notch) is palpated at the supraorbital rim, and if this is unclear, its quite possible position 2.5–3 cm lateral to the midline is marked. At this point, about 1 ml of local anesthetic solution is injected just above the bone (Fig. 3.18). Direct injection within the foramen must be avoided because it may result in nerve damage. The supratrochlear nerve is blocked by infiltrating the same amount of local anesthetic solution along the supraorbital rim, 2 cm lateral to the midline or 1 cm medial to the previous point (Fig. 3.19). By blocking both nerves, complete anesthesia of the hemiforehead is achieved.


Fig. 3.18
Supraorbital nerve block
Fig. 3.19
Supratrochlear nerve block
3.4.4 Frontal Branch of the Facial Nerve
At the forehead, the frontal branch of the facial nerve is present due to its final part (Fig. 3.20). As the frontal nerve comes from the temple, it reaches the forehead 1.0–1.5 cm above the lateral extremity of the brows. Situated at the temple along the undersurface of the temporoparietal fascia as it reaches the lateral border of the frontalis muscle, it pierces the fascia and continues to the undersurface of the frontalis muscle providing its innervation. A tiny ramus that runs medially to innervate the transverse head of the corrugator muscle has been found in 60 % of the individuals (Tzafetta and Terzis 2010).
Fig. 3.20
Frontal branch of the facial nerve at the forehead
3.5 Flaps Derived from the Forehead
The forehead constitutes a wide donor site of flap material that can be harvested in great quantity. Flaps derived from the forehead can be used in closing its own defects, but the forehead is also the ideal donor site of regional flaps in order to reconstruct medium and large nasal defects. In the past, the robust forehead flaps have been used also for cheek reconstruction, nowadays abandoned due to better reconstructive solutions.
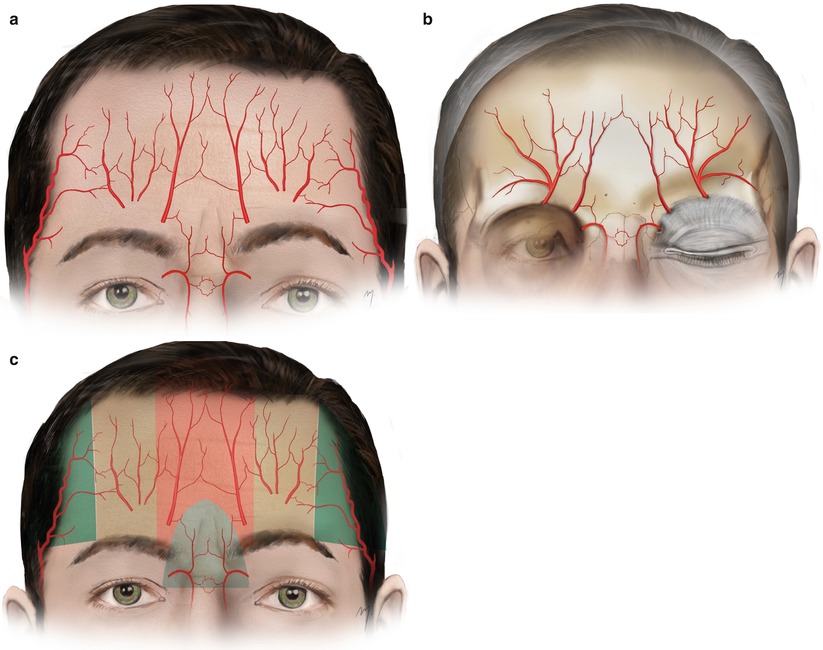
3.5.1 Flap Design Concerning Vascular Anatomy
The supratrochlear, supraorbital, dorsal nasal, and frontal branches of the superficial temporal artery anastomose each other, forming a rich superficial (Fig. 3.21a) and deep arterial network (Fig. 3.21b), in the following way.