- •
Tumescent liposuction was developed and continues to be widely practiced by dermatologic surgeons
- •
The tumescent local anesthesia offers significant safety benefits over general anesthesia
- •
Ultrasonic liposuction may increase the risk of seroma, thermal burns, and necrosis, and consequently should be used with caution
- •
Powered liposuction, using a reciprocating cannula, increases the rate of fat removal, improves patient recovery, and decreases the physician’s physical strain
The history of liposuction
The history of modern liposuction dates to 1976 when Fischer described the use of hollow cannulas to remove subcutaneous fat. Due to the efforts of Fischer, as well as Ilouz and Fournier, cannulas evolved to blunt tipped instruments containing motor driven blades. Ilouz developed the ‘wet technique’ in which hypotonic saline and hyaluronidase were infiltrated into the subcutaneous tissue prior to suction to achieve anesthesia and mobilize the fat from fibrous attachments. In contrast, Fournier introduced the ‘criss-cross’ technique that allowed for overlapping and intersecting tunnels in the subcutis designed to effect uniform fat reduction.
The early liposuction cannulas were 8–10 mm in diameter. With experience, surgeons learned that smaller caliber cannulas were sufficient to remove fat. Smaller cannulas were also beneficial in that they were less likely to damage neurovascular bundles or cause seromas and hematomas. Smaller cannulas allowed for more precise and even contour sculpting, and overall improved aesthetic outcomes. Cannulas today remain small (2–5 mm), with some having an inside diameter of less than 1 mm.
In 1987, Klein introduced the concept of liposuction using ‘tumescent technique’. Prior to that time, general anesthesia was required to perform liposuction. Tumescent technique has been refined over time, and is now commonly referred to as tumescent local anesthesia (TLA). TLA improved liposuction safety and markedly decreased intraoperative blood loss, thus reducing the overall morbidity associated with liposuction to a negligible level. In the 1980s and early 1990s, numerous American dermatologists adopted TLA and published large studies confirming the superior safety profile of the technique.
Tumescent anesthesia is a multistage process. Initially, early infiltration provides partial anesthesia which can then be maximized to full tumescence prior to the start of liposuction. Additional ‘topping off’ of anesthesia may be performed immediately before suctioning or during suctioning, if areas are revealed to have inadequate anesthesia.
The increased adoption of TLA stimulated interest in liposuction and consequently led to the development of adjuvant technologies. In 1988, Zocchi introduced the use of ultrasound-assisted liposuction. Ultrasound-assisted liposuction was met with initial enthusiasm, but unfortunately it was quickly recognized that ultrasound energy delivered into the subcutaneous fat compartment cannot infrequently be associated with complications. In the mid-1990s, powered liposuction, using electric reciprocating cannulas, was introduced. Powered liposuction increased the efficiency of tumescent liposuction while maintaining the overall safety of the procedure and hence has been widely adopted.
Patient selection
Liposuction is designed for individuals at or near their ideal body weight who want to reduce single or multiple local accumulations of excess fat. Liposuction is not a weight loss technique. It is important to discuss risks, benefits, and expectations during the initial consultation.
Preoperative evaluation
Performing a thorough preoperative evaluation is essential to maximize the likelihood of patient safety and optimal results. Review of all the patient’s medications may reveal medically necessary anticoagulation, which is generally considered a relative contraindication. Medications that thin the blood but are not medically necessary, such a fish oil, nonsteroidal anti-inflammatory drugs, and vitamin E, should be stopped for at least 2 weeks prior to the procedure. Medications that interact with cytochrome P450 3A4 decrease the liver metabolism of lidocaine and consequently could increase toxicity. If possible, these medications should also be stopped at least 2 weeks prior to the liposuction procedure. Preoperative laboratory workup routinely includes complete blood count with differential and platelet count, prothrombin time, partial thromboplastin time, comprehensive chemistry panel, human immunodeficiency virus serology, and hepatitis B and C. An electrocardiogram may be performed for patients over the age of 50.
Once the patient is ready for liposuction, the area to be treated is typically marked and photographed, with specialized symbols used to indicate areas of greater fat accumulation, areas of low fat density to be avoided during liposuction, and areas at the periphery of the target area that are to be lightly suctioned to avoid an abrupt step-off shelf, or ‘feathered.’ The patient is then prepped under sterile conditions and the remainder of the procedure is performed clean or sterile. Oral anxiolysis such as medium-duration benzodiazepines (e.g. diazepam) may not only help the patient better cope emotionally with the mild procedure-associated discomfort but also directly relax abdominal and other musculature to facilitate lidocaine infiltration and suctioning.
Anesthesia
TLA is based on a lidocaine solution in which normal saline is used as the diluent. Sodium bicarbonate 8.4% is added to buffer the solution, with 10 mL of sodium bicarbonate 8.4% usually mixed in per 1000 mL of normal saline. In order to induce vasoconstriction, which facilitates hemostasis and decreases the rate of absorption of the lidocaine, 1 mL of epinephrine 1 : 1000 is added per 1000 mL of normal saline. The concentration of lidocaine in TLA is normally between 0.05% and 0.1%. New studies have demonstrated adequate anesthesia with lidocaine concentrations as low as 0.04–0.05%, but more sensitive sites with greater sensory innervations may require slightly higher concentrations. The total volume of tumescent solution is usually kept at a level not exceeding 55 mg/kg, which is a dose level that is known to be safe.
Entry sites are prepared by intradermal infiltration using full strength lidocaine solution, such as 1% lidocaine with 1 : 100 000 epinephrine. Incisions for cannula entry sites are typically made with a No. 11 blade or a 2 mm punch biopsy device. A blunt tipped infiltration cannula or a medium diameter needle (e.g. 18–22 gauge) is inserted, and the TLA solution is delivered into the subcutaneous space using an infiltration pump. After approximately 20–60 minutes, the epinephrine should reach maximum vasoconstrictive effect with maximal intercellular diffusion.
Keeping the patient warm during the liposuction procedure may improve patient comfort.
Operative technique
The suction cannula is inserted vertically, redirected to the horizontal plane, and then repositioned so that the cannula aperture is facing downwards, away from the overlying dermis. Tunneling with the cannula is conducted using meticulous, linear strokes, in a fan-like pattern radiating circumferentially from the incision point. Long strokes that comprise almost the entire length of the cannula should be used so that fat is removed consistently and evenly, and small areas are not oversuctioned so as to create indentations. The nondominant hand, or ‘smart hand’, may be placed on the skin overlying the cannula tip to monitor the cannula position. The use of multiple entry sites facilitates a criss-cross pattern to optimize contour. Suction should be parallel to the axis of lymphatic drainage to minimize tissue trauma. To stabilize the tissue, use of MASST, manually assisted skin stabilization technique, is helpful. In this technique, an assistant stretches the skin providing traction on the skin surface. Operating technique varies according to surgeon and anatomic region.
Whenever possible, the cannula should be directed parallel to the long axis of the body to minimize lymphatic, nerve and blood vessel damage.
Manually assisted skin stabilization technique, or MASST, is a helpful way to stabilize the skin during liposuction. Using this technique, an assistant stretches the skin providing traction on the skin surface.
Liposuction of the neck and jowls is an effective treatment to remove submental fat, which is often hereditary. Initial markings may identify key anatomic structures, so that liposuction can be appropriately targeted and danger zones, such as the point at which the marginal mandibular nerve courses over the mandibular rim, can be avoided. Patients can be positioned supine with the head extended. TLA commences with infiltration of a small (100–150 mL) volume of anesthesia to establish numbness. Further infiltration is then typically continued until tumescence is achieved, and, in some cases, additional infiltration, so-called ‘topping off’, may be used to add yet more tumescence before suction begins. Short cannulas with a diameter of 1.5–3 mm are commonly used.
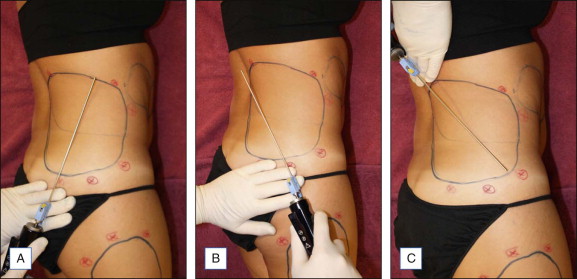
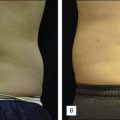
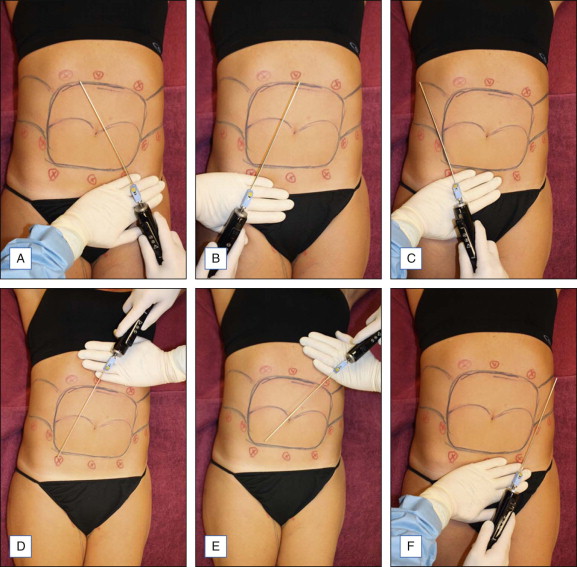
The abdomen is the most common site of body liposuction. It is important to identify which areas within the abdomen require suction. Individuals with focal excess adiposity in the lower abdomen respond well to isolated suction of the lower abdomen. However, isolated lower abdominal suction in patients with more diffuse fatty deposition can result in an overhanging upper abdomen, and so typically both lower and upper abdomens are suctioned concurrently. Suction may continue to the lateral flank area to avoid an abrupt step-off. Patients are positioned supine ( Fig. 9.1 ) before the procedure begins. Typically five or six entry sites are used, but more may be required. Suction should include the mid-fat and also target deeper fat planes to ensure adequate fat removal while avoiding surface dimpling. Meticulous anesthesia and suctioning around the umbilicus is needed to avoid residual excess fat at this location, and hence a protuberant umbilical area postoperatively.
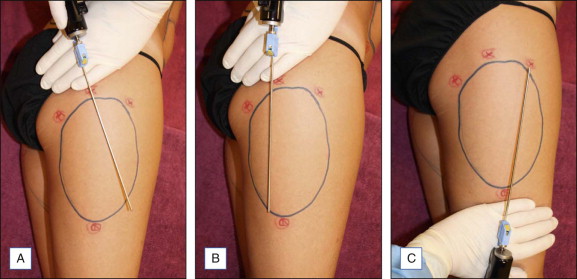
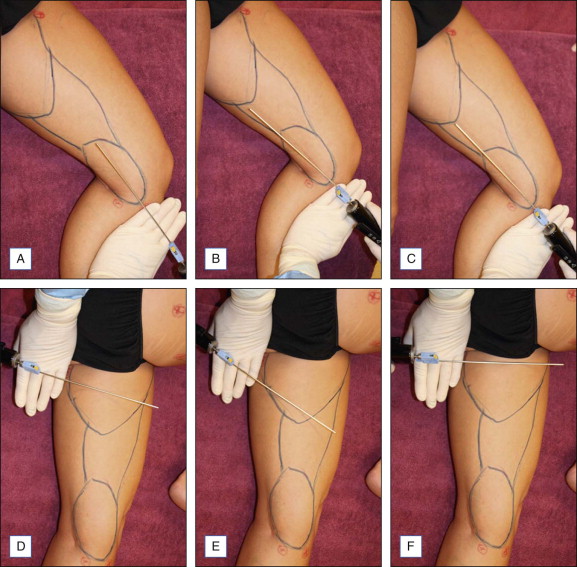
Liposuction of the hips, thighs and buttock requires careful evaluation of the musculature and skin quality on the lower extremities. For the thighs and hips, patients are routinely positioned in the lateral decubitus position ( Figs 9.2–9.4 ). For the buttock, patients tend to be positioned prone. Care should be taken to remove equal amounts of fat from both sides. Oversuctioning will result in an unnatural concave contour.