- •
Radiofrequency and ultrasound devices are at the forefront of medical advances in the treatment of cellulite
- •
Radiofrequency generates heat in the tissue, resulting in shrinkage of collagen fibers, stimulation of new collagen and elastin, and destruction of adipocytes
- •
Ultrasound uses focused sound waves to cause mechanical and thermal damage to the tissue, resulting in lysis of adipocytes, stimulation of collagen and improvement in circulation
- •
Although these devices may provide improvement in the appearance of cellulite, the results are temporary; no lasting improvements have been achieved
- •
Patients who receive the most benefit from these devices often have a moderate amount of cellulite on the buttocks or the thighs, have little skin laxity, maintain a healthy weight, and are capable of returning for a series of treatments
Cellulite
Cellulite is the lay term used to describe puckered or dimpled skin, most often present on the thighs and buttocks of women, and has been termed liposclerosis, gynoid dystrophy, dermopanniculitis, and edematofibrosclerosis in the medical literature. Cellulite is considered a normal physiologic state of secondary sex characteristics in females, 85–98% of whom are affected, regardless of their BMI.
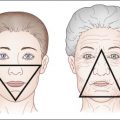
Histologic studies demonstrate that the appearance of cellulite relates to the architecture of the skin and subcutis in affected skin. Fibrous septa in women extend from the dermis to deep fascia in a perpendicular pattern, resembling a mattress or down quilt, in contrast with those of men, where they form a criss-cross pattern. As the fat layer expands, pockets of fat herniate into the reticular and papillary dermis and are fixed in place by the fibrous septa. As the skin thins with age, the herniated fat becomes more evident. The pathophysiology of cellulite is multifactorial and complex. Cellulite is stimulated by estrogens. There is also evidence that cellulite may worsen when the microcirculation and lymphatic drainage are compromised. A more extensive discussion of the pathophysiology of cellulite can be found in Chapter 12 .
Treatments aimed at fat reduction such as liposuction, high intensity focused ultrasound, and cryolipolysis, cannot target fat herniations associated with cellulite because of the risk of necrosis of the thin overlying skin. Many of the invasive and noninvasive therapies developed for cellulite treatment use a combination of modalities designed to correct the architectural and physiologic abnormalities that are thought to contribute to cellulite formation ( Box 15.1 ). These include lysing or evacuating the superficial adipocytes, increasing the metabolic activity of the adipocytes via heat or norepinephrine secretion, decreasing lymphedema, increasing the thickness of the skin by inducing new collagen formation and remodeling, and altering the fibrous septa.
Many of the technologies that will be discussed below lack controlled trials, and those that have been studied often were examined in investigations that have clinical endpoints that are difficult to reproduce, such as circumferential reduction and inconsistent photography. Objective evidence of improvement such as MRI studies is uncommon, and cellulite improvement is often difficult to assess, even with standardized photography.
Radiofrequency
Radiofrequ;ency (RF) has been used in medicine for many years to electrodesiccate, coagulate, and ablate tissue. RF relies on heating of water rather than absorption by tissue chromophores, and hence can be used in any skin type. RF creates an oscillating electrical current which induces collisions between charged ions and molecules in tissue, resulting in the generation of heat. The biologic effects of the tissue heating vary depending on the frequency used, depth of delivery, and selectivity achieved with skin cooling. The depth of penetration of RF is inversely proportional to the frequency, and the relative degree of heating of water or fat will depend on the electric field.
RF treatment of skin produces temporary shrinkage of collagen molecules, and stimulation of new collagen and elastin production. The amount of tissue contraction and remodeling is dependent upon the maximum temperature reached, the length of time that temperature is maintained, and the conductivity and age of the tissue. Collagen remodels and neocollagenesis is induced when the reticular dermis reaches 60–65 °C, which correlates with a surface temperature of 40–42 °C, the target temperature of RF devices. RF can also be used to heat and destroy fat. Heating of adipocytes with RF increases adipocyte apoptosis as well as lipase-mediated enzymatic degradation of triglycerides into free fatty acids and glycerol.
RF may be delivered using monopolar, bipolar, or unipolar devices, alone or in combination with other technologies. With monopolar devices, patients are grounded and the RF is delivered via the skin to the grounding electrode. RF travels best through tissues with high water content and produces the greatest resistance in fat, creating the highest temperature rise. Monopolar RF is delivered in a stamped mode with individual pulses or in a continuous mode, where the handpiece is applied to the skin with constant motion.
Bipolar RF is less deeply penetrating than monopolar RF. The RF travels between two poles (positive to negative), and the distance between the electrodes determines the depth of penetration in tissue, which is typically 1–4 mm. With unipolar RF, there is a single electrode without a grounding pad. The RF is emitted in all directions around the electrode. Unipolar RF uses high-frequency electromagnetic radiation at 40 MHz, not electrical current, to cause oscillation of water molecules to produce heat. The penetration ranges from 15 to 20 mm. Tripolar RF is a variation that uses a combination monopolar and bipolar electrode.
A surface temperature of 40–42 °C must be achieved in order for RF energy to cause an alteration in collagen fibers.
Ultrasound
Ultrasound is a mechanical compression or sound wave that is above the audible range (>20 kHz) and may destroy fat cells by mechanical or thermal mechanisms. Ultrasound is characterized by its frequency in kiloHertz (kHz) or megaHertz (MHz) and intensity in W/cm 2 . Like other electromagnetic radiation, ultrasound travels through tissue and is reflected, absorbed, or scattered. Waves are propagated through tissue causing molecules to oscillate and create energy that is transformed into heat. These repeated movements cause cavitation, which results in mechanical disruption and eventual death of the target cells.
In tissue, ultrasound becomes increasingly attenuated with higher frequencies, resulting in less depth of penetration. Ultrasound is commonly employed for diagnostic purposes, using frequencies in the range of 2–20 MHz. This type of ultrasound, termed ‘nonfocused’, delivers low-energy, diffuse waves that do not produce a sufficient amount of heat in the tissue to cause destruction. For body contouring, fat removal and improvement in cellulite, ultrasound is ‘focused’, with frequencies in the range of 0.8–3.5 MHz. The focused nature of waves allows for energy to be directed at a small region or single point, resulting in heat or mechanical disruption to cause tissue damage. Thus, the subcutaneous fat may be treated, while the critical surrounding structures are left unharmed.
When directing treatment to improving the appearance of cellulite, devices often use a medium-intensity ultrasound. This allows for propagation of the signal to reach the subcutaneous fat, but also provides some spread of energy to the surrounding collagen. Ultrasound energy causes lysis of fat cells, but also stimulates collagen thickening by heating the dermis and improves circulation. Studies have also shown that ultrasound results in breakdown of fat secondary to secretion of norepinephrine from sympathetic nerves.
Patient selection
The prototypical patient has moderate cellulite on the buttocks and thighs. Ideally, the contour abnormalities could be captured with standardized photography. Patients should be prepared to return for a series of treatments within a reasonable timeframe. Their expectations should be managed and they should be educated about the likelihood of delayed improvement.
Contraindications for RF devices include implanted electronic and metal devices, pregnancy, current use of isotretinoin, hip surgery or replacement, treatment over tattoos or permanent makeup/filler, blood dyscrasia or diseases with altered collagen-vascular properties.
Contraindications for ultrasound-based devices include pregnancy (exclusion of any region near the fetus); thrombophlebitis or thromboembolic disease; treatment over the vertebrae; treatment in the thoracic region if a pacemaker is present; treatment around the eye; treatment over bony fractures, metal implants, hip surgery or replacement; and current malignancy (to avoid tissue disruption and unwanted increased spread of malignant cells). Caution should be used when treating over bony prominences or regions with decreased sensitivity.
Side effects
Although infrequent, burns and fat atrophy may occur. Patients need to be properly grounded at all times and the cooling devices must be functioning properly. Fat atrophy is often a result of using energies that are too high or repeatedly treating an area without allowing for cooling. Overall, the safety profiles of these devices are excellent, and, if used properly, they are associated with few side effects or complications.
The use of standardized photography is essential in determining the efficacy of these treatments.
Radiofrequency devices
Monopolar radiofrequency devices
Thermage®
Thermage® (Solta Medical Inc., Hayward, CA) is a monopolar RF device FDA-approved for the noninvasive treatment of rhytides and the temporary improvement in the appearance of cellulite ( Table 15.1 ). The device has a generator, a handpiece with treatment tip, and a cryogen unit. The handpiece is equipped with sensors for skin temperature and pressure, as well as a cooling apparatus. Tip sizes vary depending on the treatment region, with the DC and CL tips used for body contouring and cellulite. The company supplies a temporary grid that may be applied to the patient’s skin in order to provide a systematic treatment approach. Contact gel is spread over the area and, as the handpiece is activated, the epidermis is heated to 40–42 °C. Multiple passes are conducted over the treatment area, though care needs to be taken to allow epidermal cooling between passes.
| Device | Modality |
|---|---|
| Thermage® | Monopolar RF |
| VelaSmooth™ | Bipolar RF |
| VelaShape™ | Bipolar RF |
| Reaction™ | Bipolar RF |
| Accent™ RF System | Unipolar or bipolar RF |
| TriPollar™ | Tripolar RF |
| Venus Freeze™ | Multipolar RF |
| C-Actor® | Ultrasound |
| VASERshape™ | Ultrasound |
| Bella Contour® | Ultrasound |
| UltraShape | Ultrasound |
| Ulthera | Ultrasound |
Mechanism of action
The heat produced by monopolar RF (6 MHz) causes heat damage to collagen and incites the inflammatory cascade that results in a wound healing response. As RF produces volumetric heating, the collagen fibrils quickly shorten, providing the immediate appearance of tightening. The shrinkage is secondary to a breakdown of hydrogen bonds in the collagen chain. Blood flow is also increased which in turn allows for enhanced metabolism of fat. Over weeks to months, neocollagenesis occurs as a result of the wound healing response.
Results
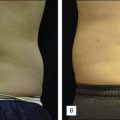
The majority of Thermage studies have been conducted to provide data for improvement of rhytides and facial laxity, with very few concentrating on body contouring and cellulite. Anolik et al. conducted a blinded, multicenter trial using the ThermaCool TC to treat mild to moderate abdominal skin laxity in 12 patients. The protocol used the Thermage Multiplex Tip and most patients received 300 pulses with energies ranging from 28 to 46 J/cm 2 . Of the patients who returned for follow-up, all had a decrease in waist circumference. All but one patient had aesthetic improvement (body contour and skin laxity). Patients received anxiolytics and analgesics before the procedure and side effects included transient edema and erythema, lasting only a few hours.
Zelickson et al. evaluated histologic specimens after Thermage treatment that revealed an increased diameter of collagen fibrils post-treatment. Protein analysis confirmed neocollagenesis by the presence of increased collagen type I mRNA expression.
Side effects using the original system included fat atrophy, erosions, and dysesthesias. As new software and protocols were implemented that use lower-energy, higher-pass treatments, side effects have diminished significantly and patients typically experience only mild erythema and edema.
Exilis
Exilis (BTL Industries, Boston, MA) is an FDA-approved device for treatment of wrinkles and rhytides and is often used off-label for body shaping and skin tightening. The system incorporates monopolar RF with energy flow control (EFC). EFC is an innovative technology that eliminates energy peaks, allowing for a more controlled and constant heating of the tissue. BTL has coined this process as square (‘flat top’) spectrum energy profiling. As the handpiece allows for real-time monitoring of skin temperature and RF energy, the system will shut off if skin temperatures and energies are out of range. Patients usually receive four treatments, 1 week apart. There are no published clinical trials using this device for the treatment of cellulite, but there are anecdotal reports of improvement.
Bipolar radiofrequency devices
VelaSmooth™
VelaSmooth™ (Syneron Medical Ltd, Yokneam, Israel) is an FDA-approved device that uses electrical optical synergy (ELOS) technology for noninvasive body contouring and improvement of cellulite. It combines infrared (IR) light (700–2000 nm), bipolar RF (up to 35 W) and massage with suction (750 mmHg negative pressure).
Mechanism of action
The heating of fat with a combination of two modalities is thought to increase fat metabolism by dissociating oxygen from oxyhemoglobin. The IR light preheats the tissue, to which RF is drawn, and since the RF is more easily conducted through heated tissue, less energy is required. The IR penetrates to a depth of up to 3 mm and the RF portion reaches 2–20 mm. The suction and massage rollers rupture fat cell clusters and manipulate the vertical fibrous septa, both of which contribute to the improved skin appearance of cellulite. The device is used with a conductive lotion that is manufactured by the company.
Results
VelaSmooth has been shown to improve the appearance of cellulite in several studies. After a single treatment, histologic studies show that the VelaSmooth causes membrane rupture and incipient necrosis of adipocytes.
In a split body study, Romero et al. treated 10 patients with cellulite on the buttocks for a total of 12 sessions performed biweekly. The handpiece had an adjustable intensity, from 0–3, and all of the patients were treated at the highest intensity. Sessions lasted approximately 30 minutes and included 6–8 passes on one buttock. All patients had improvement in the appearance of cellulite, though results had decreased at the 2-month follow-up period. Following treatment, histologic analysis showed a realignment of the collagen fibers parallel to the dermal–epidermal junction and tightening of the dermal collagen, both of which contributed to the appearance of smoother skin texture.
VelaSmooth was studied by Kulick in 16 patients with cellulite on the posterior or lateral thigh, receiving biweekly treatments for 4 weeks. Patients reported a 75% improvement in cellulite appearance at 3 months and 50% at 6 months. The investigators noted 62% improvement at 3 months and 50% at 6 months. The improvement achieved from the treatments appeared to be relatively short-lived and monthly maintenance treatments were required to sustain the improvement.
As both of the above studies noted a decreased degree of improvement as time since treatment increased, it is thought that monthly treatments may be necessary for maintenance.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


