- •
Skin laxity is a common sign of photoaging
- •
Skin lifting and tightening are desirable outcomes for a large majority of patients interested in photo-rejuvenation
- •
Noninvasive treatment options for skin tightening and skin lifting are very limited.
- •
Micro-focused ultrasound with visualization (MFU-V) has been shown to provide skin lifting and tightening, making it the only FDA cleared technology (Ulthera Inc., Mesa, AZ) with a ‘lifting’ indication
- •
MFU-V is a safe and efficacious treatment for mild to moderate laxity
Introduction
Skin tightening and lifting continues to be a sought-after goal for millions of people across the globe. Despite much in the way of advances in our ability to improve and enhance various aspects of photoaging, until recently our capacity for safe and effective skin tightening has been limited. Photoaging occurs in a semi-predictable stepwise progression which includes both textural as well as pigmentary alterations to the skin. In the initial steps of skin aging, dynamic rhytides are evident in areas of skin movement and these eventuate into static rhytides. With further aging, the skin begins to develop laxity, which is often most evident in the jowls and submental skin. Photo-rejuvenation of the skin, in its optimum, should address all of these components of aging skin. Traditionally, various energy delivery devices have been used to treat several components of skin aging, including rhytides, laxity, and dyschromia, such as ablative CO 2 or Er:YAG laser devices, as well as treatments such as deep chemical peels and dermabrasion. These methods relied on ablation of the epidermis causing re-epithelialization while delivering significant thermal injury to the dermis sufficient to stimulate a robust wound healing response with subsequent collagen remodeling and contraction leading to decreased rhytides, improvement in skin texture, skin tightening and lifting, and improvement in pigmentation. However, despite significant improvement in these skin characteristics and efficacy of these treatments, significant patient downtime, long and painful post-treatment healing and substantial side effects were major drawbacks of these ablative procedures.
In recent years, multiple treatment modalities have become available for treatment of skin wrinkling and laxity in a nonablative manner. These include lasers and light devices, infrared energy devices as well as energy-based procedures including radiofrequency with and without ablation. These allow the use of thermal energy to target the reticular dermis and subcutis in an effort to cause tissue contraction and dermal remodeling whilst minimizing undesirable epidermal injury. As a result, ‘downtime’ is minimized with expedient post-procedure healing allowing the patient to proceed with their regular activities shortly after treatment and minimizing the necessity to interrupt a busy patient’s work or social schedule. Additionally, minimal epidermal injury allows for safer treatment among a wider range of skin types and reduces the risk of adverse events compared to either ablative resurfacing or more invasive surgical procedures such as rhytidectomy. However, the drawback of these safer nonablative methods is that, relative to their invasive and ablative counterparts, the results are often modest, less reliable, and result in an inconsistent duration of benefit. Individual variation in responsiveness to noninvasive skin tightening has also been significant. Ultrasound (US) is an energy modality that can be focused in the skin and subcutis to cause thermal coagulation at specific desired depths, while also allowing for real-time visualization of tissue targets for energy deposition. Micro-focused US with visualization (MFU-V) for skin rejuvenation has been shown in recent studies to be safe and effective for skin lifting and tightening.
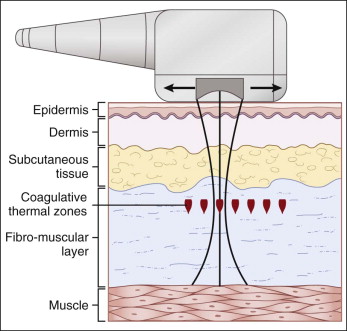
MFU-V delivers energy to selected foci within the dermis and subcutis leading to the generation of heat and selective coagulative changes.
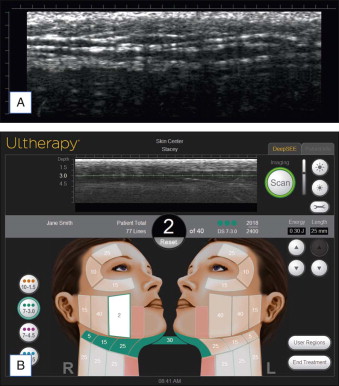
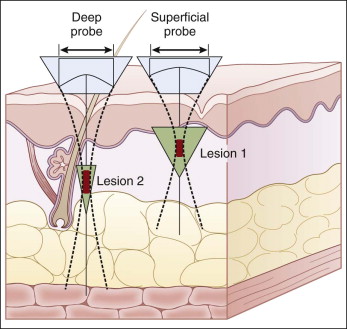
MFU-V delivers inducible energy to selected foci within the dermis and subcutis leading to the generation of heat and selective coagulative changes ( Fig. 4.1 ). The generated heat causes initiation of a tissue injury and repair cascade, the end result of which is a tightening of the skin. Results from several studies have led the currently available MFU-V device on the market, the Ulthera system ( Fig. 4.2 ), to receive the first Food and Drug Administration (FDA) approval for skin lifting, initially for eyebrow lifting in 2009, followed by an approval for lifting the submentum and neck tissue in 2012. An advantage associated with this device is that the built-in diagnostic ultrasound may potentially improve targeting and hence safety ( Fig. 4.3 ). Unfocused US energy can be used to image the treatment area while focused US energy can induce thermal injury of the mid to deep reticular dermis. Visualization of key structures with the diagnostic US can help ensure that the energy from the therapeutic device is delivered at the optimal points, and anatomic structures that do not need to be treated are spared.

The MFU-V device has been proven effective for the treatment of patients with mild to moderate laxity of the skin. Recently it has also been used in various other locations and applications, including tightening of the skin of the buttocks, décolleté, knees, and elbows, as well as for the treatment of acne and hyperhidrosis.
Proposed mechanism(s) of action
US includes the sound wave frequencies above the range of human hearing (18–20 kHz), and the Ulthera device operates at 4–10 MHz. US imaging is adapted to the visualization of the first 8 mm of tissue, thus specifically allowing for imaging of skin (see Fig. 4.3 ). The dual modality US device offered the capability of real-time imaging, which allows visualization below the skin’s surface as precisely-placed ‘thermal coagulation points’ (TCPs) are placed at prescribed depths. The resulting small micro-coagulation zones, approximately 1 mm 3 in size, cause thermal contraction of tissue. Subsequent wound healing results in neocollagenesis and collagen remodeling. A recent study using a safe nontoxic stable isotope (deuterated water) to quantitatively measure new collagen synthesis in vivo over a 4-week period following MFU-V treatment demonstrated that type I and type III collagen synthesis was increased by an average of 8.4% and 16.4%, respectively, when compared with control untreated tissue.
The generated heat causes initiation of the tissue repair cascade in which the end result is a tightening effect of the skin.
The Ulthera device consists of a central computerized power unit, a handpiece, and interchangeable transducers designed to target specific layers of the dermis and subcutis (see Fig. 4.2 ). The handpiece contains the transducer that enables sequential imaging (unfocused US energy, allowing visualization of dermal and subcutaneous structures) and treatment (delivery of focused US energy to create thermal injuries at specific depths in the skin).
The device initially had three transducers: 1) superficial: 7 MHz, 3.0 mm focus depth; 2) intermediate: 7 MHz, 4.5 mm focus depth; and 3) deep: 4 MHz, 4.5 mm focus depth. Most recently, a 10 MHz transducer capable of producing focal TCPs at depths of 1.5 mm into the dermis was introduced to induce more superficial dermal neocollagenesis. Human cadaveric tissues have demonstrated that penetration depth is determined by frequency, such that higher frequency waves produce a shallow focal injury zone and lower frequency waves have a greater depth of penetration to produce TCPs at deeper layers.
Each transducer delivers US energy in a straight 25 mm line with spacing between each TCP of 1.1 mm for the 1.5 mm and 3.0 mm depths, and 1.5 mm for the 4.5 mm depths. Short pulse durations (25–50 ms) and relatively low energy (in the 0.20–1.2 J range), depending on the particular transducer, confine the TCPs to their target depth ( Fig. 4.4 ). The handpiece is advanced in a line pattern at the set conditions (power, duration) and at the selective variables (length of treatment, spacing of exposures) to produce uniform tissue exposures for each ‘line’ of MFU-V treatment. Human cadaveric studies, as well as preclinical studies in porcine skin and pre-rhytidectomy excision skin, have confirmed consistency in the depth, size, and orientation of TCP created by MFU-V in the subdermal soft tissue and deeper superficial musculo-aponeurotic system (SMAS) layers, with preservation of immediately adjacent soft tissue and structures.
Thermal injury is confined by keeping the pulse duration relatively short. Provided that the energy delivered is not excessive for the focal depth and frequency emitted by a given transducer, the epidermal surface remains unaffected. Therefore, the need for epidermal cooling is eliminated. Since the tissue is altered by arrays of small zones of focal damage rather than ablation of an entire macroscopic area, rapid healing occurs from tissue immediately adjacent to the thermal lesions. This is somewhat analogous to fractional laser ablation, except MFU-V affects only the deep dermal and subcutaneous tissue, as per the transducer selected, and the thermal injury zones are wider.
The lifting and tightening effect of US treatment is based on coagulative heating of specific zones of the dermis and subcutaneous tissue. The US energy is micro-focused, such that thermal coagulation occurs only where the sound waves meet at discrete separated TCPs (see Figs 4.1 and 4.4 ). The size of the points varies based on the specific frequency and power settings used. This eventuates into nonsurgical tissue lifting without affecting the surface of the skin, thus making this technology safe to apply in all Fitzpatrick skin types with exceedingly low risk of hyper- or hypopigmentation. Apart from ionizing radiation, US is the only type of inducible energy that can be delivered arbitrarily deeply into tissue in a selective manner. The treatment is programmable for various depths and spacing based on transducer selection. Variability of energy delivery can occur in the actual treatment if there is improper skin contact, poor coupling, or too much pressure applied to the handpiece. Transcutaneous application of US into whole-organ soft tissue produces coagulative necrosis resulting primarily from thermal mechanisms. The US field vibrates tissue, creating friction between molecules, which absorb mechanical energy that leads to secondary generation of heat. Selective coagulative change is affected within the focal region of the beam, with the immediately adjacent tissue spared.
In MFU-V, energy is deposited in short pulses in the millisecond domain (50–200 ms). Avoiding cavitational processes, a frequency in the megahertz (MHz) range is used with energy levels deposited at each treatment site being on the order of 0.20–1.2 J. It is estimated that the device heats tissue to 65 °C–70 °C, the critical temperature at which collagen denaturation occurs with instigation of the tissue repair cascade. Precise microcoagulation points deep in the dermis as well as the SMAS have been demonstrated. Suh et al. demonstrate histologic evidence that both dermal collagen and elastic fibers are significantly regenerated and increase in number, resulting in thickening of the reticular dermis with no significant change in the epidermis. These authors conclude that it is via this dermal collagen regeneration that the rejuvenation of infraorbital laxity is achieved. This effect of increasing collagen synthesis has recently been quantitatively measured after treatment.
Microcoagulation is thought to cause gradual tightening of the skin through collagen contraction and remodeling. The initial collagen denaturation is followed by gradual tissue contraction over approximately 3 months. The duration of clinical lifting response is permanent but as patients continue to age, new collagen breaks down as part of the aging process. No controlled studies have thus far been performed to evaluate the clinical response relative to other similar skin-tightening treatments with radiofrequency or laser energy sources.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


