- •
Skin laxity is defined as the acquired loose, relaxed state of the skin that develops with age as a result of skin extensibility (stretch) and decreased skin recoil (return to original state after stretch)
- •
Intrinsic and extrinsic aging cause specific cutaneous changes, such as epidermal thinning, loss of collagen, degradation of elastin, and redistribution of subcutaneous fat, that all lead to significant skin laxity
- •
Factors that exacerbate skin laxity include advanced age, cumulative ultraviolet light exposure, smoking, menopause, and rapid weight gain
- •
Non-invasive treatment modalities, such as lasers, radiofrequency and high frequency ultrasound, aim to restore skin elasticity through stimulation of dermal fibroblasts, dermal reorganization, and collagen remodeling. Minimally invasive procedures, such as dermal fillers and autologous fat transfer, aim to restore skin turgor and volume. Surgical procedures such as rhytidectomy and blepharoplasty permanently remove excess or lax skin
Skin laxity is an acquired cutaneous state in which the skin becomes loose and lax secondary to loss of elasticity. Elasticity is defined as the ability of a material to return to its original state after stretching or straining. The amount of strain a material can endure before breakage is referred to as extensibility. Younger skin exhibits resilient elasticity and recoil when under stretch or stress. With age, elasticity begins to decrease at an early time point while extensibility is maintained well into the seventh decade of life, leading to gradual progression of skin slackness.
Anatomy and pathophysiology
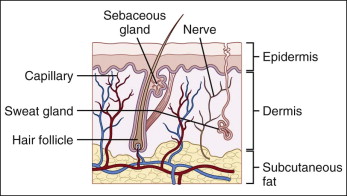
The skin is composed of three distinct layers, the epidermis, dermis, and hypodermis or subcutaneous tissue, that all undergo significant alterations as an individual ages ( Fig. 1.1 ), with one manifestation being change in skin elasticity. Cutaneous aging results from the interplay of several intrinsic and extrinsic factors. Intrinsic aging is a naturally occurring process caused by several factors including gradual oxidative damage and reduction in the rate of skin cell replication (resulting in dermal atrophy), elastic fiber degeneration, and loss of hydration, among many other microscopic changes. Extrinsic aging is due to environmental factors such as sun damage and smoking. Chronic ultraviolet (UV) exposure is the major cause of extrinsic aging, otherwise referred to as photoaging. Photoaging, superimposed on intrinsic aging, causes most of the visible age-related changes in the skin.
As chronic UV exposure is the single most important factor in extrinsic damage to the skin, the importance of mitigation through diligent sunscreen use and other sun-protective behaviors should be stressed to every dermatologic patient.
Epidermis
Although most of the cutaneous alterations that lead to increased skin laxity involve the dermis, changes within all skin layers exacerbate these effects. Alterations in the epidermis render the skin more vulnerable to damaging influences such as UV radiation, desiccation, and external stress, thereby worsening the cumulative effect of the aging process on the underlying structures of the skin. The most striking change in the epidermis is a flattening of the dermal–epidermal junction (DEJ), with effacement of the dermal papillae and rete pegs. This results in less surface area contact between the epidermis and underlying dermis. The decrease in contact surface area between the two skin layers reduces the strength of epidermal attachment to the dermis resulting in an increased tendency to form abrasions and blisters after minor trauma. In addition, the epidermis undergoes a thinning of 10 to 50% between the ages of 30 and 80 years. This atrophy of the epidermis is most notably appreciated in slack eyelid skin, where skin is the thinnest. Furthermore, epidermal stratum corneum lipid concentration declines, leading to a delay in tissue repair and restoration after external stress or trauma. Finally, active epidermal melanocytes are reduced by approximately 10 to 20% per decade, thereby decreasing melanin production and functionally impairing the protective barrier against UV radiation.
Dermis
Specialized junctions connect the dermis and the epidermis and help maintain mechanical integrity and cell-to-cell communication between these two layers. The dermis is the thickest layer of the skin, and is predominantly made up of collagen, elastin, and ground substance composed of glycosaminoglycans and proteoglycans, in addition to cells of the immune system, fibroblasts, blood and lymphatic vessels, nerve fibers, hair follicles and eccrine and apocrine glands. The dermis is further subdivided into two layers. The upper papillary dermal layer contains small, fine, and loose collagen fibrils, while the lower reticular dermis is composed of larger, denser, and interwoven collagen fibrils. The entirety of the dermis provides the skin with its collective tensile strength, elasticity, and malleability.
As cutaneous aging continues, the dermal layer progressively loses volume. The dermis thins by about 20% by late adulthood, and UV exposure tends to exacerbate this thinning. Histologic evaluation of aged skin also shows reduction in cellularity, depletion of vasculature, and loss of elastic fibers and dermal collagen.
Changes in collagen, elastin, and the ground substance cause a loss of flexibility and pliability, and eventual increase in rigidity of the skin. Normally, collagen composes the main structural component of the skin, accounting for 77% of its dry weight. It is stiff, has high tensile strength, and lacks extensibility. With aging, collagen content decreases by approximately 1% per year. Not only does the number of collagen fibrils decrease, but the collagen that remains loses organizational integrity, becomes more compact, and displays increased cross-linking. The increase in cross-linking may be due to a reduction in collagen synthesis, defects in collagen processing, and an increase in collagenases with age.
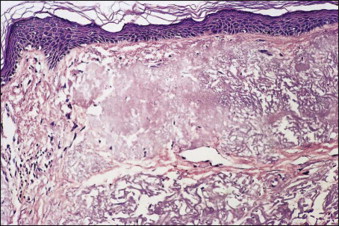
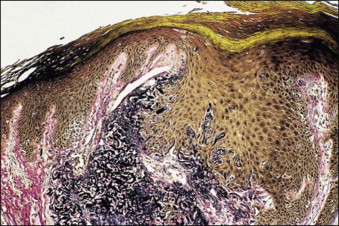
In addition to collagen, elastic fibers also undergo significant alterations with age. Elastin makes up about 4% of the skin’s dry weight. It is characterized by its elastic extensibility – the ability to stretch under stress but also to recoil and return to its original shape after the stress is removed. Therefore elastin and elastic fibers are inherently important in skin elasticity. It is estimated that as early as young adulthood, elastic fibers diminish in size and number. By late adulthood elastin is degraded, and elastic fibers lose their structural integrity leading to diffuse fragmentation, especially at the DEJ – a condition known as solar elastosis ( Fig. 1.2 ). Furthermore, elastic fibers display more cross-linking, progressive calcification, and at times trans-epidermal extrusion from the dermis ( Fig. 1.3 ). In addition to these structural changes, elastic fibers also endure compositional changes, exhibiting decreases in essential components including elastin and fibrillin. Fibrillin remains abundant in the deeper zones of the dermis; however, it becomes significantly reduced in the upper zone of the dermis. Aged skin displays significant decreases in fibulin-5, an extracellular protein that provides a support base for elastic fibers. Studies have shown that a decrease in fibulin-5 expression may be one of the earliest changes, and therefore markers, of cutaneous aging.
Beyond collagen and elastin, the other major structural component of the dermis is the ground substance located between collagen and elastic fibers. It is composed of proteoglycans, glycosaminoglycans (GAGs), and mucopolysaccharides. Of these, hyaluronic acid is most prevalent, and its presence decreases significantly with age – likely due to either decreased hyaluronic acid extractability or decreased hyaluronan secretion. This decrease in hyaluronic acid leads to the formation of altered or less functional ground substance. Overall, as the amount of collagen decreases, the amount of ground substance composed of altered GAGs and proteoglycans increases in photoaged skin. Normally proteoglycans bind about 1000 times their own weight in water and help direct proper collagen deposition, giving youthful skin its tensile strength and supple, voluminous turgor. Therefore, it is no surprise that deleterious age-related changes in the composition of these substances decrease dermal water content, as has been proven on ultrasound imaging, and thereby decrease skin turgor, elasticity and pliability, thus contributing to the appearance of laxity and rhytid formation.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


