Severe midface hypoplasia is often managed by Le Fort III distraction. Le Fort II distraction with zygomatic repositioning is a modification of the Le Fort III distraction operation aimed to correct abnormal facial ratios of patients with greater central than lateral midface deficiency. The operation starts with Le Fort III osteotomies and is followed by separation and fixation of bilateral zygomas. The central nasomaxillary Le Fort II segment is then distracted to achieve independent movements of the central and lateral midface. The Le Fort II zygomatic repositioning operation has become our procedure of choice for patients with Apert facial dysmorphology.
Key points
- •
Apert midface hypoplasia is characterized by central nasomaxillary deficiency that is more severe than the degree of hypoplasia present at the lateral orbitomalar region.
- •
Le Fort II distraction with zygomatic repositioning allows for differential advancement of the central and lateral components of the midface to correct the relative central deficiency for Apert midface hypoplasia and other similar conditions.
- •
Early outcomes of Le Fort II distraction with zygomatic repositioning demonstrate normalization of facial ratios in patients with Apert syndrome, significant increases in the nasopharyngeal airway volume, and comparable complication profile to Le Fort III distraction.
Background
Severe midface hypoplasia is commonly associated with syndromic craniosynostosis and can lead to several functional problems including exorbitism, airway obstruction, and malocclusion. Subcranial Le Fort III distraction osteogenesis has become the standard treatment for correction of severe midface hypoplasia. However, surgical movement of the entire midface may not adequately address all forms of midface hypoplasia. In a subset of patients, the degree of hypoplasia varies between the central nasomaxillary region and the lateral orbitozygomatic region. For example, the midface of patients with Apert syndrome is characterized by the presence of a central concavity in the setting of a retrusive midface. This is caused by a severe deficiency in the sagittal and vertical dimension of the central midface relative to the lateral midface. Unlike the midface hypoplasia associated with Crouzon syndrome, the Apert facial dysmorphology has been described as an abnormal face in an abnormal position.
The en bloc midface advancement achieved through Le Fort III distraction corrects exorbitism and malar hypoplasia through sagittal advancement of the inferior orbital rims and the body of the zygomas. The extent of sagittal advancement in the central nasomaxillary region with the Le Fort III operation is limited by the risk of causing enophthalmos, and vertical lengthening is limited by the risk of creating excessive orbital height. Therefore, the relative central midface vertical and axial deficiency remains undercorrected in patients with Apert syndrome after a Le Fort III operation because of these limitations imposed by the adjacent zygomas. Le Fort II distraction with simultaneous zygomatic repositioning (LF2ZR) was designed with the goal of differential and unrestricted movement of the central midface relative to the lateral zygomas, thus achieving not only advancement of the existing hypoplastic facial structures but also normalization of the facial ratios. ,
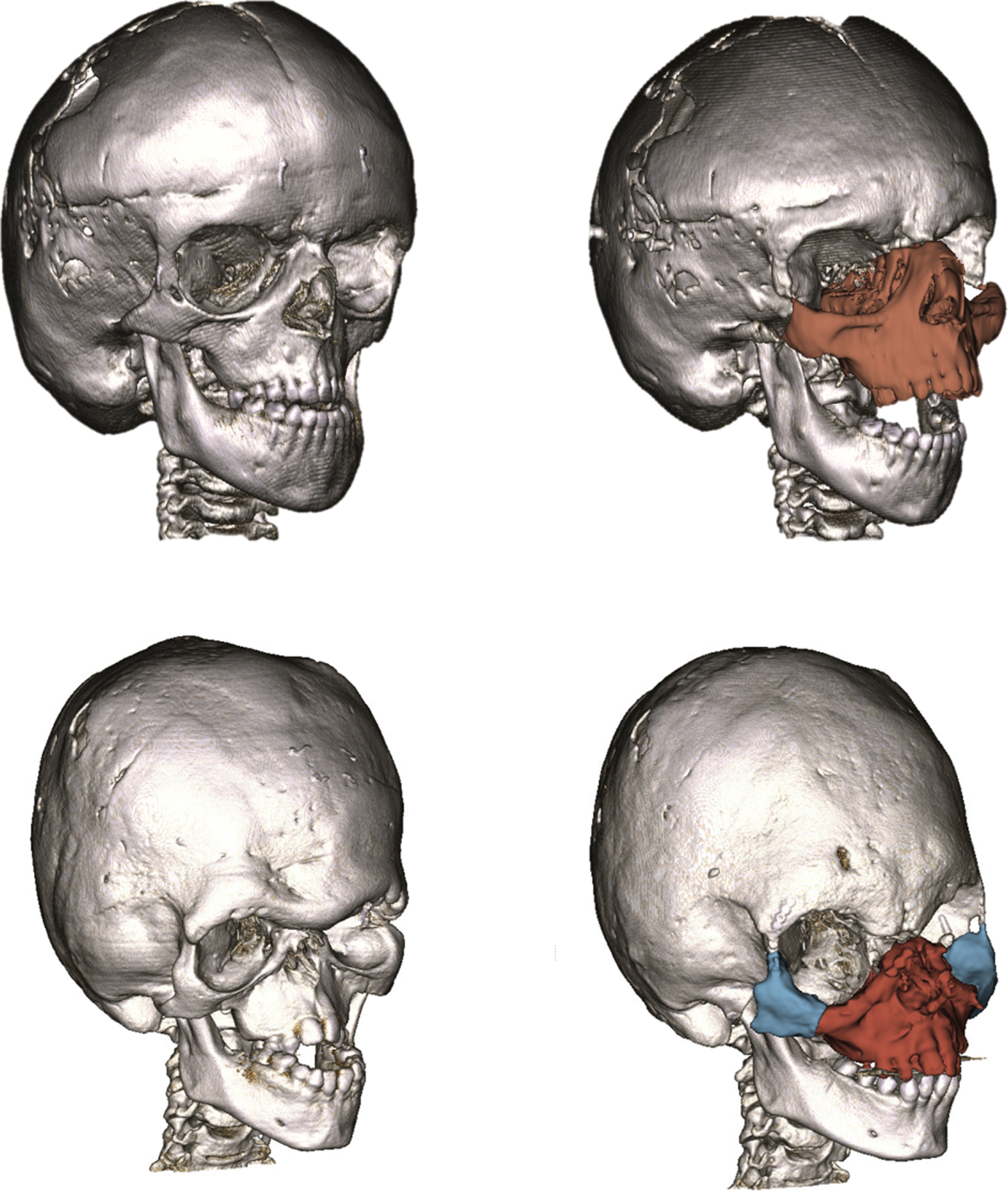
LF2ZR involves a single surgery that first repositions and fixates the Le Fort III osteotomy to optimize lateral malar position, followed by osteotomy at the Le Fort II level to allow unrestricted movement of the central nasomaxillary region through distraction osteogenesis ( Fig. 1 ). The smaller advancement and elevation of the zygoma segments correct exorbitism and malar hypoplasia, whereas the subsequent greater advancement and vertical lengthening of the Le Fort II osteotomy corrects the biconcave deformity of the syndromic midface without affecting globe position because of the support from the fixated zygomas. The LF2ZR operation was first described for the correction of the characteristic central midface deficiency associated with Apert syndrome, but the indications for LF2ZR also include other conditions where a differential magnitude of hypoplasia exists between the central and lateral midface. ,
Indications
Apert and Pfeiffer Syndromes
Patients with Apert, Pfeiffer, and Crouzon syndromes share the phenotype of midface hypoplasia that is characterized by a concave lateral facial profile. Unlike Crouzon syndrome, Apert and Pfeiffer facial dysmorphology is also characterized by a more profound retrusion and vertical deficiency of the central nasomaxillary region compared with the lateral orbitozygomatic regions, resulting in an additional concave facial profile on worm’s-eye view and frontal view. These three conditions are also characterized by a down-slanting palpebral fissure. However, in Crouzon syndrome this is secondary to lateral canthal dystopia, whereas in Apert and Pfeiffer, it is caused by an elevation of the medial canthus from the central facial vertical impaction. The vertical lengthening and advancement of the central Le Fort II segment in LF2ZR not only corrects this biconcave deformity of Apert and Pfeiffer syndromes, but it also creates a desirable lengthening of the nose and downward movement of the medial canthus to improve the periorbital esthetics ( Fig. 2 ).

Achondroplasia
Certain patients with achondroplasia share a similar facial dysmorphology with Apert syndrome where the central midface hypoplasia is more severe than the lateral midface, and associated obstructive sleep apnea is common. Le Fort III distraction alone has been shown to be limited in treating the central hypoplasia of the face and the obstructive apnea in these patients. LF2ZR has the potential for greater airway expansion by distracting the central nasomaxillary region independent of the zygoma positions. This differential movement treats the nasopharyngeal compression while avoiding enophthalmos ( Fig. 3 ).

Positive-Pressure Therapy Induced Midface Retrusion
Children with obstructive sleep apnea who require high-pressure nasal positive-pressure airway therapy at an early age can develop midface retrusion as a result of the effect of constant pressure on the growing facial structures. The nasomaxillary region tends to be the most affected area, because the pressure of the mask is focused on this region, and can cause challenges in maintaining mask fit and air seal. In these patients, Le Fort II distraction with or without zygomatic repositioning depending on the degree of zygomatic retrusion can advance and lengthen the central midface to improve airway anatomy, facial balance, and fit of the pressure mask ( Fig. 4 ).

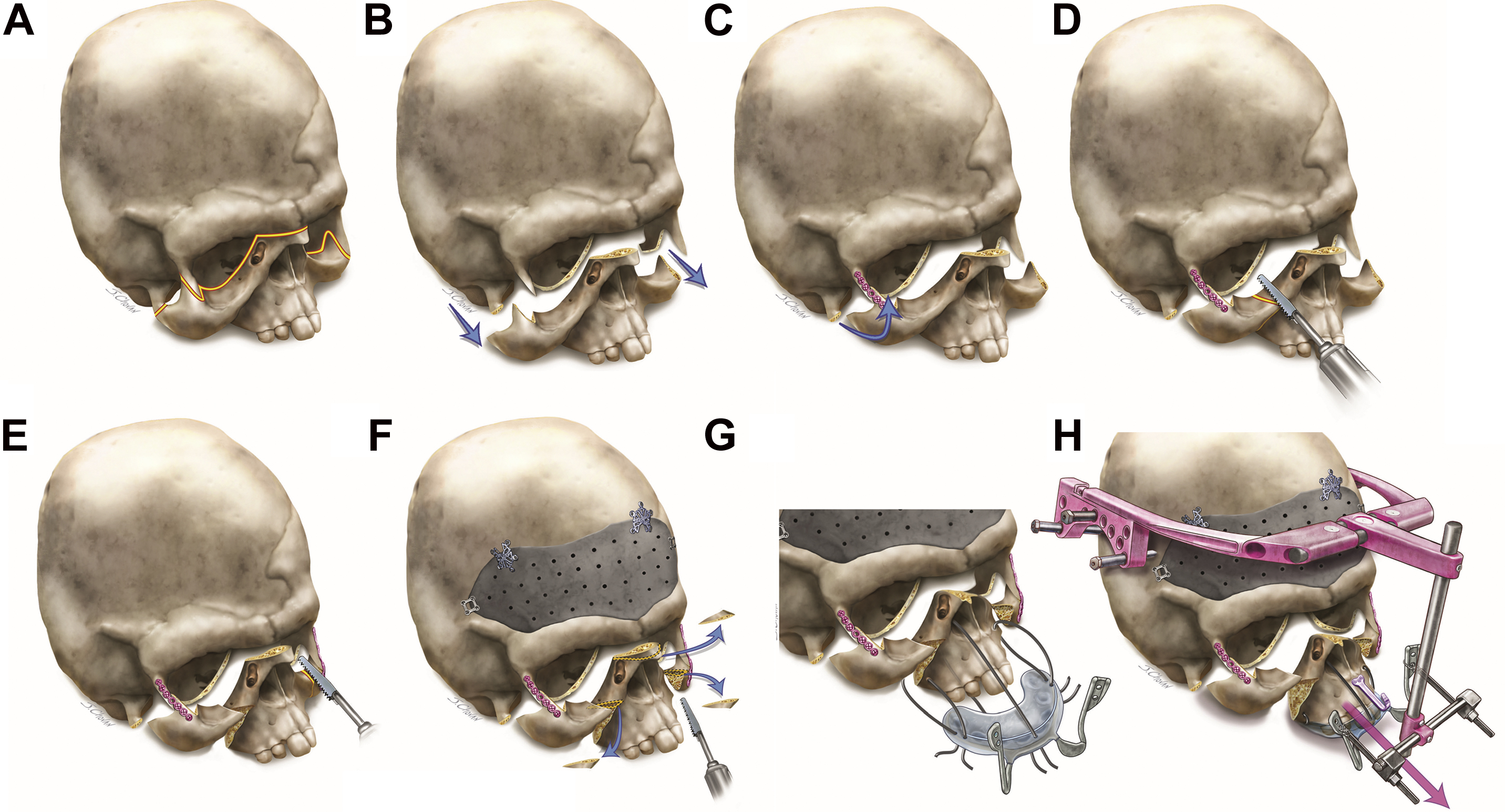
Surgical technique
A detailed description of the surgical technique of LF2ZR was previously published. We recommend performing the operation on patients at age of 7 years or older, with an ideal age range of 9 to 12 years. Performing LF2ZR before 7 years of age can result in zygoma instability or resorption. Next is a summary of the operative steps ( Fig. 5 ).
Le Fort III Osteotomy
- •
A coronal incision is used to expose the upper midface.
- •
Dissection is performed in the subperiosteal plane with reflection of the anterior portion of the temporalis muscle bilaterally to expose the anterior zygomatic arch laterally and nasofrontal region centrally.
- •
The zygomatic arch osteotomies are performed with a reciprocating saw just behind the body of the zygomas without disruption of the posterior temporalis muscle.
- •
Stepped osteotomies of the lateral orbital walls are made from the zygomaticofrontal suture down to the inferior orbital fissure using a piezoelectric or reciprocating saw.
- •
A small osteotome from the lateral orbit creates an osteotomy along the orbital floor from the inferior orbital fissure to the uncinate process behind the lacrimal fossa.
- •
A piezoelectric saw is used to perform an osteotomy at the nasofrontal junction, which is carried along the medial orbital wall behind the lacrimal fossa to join the orbital floor osteotomy.
- •
From underneath the lateral orbit an osteotome is placed in the orbital floor osteotomy at the anterior edge of the inferior orbital fissure and used to continue the osteotomy along the posterior maxillary sinus wall, down to and through the pterygomaxillary junction.
- •
The pterygomaxillary separation is completed from this lateral coronal incision approach or from a permucosal intraoral access directly at the pterygomaxillary junction.
- •
A septal osteotome is used to perform the posterior septal osteotomy from the nasofrontal junction toward the posterior nasal spine.
- •
Down-fracture of the midface is performed with careful manual pressure, and the midface is mobilized with Rowe-Killey forceps.
Zygomatic Repositioning and Le Fort II Osteotomy
- •
The mobilized Le Fort III segment is tilted and advanced to place one zygoma in the desired position based on the stepped osteotomy. It is then fixated using a 1.5- to 1.7-mm titanium plate across the repositioned lateral orbital wall osteotomy.
- •
The typical movement of the zygoma is 5 to 8 mm anterior and 3 to 5 mm superior.
- •
Through an upper gingivobuccal sulcus incision, the fixated zygoma is released from the maxilla using a piezoelectric saw lateral to the infraorbital nerve. Care is taken to preserve the zygomatic retaining ligament and periosteal attachments to avoid vascular compromise of the zygomatic segment.
- •
The same sequence is performed on the contralateral side to reposition, fixate, and release the contralateral orbitozygomatic complex.
Adjunctive Procedures
- •
The zygomatic repositioning and Le Fort II osteotomy have now been completed.
- •
A custom onlay forehead implant is inserted during the LF2ZR surgery to treat the forehead contour irregularities that are commonly present in Apert patients.
- •
In anticipation of the potential for bony step-offs that can occur after distraction of the Le Fort II segment, small wedges of bone are removed at the nasofrontal and inferior orbital osteotomy edges.
- •
Although the vertical distraction of the Le Fort II segment helps correct medial canthal position, lateral canthopexies should also be performed at this time to resuspend the canthal ligament inside the superior lateral orbital wall.
- •
The coronal incision is then closed after thorough irrigation and resuspension of the temporalis muscle.
Le Fort II Distraction
- •
Through the intraoral incisions, a custom acrylic splint containing an embedded portion of a face bow with two extraoral loop extensions is secured to the maxilla using 26-gauge steel wire loops through bone holes in the piriform rim and lateral maxillary buttresses.
- •
The intraoral incisions are then closed, and orthodontic bone anchors are inserted at the midline of the maxilla and mandible to allow for inferior vector control with elastics during activation.
- •
A halo-based rigid external distraction device is secured using cranial pins with a mounted vertical midline post and transverse activation arms.
- •
The activation arms are set at a 30° to 45° downward vector relative to Frankfort horizontal and secured to the maxillary traction splint extensions with 24-gauge steel wires.
Postoperative Care
- •
Patients are kept intubated and sedated for 2 to 3 days postoperatively in the intensive care unit until an air leak is confirmed.
- •
After a latency period of 3 to 5 days, distraction begins at a rate of 1 to 1.5 mm per day, with a shorter latency and faster rate used for younger patients.
- •
The distraction vector is decided based on the goals of augmenting the dorsal nasal length, increasing the vertical maxillary height, leveling the palpebral fissures, and correcting the maxillary occlusal plane.
- •
The end point of Le Fort II distraction is determined by maximizing advancement without the medial lids losing their scleral contact, and vertical lengthening that achieves a level palpebral fissure. This should bring the patient into an overjet position, demonstrating the associated mandible hypoplasia and common need for mandible advancement surgery at skeletal maturity in these patients.
- •
The external distraction device is removed after 6 to 8 weeks of consolidation.
Clinical outcomes
Correction of Abnormal Facial Ratios
Patients with Apert syndrome have a relative deficiency in the facial ratios of central to lateral midface in the worm’s-eye view (axial facial ratio) and the frontal view (vertical facial ratio). Our retrospective study comparing LF2ZR and Le Fort III distraction in Apert patients found that Le Fort III distraction left the abnormal facial ratio unchanged after midface advancement. In comparison, after LF2ZR surgery, the axial and vertical facial ratios of the treated Apert patients became similar to those of Crouzon patients and normal control subjects. This correction was achieved through differential movements with LF2ZR in which the central midface was advanced an average of 18.0 mm and lengthened 13.5 mm compared with only 5.2 mm of advancement and 2.9 mm of lengthening for the lateral midface.
In addition to correction of the abnormal facial ratio, the large magnitude and inferior vector of central midface advancement can also lead to other desirable facial changes in this patient population. Patients with Apert syndrome often have downward oriented palpebral fissures with the medial canthi positioned close to the nasofrontal junction and higher than the lateral canthi. With the medial canthi attached to the Le Fort II segment, the inferior advancement of the nasomaxillary region relative to the lateral orbital region can have a favorable effect by leveling the palpebral fissure. Other periorbital features of Apert syndrome include soft tissue bulges overlying the inferior orbital rims and prominent nasojugal folds that result from the worm’s-eye concavity. These features are improved by the differential inferior and anterior movement of the medial orbit relative to the lateral orbit, which is moved superiorly. Other facial features that are improved include the short nasal dorsum, which is lengthened by the inferior distraction of the nasomaxillary complex, and the anterior open bite, which is reduced through a clockwise rotation of the palate. Thus, LF2ZR allows for correction of the abnormal facial ratios and many of the facial features that contribute to the stigmata of Apert syndrome.
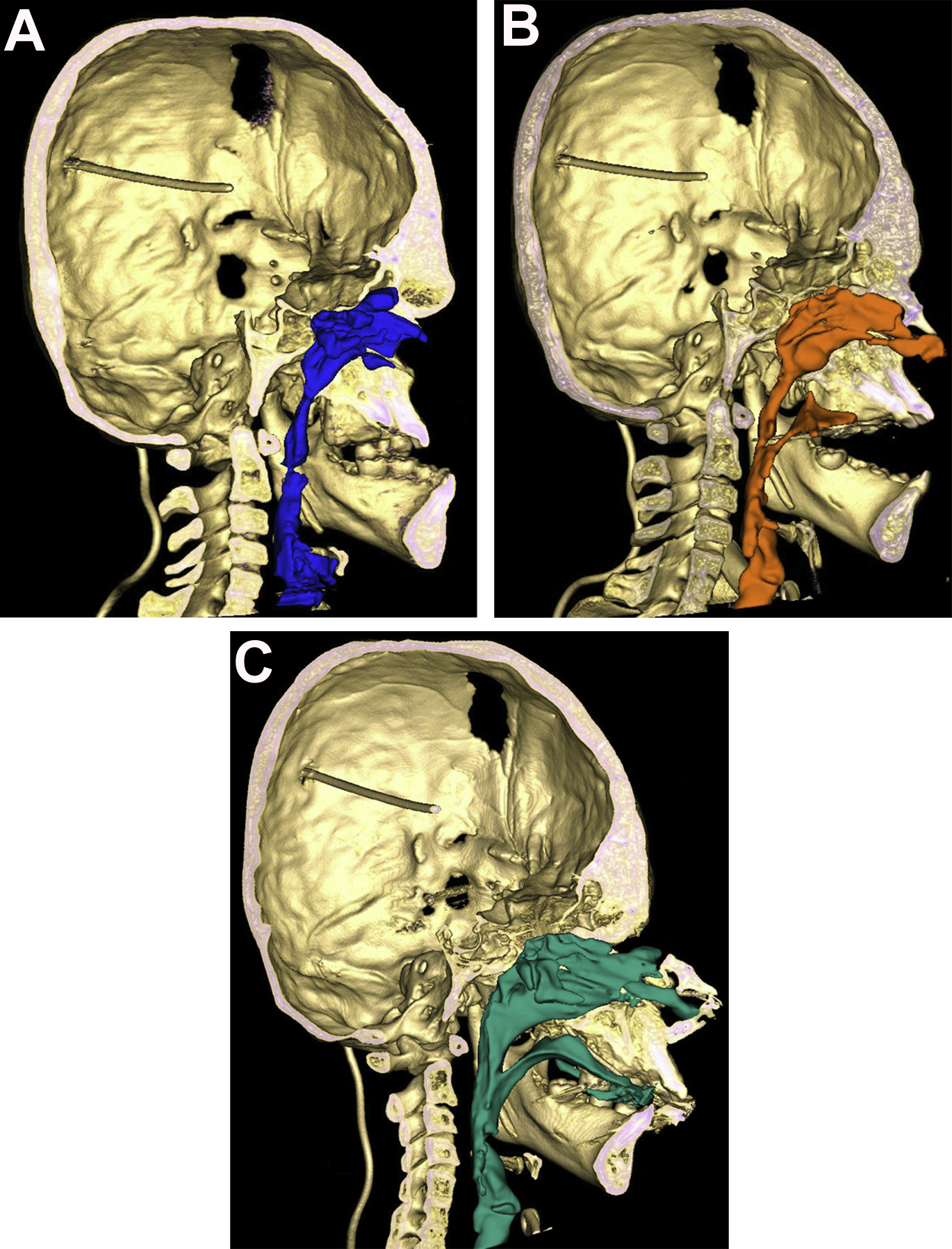
Airway Changes
Severe midface hypoplasia can contribute to upper airway obstruction and is commonly associated with obstructive sleep apnea. Volumetric changes to the upper airway secondary to Le Fort III distraction and LF2ZR are illustrated in Fig. 6 . Advancement of the midface via Le Fort III distraction has been shown to increase upper airway volume, improve polysomnography study results, and lead to the resolution of obstructive sleep apnea in a subset of patients after surgery. Previous studies have found that the greatest increase in airway volume after Le Fort III advancement occurs at the nasopharyngeal level. , Although outcomes data on airway changes after LF2ZR are limited, our center has found that improvement in sleep apnea measures and airway volume is most dependent on the magnitude of horizontal displacement of the midface, and not on the technique, palate rotation, or vertical movement. Taken together, these findings emphasize the importance of fully correcting the central midface deficiency in syndromic children regardless of surgical procedure. In patients with differential central midface hypoplasia, this is not possible without a segmental procedure, such as LF2ZR.