Le Fort I Osteotomy and Advancement
Kathlyn Kruger Powell
Ahmed Elsherbiny
John H. Grant III
DEFINITION
A procedure that involves cutting and repositioning the maxilla to the correct position
It is one of the most common procedures used to correct maxillary dentofacial deformities including size, position, orientation, shape, and/or symmetry.
Often performed with corrective mandibular ramus surgery such as a bilateral sagittal split osteotomy (BSSO)
Corrects in three planes: vertical, horizontal, and transverse
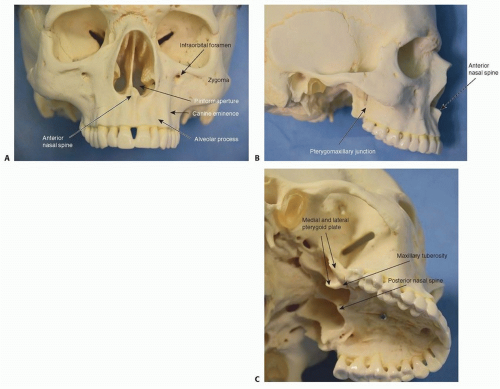 FIG 1 • Osseous anatomy of maxilla: anterior (A), lateral (B), and basal oblique (C) views. |
ANATOMY
Osseous Structures
In the anterior view of the skull, the maxilla (FIG 1) forms the piriform aperture and inferior and medial border of the orbit.
The anterior surface of the maxilla is the anterolateral wall of the maxillary sinus.
From the piriform rim to the descending palatine canal, the mean length of the medial sinus wall is 34 mm; therefore, when creating the osteotomy in the lateral
nasal wall, it should be no further posterior than 25 to 30 mm from the piriform rim.1
The infraorbital foramen is at a variable distance from the inferior orbital rim and the maxillary alveolus, 8 to 20 mm from the nasal floor.
The nasolacrimal duct lies within the thin bony wall of the maxillary sinus and the nasal cavity. The duct ends at the inferior nasal meatus through the valve of Hasner.
The inferior nasal meatus is 11 to 14 mm posterior to the piriform aperture and 11 to 17 mm above the nasal floor.2
The root prominences are occasionally visible through the maxillary alveolar process.
The canine is the longest root.
Anterior teeth roots are typically more visible.
The maxillary suture at the inferior midline of the piriform aperture forms the anterior nasal spine (ANS), and the anterior maxilla surrounds the piriform aperture.
Extending posteriorly from the ANS is the nasal crest of the maxilla, which joins the nasal septum. The nasal floor is formed by the maxillary roof.
The piriform rim (nasomaxillary buttress) is a vertical pillar of medial midface support. The zygomaticomaxillary buttress is the pillar of lateral midface support.
The septal or quadrangular cartilage, the vomer, and the perpendicular plate of the ethmoid bone articulate in the midline with the nasal crest.
The junction of the premaxilla and the maxilla contains the incisive foramen, which contains the nasopalatine vessels and nerves.
The hard palate is formed by the fusion of the palatine processes of the two hemimaxillae and the horizontal lamina of the palatine bones.
The posterior border of the maxilla is the maxillary tuberosity.
The pterygomaxillary fissure is located between the maxillary tuberosity and the pterygoid plates of the sphenoid bones.
The descending palatine artery is 10 mm medial to the maxillary tuberosity.1
Muscular Structures
The orbicularis oris surrounds the stomion (origin: buccinators, depressor anguli oris, levator anguli oris).
Risorius (origin, fascia overlying the parotid gland; insertion, angle of the mouth)
Zygomaticus major (origin, zygomatic bone; insertion, skin at the angle of the mouth and orbicularis oris)
Zygomaticus minor (origin, zygomatic bone; insertion, skin of the upper lip)
Levator labii superioris (origin, maxilla; insertion, skin of the upper lip)
Levator labii superioris alae nasi (origin, frontal process of the maxilla; insertion, skin of the upper lip)
Levator anguli oris (origin, maxilla; insertion, skin of the upper lip)
Levator labii superioris alaeque nasi (origin, upper frontal process of the maxilla; insertion, upper lip and ala of the nose)
Depressor septi (origin, incisive fossa of the maxilla; insertion, base of the columella and the nasal septum)
Nasalis muscles (origin, maxilla; insertion, alar cartilage)
Medial fibers blend with depressor septi.
Responsible for compression and dilation of nares
Primary muscle in alar base cinch
Vascular Anatomy
Arteries
Perfusion of the maxilla via three main vessels
Ascending pharyngeal
Ascending palatal
Soft palate vessels
Must maintain posterior pedicle when sacrificing the descending palatine arteries
Veins
Pterygoid plexus
Surrounds the maxillary artery
Deep to the lateral pterygoid muscle
Pterygoid plexus drainage
Drains to the maxillary vein
Drains to the deep facial vein and then the facial vein
Drains to the cavernous sinus through the foramen ovale
Drains to the middle meningeal veins through the foramen spinosum
PATIENT HISTORY AND PHYSICAL FINDINGS
Past medical history, surgical history, allergies, social history, and family history should be elicited.
Patient history should include questions regarding difficulty chewing food, headaches, temporomandibular joint dysfunction (TMD), speech, growth, and breathing.
Growth evaluation may include the following:
Serial physical examinations
Serial cephalometric radiographs
A hand-wrist film
Evaluation of maturation of vertebrae on a lateral cephalometric radiograph
TMJ examination
Examine muscles of mastication of TMJ capsule for tenderness to palpation.
Examine for clicking, popping, or crepitus.
Examine for excursive movements, protrusion, and maximal incisal opening.
Examine for deviation upon opening.
Skeletal examination
Vertical orbital dystopia
Measure intercanthal distance.
Placement of nose in relation to facial midline
Transverse dimension
Maxillary midline in relation to facial midline
Mandibular midline in relation to maxillary midline and facial midline
Chin point in relation to facial midline
Maxillary occlusal plane and cant in relation to the maxillary canine teeth
Mandibular occlusal plane level vs canted
Mandibular angles level vs canted
Maxillary arch width (evaluate utilizing handheld dental models)
AP dimension
Overjet
Nasolabial angle
Labiomental fold
Chin position
Profile
Vertical dimension
Facial thirds
Maxillary incisor length
Maxillary incisor show at rest and high smile
Gingival show at rest and high smile
Dental examination
Overall dental health
Missing teeth
Presence of third molars
Overbite
Overjet
Angle class of occlusion
Arch width (evaluate utilizing handheld dental models)
Curve of Spee
Dental decompensation
Periodontal health
Soft tissue examination
Upper lip thickness and length
Nasolabial angle
Nasal tip rotation
Patients with maxillary deficiency often appear to have a retruded upper lip, flat malar eminences, deficiency in the infraorbital rims as well as paranasal sinuses, inadequate tooth show, and a prominent chin relative to the midface
Patients have a “psuedoprognathism” with reverse anterior overjet.
Patients with vertical maxillary excess (VME) have a long face with excessive gingival show
Mouth breathing is common.
Class II malocclusion is common.
IMAGING
Panoramic radiograph should be examined for the following:
Health of dentition
Presence of third molars
Pathology
Health of the temporomandibular joint
Presence of hardware from previous facial surgery
Lateral cephalometric radiograph with the patient’s lips relaxed and the mandible in centric relation
Assess the anteroposterior (AP) position of the maxilla.
Assess the AP position of the mandible.
Assess the AP discrepancy between the maxilla and the mandible.
Assess the maxillary incisor inclination.
Assess the mandibular incisor inclination.
Assess the facial type.
Assess the chin.
Preoperative profile, frontal (smiling and rest), and occlusal photographs should be obtained.
Dental models made of stone casts or digital scans are used to evaluate the dentition as well as to establish the new occlusion.
Cone beam computed tomography (CBCT) or computed tomography (CT) is done for virtual surgical planning (VSP) and/or complex asymmetry cases.
PA cephalometric radiograph may be needed in complex cases if CBCT or CT is not an option.
NONOPERATIVE MANAGEMENT
Orthodontic camouflage is an option for nonoperative management if the deficiency falls within the envelope of orthodontic treatment as described by Proffit.3
SURGICAL MANAGEMENT
Preoperative Planning
Panoramic dental x-ray, cephalometric analysis, and/or cone beam CT should be reviewed.
Model surgery or VSP should be performed in order to determine the most appropriate movements of the maxilla.
A surgical splint will be fabricated from the model surgery or virtual surgical planning.
The need for a bone graft for stability should be determined.
Autogenous bone should be harvested prior to the start of the Le Fort I osteotomy.
Allogenic bone is used frequently as well.
Positioning
A standard nasotracheal intubation is performed with a Nasal RAE endotracheal tube.
The tube is secured with a headwrap over the forehead. This brings the tube out of the operative site (FIG 2).
The eyes are lubricated and covered with Tegaderm.
The patient is placed supine with the head of bed slightly elevated.
The arms are tucked at the patient’s side and padded in standard fashion.
Approach
An upper buccal sulcus incision with lateral back cut has the advantage of better preservation of blood supply with sufficient access when compared to the traditional longer incision.
A vertical incision up the zygomatic buttress improves both vascularity and access.
 FIG 2 • Fixation of the endotracheal tube. |
TECHNIQUES
▪ Preparation and External Reference
The patient is prepped and draped with four towels and a head and neck drape.
The mouth is thoroughly irrigated with chlorhexidine gluconate 0.12% oral rinse.
The orthodontic appliances are carefully examined. The surgeon should know which teeth have bands and brackets and if any brackets are missing. This is in the event that brackets are dislodged during the case. The surgeon will know to look for them and not inadvertently leave them in the wound. This is particularly important when there is a mandibular vestibular incision for a simultaneous sagittal split osteotomy.
If possible, hypotensive anesthesia with a MAP less than 60 should be performed when the maxilla is down-fractured.
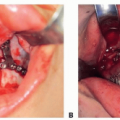
Local anesthesia with epinephrine is infiltrated into the maxillary vestibule from second molar to second molar. Bilateral posterior superior alveolar and greater palatine nerve blocks are administered (TECH FIG 1A).
An external reference in addition to directly measuring marks on the bone is more accurate when the vertical position of the maxilla is going to be changed.
A 0.035-inch K-wire is placed in the glabella (nasal bone) as an external stable reference. Soft tissue markers are not accurate.
A measurement from the K-wire to the maxillary arch wire at the central incisors is recorded utilizing a Boley gauge (TECH FIG 1C).
The soft tissue midline is marked on the upper lip and verified with the dental midline (TECH FIG 1B).
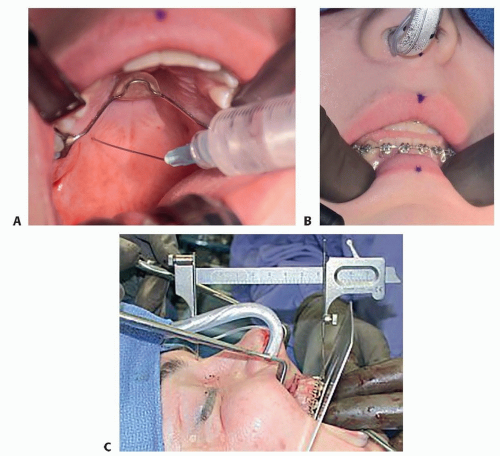 TECH FIG 1 • A. Greater palatine nerve block given in the right side. B. External reference placed on the upper lip midline. C. Glabellar K-wire and Boley gauge.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|