- •
Laser and light-based modalities are one of the latest advances in the treatment of cellulite
- •
External light irradiation has the capacity to trigger a photobiomodulatory effect in the targeted tissue stimulating several cellular functions such as neocollagenesis or adipocyte lipolysis. The therapeutic benefit stems from a thermogenic or nonthermogenetic effect
- •
Green (532 nm), red (650 nm) and infrared (700–2000 nm) laser light in a low- or high-energy level is used for cellulite treatments
- •
Depending upon the wavelength, intensity, and total energy delivered, the therapeutic benefit of light-based treatment modalities stems from a thermogenic or nonthermogenetic effect
- •
Long-term effectiveness has not yet been proven with any of the medical devices available
Introduction
Cellulite is a topographic and localized alteration of the skin that creates a dimpled or ‘orange peel’ appearance, most commonly found on the posterolateral thighs, buttocks, and abdomen. In 1978, Nürnberger and Müller first described cellulite as a result of sex-related differences in the structure of skin and subcutaneous tissue. The perpendicular orientation of the fibrous septa in women allows protrusion of the underlying fat, creating a rippled appearance. The oblique nature of these fibers in men appears to prevent this phenomenon. More recent studies confirm these sex-related structural differences, and further explain the appearance of cellulite to be a result of the convergence of several overlapping physiological alterations such as focally enlarged fibrosclerotic septa that tether the skin in areas of cellulite, or an uneven dermal–hypodermal interface.
Although precise epidemiological data are lacking, most studies claim that cellulite is present in over 80–90% of post-pubertal women. Given the ubiquitous nature of cellulite, it is more appropriately thought of as a secondary sex characteristic rather than a disease. However, as digitally altered images of women’s bodies in the media have become the new standard of ‘beauty’, the perception is that cellulite affects only the unlucky few. As such, it has become a major cosmetic concern for women.
Treatment
Although cellulite is not a disease in the proper sense and there is currently no cure for it, numerous treatment modalities have been developed to improve the appearance of cellulite. There are a myriad of over-the-counter creams that purport to remove cellulite; however, there is little evidence demonstrating efficacy of these products. Currently available medical devices aim to target the structural features of cellulite. In addition to the application of ultrasound and radiofrequency (RF) energy and mechanical manipulation and disruption, laser and light-based modalities are one of the latest advances in the treatment of cellulite.
Historically, various light sources have been used in physical therapy to reduce pain and inflammation, although the exact mechanism of action was widely unknown. Only recently, it became evident that external laser and light emitting diode (LED) irradiation has the capacity to trigger a photobiomodulatory effect in the targeted tissue stimulating several cellular functions such as neocollagenesis or adipocyte lipolysis. Depending on the wavelength, intensity, and total energy (J/cm 2 ) delivered, the therapeutic benefit may stem from a thermogenic or nonthermogenetic effect.
VelaSmooth ™
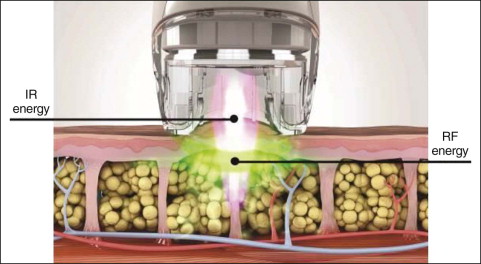
The VelaSmooth™ technology (Syneron Medical Ltd, Yokneam, Israel) is based on the simultaneous application of light energy to the tissue at a controlled infrared (IR) wavelength, conducted RF energy, and mechanical manipulations of the skin and fat layer. It was the first medical light-based device to achieve FDA approval. Bipolar RF (up to 35 W) and infrared light in the wavelength range of 700–2000 nm are used to heat the subcutaneous tissue, while vacuum suction is applied to shape the skin for optimal delivery of RF energy up to a depth of 15 mm. Proposed tissue reaction to the VelaSmooth technology is an increase in local blood supply to the subcutaneous tissue promoting an increase in fat metabolism. Eventually, the mechanical action due to suction and massage lead to a collapse of fat cell clusters and fibrous bands smoothing the skin surface.
Further advancements of the VelaSmooth technology are the VelaShape™ II and VelaShape III devices (see Table 14.1 ). Both use the combined modality treatment of controlled heating and mechanical action ( Fig. 14.1 ), but offer a more powerful RF power up to 150 W allowing a faster and deeper heat penetration into the tissue. With these alterations, treatment duration is shortened by approximately 30%, and fewer treatment sessions are needed.
| IR power | IR light spectrum | RF power | RF frequency | Vacuum suction | Massage | |
|---|---|---|---|---|---|---|
| VelaSmooth™ Plus | Up to 35 W | 700–2000 nm | Up to 35 W | 1 MHz | 200 mbar | Yes |
| VelaShape™ II | Up to 35 W | 700–2000 nm | Up to 60 W | 1 MHz | 200 mbar | Yes |
| VelaShape™ III | Up to 3.3 W | 850 nm | Up to 150 W | 1 MHz | 350 mbar | Yes |
A conductive fluid is used immediately before treatment to hydrate the skin surface. Using the handheld applicator, the area of interest should be treated with 4–6 passes by moving the handpiece back and forth several times. Thereby, the applicator must be in full contact with the skin surface area to allow the vacuum to be most effective and to ensure that the electrode rollers are fully coupled to the skin. The endpoint of treatment is achieved when significant erythema and warmth radiating from the treated skin is observed. The average duration of a thigh and buttock treatment lasts about 30–45 minutes. The treatment is generally very well tolerated with only minimal to no discomfort. However, heating sensations and pinching as well as transient erythema, bruising and localized swelling have been reported.
One of the first studies evaluating the safety and efficacy of the VelaSmooth system was published by Sadick and Mulholland in 2004. Thirty-five female subjects with cellulite and/or skin irregularities on the thighs and/or buttocks received twice-weekly treatments for 4 and 8 weeks. Circumferential measurement and pre- and post-treatment photographs were used to grade the level of improvement. In most of the patients the thigh area showed an overall mild to moderate improvement in skin smoothing and cellulite appearance. The overall mean decrease in thigh circumference was approximately 0.8 inches.
Similar results were assessed in a study conducted by Alster and Tanzi who treated 20 female subjects with moderate bilateral thigh and buttock cellulite with eight biweekly treatments to a randomly selected side with the contralateral side serving as the control. Clinical improvement was scored from comparable photographs using a quartile grading scale by two blinded evaluators. Ninety percent of patients noticed overall improvement and clinical scores averaged 50% improvement upon completion of the study.
In another split side study, 10 subjects received biweekly treatments for 12 weeks to one side of the buttocks with the opposite side serving as the control. All patients were satisfied with the results 2 months post-treatment and requested treatment of the nontreated side. Histological analysis showed fiber compaction and tightening of skin layers, including the subcutis, which may account for the observed clinical improvement ( Fig. 14.2 ).
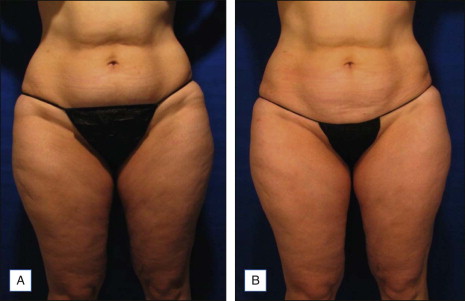
Long-term results for both the thigh and abdomen were first reported by Wanitphakdeedecha and Manuskiatti 1 year post-treatment. The long-term evaluation suggests that most of the circumference reduction is maintained for at least 1 year after the completion of 8–9 treatments twice a week (6.23% after the final treatment, and 5.50% 1 year later).
Baseline and follow-up standardized digital non-flash photographs with identical positioning and lighting are strongly recommended in order to track efficacy.
TriActive™
The TriActive™ (Cynosure Inc., Chelmsford, MA), a class II over-the-counter device, merges suction, massage, and contact cooling with the application of an 808 nm diode low-level laser.
Gold treated 10 female subjects with a total of 15 biweekly treatments, utilizing protocols determined by the device manufacturer. Of the nine subjects completing the study, there was an overall change on the Visual Cellulite Grading Scale from 2.44 at baseline, to 1.44 post-treatment. This represented an approximately 50% improvement. Length of follow-up was not noted in this study. Boyce et al. found an improvement of cellulite, skin texture, size and skin tone after biweekly treatments for 6 weeks. They stated that the greatest improvement was seen in those with the least symptoms.
In a study comparing the TriActive and the VelaSmooth devices, Nootheti et al. treated 26 female patients biweekly for 6 weeks. Treatment was randomized with use of the TriActive on one side and VelaSmooth on the other side. Patients were evaluated with photographs and circumferential thigh measurements before treatment and after the final treatment. Both devices produced modest improvements in the appearance of cellulite and the average mean percent age change calculated was roughly the same for both treatments.
Verjú
Verjú (Erchonia Corporation, McKinney, TX) is another low-level laser method that uses six 532 nm green diodes for improving the appearance of cellulite. Unlike common high-energy laser treatments, low-level laser therapy (LLLT) does not cause significant changes in the tissue structure, but, among its effects, it modulates adipocyte function by causing a transitory pore in the cell membrane, which purportedly drains the fat cell.
To date, only one study, by Jackson et al. , has been published on this device. This double blind, placebo-controlled randomized trial evaluated 68 subjects who received three weekly treatment sessions 2–3 days apart. During each session, the front and back of the hips, thighs, and waist were exposed for 30 minutes in total. All subjects in the LLLT group achieved a decrease of one or more stages on the Nürnberger–Müller grading scale and a significant decrease in thigh circumference at the 2-week study endpoint and 6-week follow-up evaluation. About 62.1% of the LLLT-treated subjects were ‘very satisfied’ or ‘somewhat satisfied’ with the clinical outcome.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


