If one examines the timeline of progression in cosmetic surgery, there would be a big annotation around the early 1990s dedicated to lasers. Although lasers had been used sporadically 50 years earlier, the 1990s ushered in predictable clinical science and the applications for clinical laser medicine and surgery took off exponentially and is still rising.
Prior to the mid-1990s, dermabrasion and chemical peels were the accepted means of skin resurfacing. Light and medium chemical peels could improve pigment problems and minor skin wrinkles. More aggressive peels used for “skin leveling” was predictable in the hands of experts but often led to significant hypopigmentation. Dermabrasion, an art in itself, was difficult to master in the hands of the average clinician. In addition, the spray of blood, serum, and tissue made this procedure especially unsavory in a time when blood-borne transmittable diseases were on the rise. The cosmetic world longed for a more controlled means of rejuvenating facial skin, and laser science had progressed just at the right time to fill this gap.
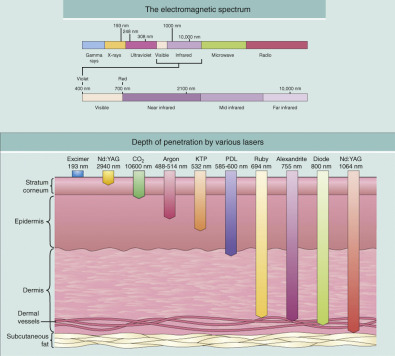
The acronym “LASER” stands for Light Amplification by Stimulated Emission of Radiation. Laser technology in medicine existed decades before it became popular but problems existed with the ability to ablate unwanted tissue without damaging surrounding normal tissue. With the improvement of technology and the understanding of photoscience and tissue response, lasers became a versatile treatment option. The basic principle of laser therapy is known as “selective photothermolysis,” in which the chromophore is targeted with a pulse duration that is shorter than the thermal relaxation time, thus minimizing risks of unwanted surrounding tissue damage. The development of the CO 2 laser (a wavelength of 10,600 nm) was initially used for surgical excisions but eventually was refined as a useful tool for skin rejuvenation and surgical incisions ( Fig. 13.1 ). The CO 2 laser produces tissue ablation and collagen shrinkage and is used to treat scarring, dyschromias, actinic cheilitis, rhytids, and numerous lesions. While the previous technologies of dermabrasion and chemical peel were “an experienced guess” at tissue depth, the CO 2 laser is an instrument that can precisely ablate tissue at predictable depths. The CO 2 laser can ablate 50–150 microns (µm) of tissue with a zone of thermal damage up to 100 µm. The chromophore for CO 2 laser is tissue water and the laser energy is also absorbed by surrounding vessels and structures for unselective tissue destruction. This is different for other lasers that have chromophores of melanin or hemoglobin and are much more specific as to the tissue target. The earlier CO 2 lasers were continuous wave in nature and more difficult to control lateral tissue damage. With the advent of ultrapulsed lasers and computerized pattern generators, high-peak powers and short-pulse duration were possible in which tissue vaporization was maximized and thermal injury minimized. Laser treatment rejuvenates the skin by several actions. First, it vaporizes the epidermis and superficial dermis. This in and of itself is like stripping old wallpaper or pulling up old carpet. When the new skin reepithelializes, the patient has youthful skin in the place of the damaged skin. Also, the thermal effect on the dermis creates neocollagenesis. The new and more plentiful collagen also firms and rejuvenates the skin.
With the availability of this powerful technology, the entire world set loose in pioneering skin resurfacing techniques. As happens when new technology is introduced, much of the learning curve must be mastered by trial and error. Unlike today where relative “cookbook” laser settings and “smart screens” with autoprogrammable treatment settings exist, the early days of laser treatment were less controlled. Unfortunately, many lessons were learned the hard way and an onslaught of complications occurred in the 1990s. Learning from the past, today’s contemporary CO 2 laser surgeons can offer safer and more predictable treatments. One disheartening note is that we are seeing a resurgence of similar complications from surgeons trying to push the envelope of fractional lasers in an effort to equate results with traditional CO 2 resurfacing.
In concert with progressing technology, many types of lasers were introduced to compete with CO 2 technology. The Erbium : YAG laser with a wavelength of 2940 nm became popular in the mid-1990s as a “safer and gentler” laser. This wavelength has a 13-fold greater affinity for water, of which the skin is about 70%. The stated advantages included less ablation depth, less thermal damage, faster healing, and decreased erythema persistence. Although this laser grew quickly in popularity after the Food and Drug Administration (FDA) approval in 1996, many of the same problems and complications associated with CO 2 lasers appeared soon after. Although the Erbium : YAG laser is still popular with some clinicians, the CO 2 laser is still the gold standard for skin rejuvenation, especially skin tightening and rhytid effacement. Some clinicians feel that “old school” traditional CO 2 treatment has been usurped by fractional laser treatments but I disagree. Although the healing may be faster, the treatment is much less dramatic and requires multiple sessions. Ardent proponents of fractional lasers decry the 12–14 days of recovery required for CO 2 laser but perform 3–5 sessions of fractional treatments that require 3–5 days of recovery each time. The math simply does not add up. Although I understand that some patients simply cannot miss 2 weeks of work or play, repeating any procedure 3–5 times actually has more recovery. I also feel that the popularity of fractional laser is driven less by result and more by the fact that it can be sold to a far larger number of doctors than CO 2 lasers. The reason for this is that the average laser surgeon frequently does not have the training to perform sedation or has access to general anesthesia. Fractional laser can be performed on awake patients (although I think all laser patients and surgeons do better with sedation) and because of this, companies can sell more lasers to a more diverse doctor base. Fractional treatments are also easily delegated to physician extenders. It is “all around” easier, but in my experience is a compromise of the results obtainable from traditional CO 2 laser treatment. Having opined on this, it is fair to say that any laser technology that enables satisfactory, reproducible results on happy patients with low complications is a good platform. Fractional lasers are available in ablative and non-ablative platforms. Ablative resurfacing literally vaporizes the tissue and removes it. Non-ablative laser treatment damages or kills the cells without vaporizing them.
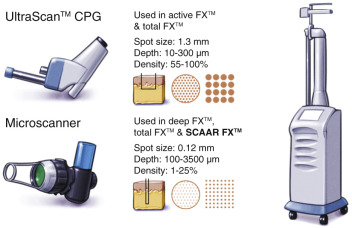
Although I have used all of the popular types of resurfacing lasers, the majority of my treatments have been with the Lumenis Ultrapulse Encore laser (Lumenis Inc., Santa Clara, CA), in the performance of a wide array of treatment depths from superficial fractional to ultra-deep ( Fig. 13.2 ). The Lumenis Encore CO 2 laser has a peak output of 60 watts and at 600 Hz with 100 mJ setting will produce a fluence of 7.5 J/cm 2 . The laser is equipped with a computerized pattern generator for skin resurfacing as well as straight handpieces for lesion removal and tissue incision ( Fig. 13.3 ). Currently, several options are available with the Encore laser, including a curved laser wave guide that can be used for endoscopic brow and forehead lift and a computerized scanner for deeper fractional treatments (Deep FX and SCAAR FX) for newer technology deep fractional scar treatments.


I also have experience with the Ellman Cortex CO 2 laser ( Fig. 13.2B ). This is a very affordable and versatile system. The CO 2 component is exclusively fractional but can be used more aggressively by performing multiple passes on the skin. Technically, when additional passes are performed with a fractional laser, the treatment is technically not necessarily fractional as the intact bridges of skin between the treated columns are also lasered, making it full (or fuller) coverage. I have used this laser with the fractional mode and with multiple overlapping passes with good results. This laser also has an incisional handpiece for blepharoplasty surgery or lesion ablation. An appreciable bonus of the Ellman Cortex laser is the Erbium handpiece. This comes with the laser and is a great option for very superficial resurfacing and treatment of superficial skin lesions such as dyschromias. The Erbium handpiece on this laser is single spot only (with several screw-on treatment heads to adjust size) but has a 5-mm spot size, which makes coverage efficient.
Patient Selection
As with any cosmetic procedure, proper patient selection is the key to obtaining ideal results. Lighter skin types have the potential for more predictable skin resurfacing and fewer pigmentation problems. Although many skin classification systems exist, the Fitzpatrick system is the most widely used ( Table 13.1 ). This system is derived from skin response to sunlight and generalizations with hair and eye color and amount of melanin ( Fig. 13.4 ).
| Skin type | Skin color and characteristics |
|---|---|
| Ivory white | Always burns, never tans |
| White | Usually burns, tans minimally |
| White | Burns moderately, tans moderately |
| Beige/light brown | Burns minimally, tans easily |
| Moderate brown | Rarely burns, tans profusely |
| Dark brown/black | Never burns, tans profusely |

The basis of the Fitzpatrick classification include:
- •
Type I – fair-skinned redheads (always burn, never tan)
- •
Type II – blue-eyed blondes (usually burn, tan with difficulty)
- •
Type III – dark-haired, brown-eyed patients (sometimes burn, slowly tan)
- •
Type IV – Asians, Hispanics, and light-skinned African-Americans (rarely burn, tan easily)
- •
Type V – brown-skinned African-Americans (rarely burn, tan easily)
- •
Type VI – very dark-skinned African-Americans (never burn, tan fast).
There are very few distinct boundaries with skin classification, and overlap is frequent. Any skin classification system offers broad commonalities, not sole determinants.
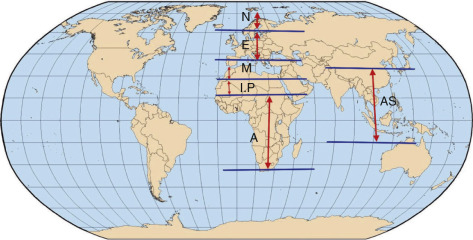
Whereas the Fitzpatrick system is relatively straightforward, looking at the larger picture of who we are and where we came from intensifies our understanding of skin types. The Fanous classification of skin type is based on racial origins and puts a logical understanding behind numbers ( Fig. 13.5 ). Our reaction to the sun (and laser) is ultimately related to our ancestral origins.
In treating various skin types, surgeons should keep in mind that the darker a patient’s skin is, the more potential problems can exist with peel or laser, especially hyper- or hypopigmentation ( Fig. 13.6 ). The very light skin types and the darkest skin types are the most stable for resurfacing; the mixed browns are the most problematic in terms of pigmentation difficulties. Referred to as global skin , this type should always be approached with caution when using peels and lasers. The best patients for the novice resurfacing surgeon are Fitzpatrick I and II skin types. Type III and above should be reserved for more experienced surgeons. Most doctors do not routinely laser dark skin and default to chemical peel for these patients. Fractional laser resurfacing is used with caution on select cases ( Fig. 13.7 ). Laser surgeons must keep in mind that they can make a patient permanently lighter or darker. Anticipating a patient’s skin response to resurfacing is in part based on their skin type and amount of melanin, as well as the depth of the melanin. Computerized skin scanning systems are very useful for diagnosis and patient education ( Fig. 13.8 ). Similar to placing a patient under ultraviolet light, the filters on the scanning systems enhance epidermal melanin ( Fig. 13.9 ). This means that superficial pigment will show up dark and deep pigment will not be as dark. When pigmentation is extremely dark and noticeably obvious, it is superficial and will most likely respond well to medium-depth dermal peels and lasers. If the pigment does not enhance and darken on the scan, it is likely deeper dermal pigment and may not improve with peels and lasers.




Since many patients do not “see” their actual sun damage, patients seeing the extent for the first time can become very motivated to begin skincare regimens. These scanners are also a valuable tool to illustrate the before and after improvement of resurfacing procedures.
Resurfacing Contraindications
Numerous contraindications exist for both peel and laser resurfacing. History of hypertrophic or keloid scar, poor healing, and active conditions such as severe rosacea or acne may complicate skin resurfacing. Some skin diseases such vitiligo, lichen planus, psoriasis, and verrucae can spread to traumatized skin, which is known as Koebner’s phenomenon. Peel or laser resurfacing can induce this problem on the treated face and neck areas. A patient with somatic vitiligo who underwent facial resurfacing could possibly have vitiligo pigmentation changes on the lasered facial skin.
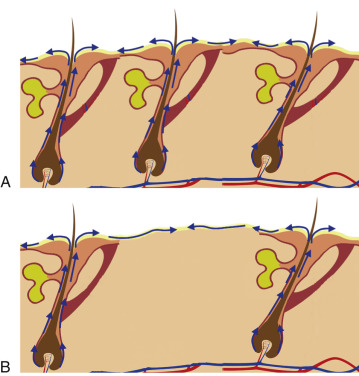
After the epithelium is destroyed by chemical agents or light sources, it must regenerate, or a full-thickness burn scar will result. Reepithelialization occurs from the base of the pilosebaceous units, and the presence of the hair/sebaceous gland unit is directly related to how much and how quickly the new epithelium regenerates. In a process known as epiboly , the pilosebaceous units serve as the progenitors of new epithelium. New epidermal cells migrate from the base of the pilosebaceous unit, progress up the hair shaft, then spread laterally on the injured skin surface ( Fig. 13.10 ). Areas of the body that are heavily populated with pilosebaceous units have a better chance of more rapid epithelialization. The face has 30 times the pilosebaceous units as the neck or chest and 40 times the number on the dorsal arms and hands. For this reason, deeper peeling and laser treatment can be performed on the face, whereas the same treatment on the neck or extremities can lead to disastrous scarring. Areas heavily populated with hair follicles heal faster; with low hair-bearing areas, the epithelial cells simply have too far to travel and scarring can result.
The most sincere words of wisdom to surgeons just beginning skin resurfacing is to always respect the neck (and nonfacial skin), and never treat it in an aggressive manner. I have served as an expert defense witness for several surgeons who caused significant scarring by peeling or lasering the neck. I have also had my own misadventures in this region but luckily without permanent scarring. I learned to respect the neck early on in my experience and always pass this on to all beginners. I have had my most sleepless nights worrying about resurfacing patients. Experienced surgeons will understand this statement.
Understanding the importance of pilosebaceous units and healing, any procedure or medication that affects or suppresses the pilosebaceous units could compromise healing and produce scarring. The mechanism of action of systemic retinoids such as isotretinoin (Accutane) is suppression of the pilosebaceous units, which would affect reepithelialization after skin resurfacing by peel or laser. Most authorities recommend waiting at least 1 year after Accutane therapy before laser resurfacing (6 months for medium-depth chemical peel). Radiation therapy can also destroy pilosebaceous units, and patients who have received therapeutic radiation can be problematic healers. Other relative contraindications can include history of keloid or hypertrophic scarring, history of severe herpetic outbreak, or a history of excessive lower-eyelid skin removal. Patients with collagen vascular diseases such as lupus or scleroderma may have impaired healing mechanisms and could affect healing.
Whereas preconditioning with tretinoin or bleaching agents is critical for chemical peeling to allow even penetration of acid, many practitioners do not precondition laser patients. In my opinion, patients with the potential for post-inflammatory hyperpigmentation (PIH) will heal with fewer problems if they undergo 2–6 weeks of skin conditioning with Retin-A and hydroquinone 4%.
Laser skin resurfacing (LSR) is very effective for skin tightening, textural improvement, and the effacement of wrinkles. In my experience, the degree of both is far superior to a single medium-depth chemical peel. Having said that, the recovery with LSR is much more complex and will be discussed in detail. When discussing LSR with potential patients, the surgeon and patient must decide which type of CO 2 laser treatment is applicable to their degree of skin damage and their recovery window. With the Lumenis Encore platform, numerous types of treatments can be performed, including ultralight fractional, light, medium, deep fractional, and aggressive high energy and high density (traditional resurfacing). Each type of increase in treatment depth has increasingly noticeable results and extended recoveries. Aggressive CO 2 resurfacing can be a formidable recovery process and not all patients (especially younger ones) will accept that extreme.
Personally, I believe the standard of care for full face LSR of any type (fractional or full coverage) includes pre-treating patients with antibiotics and antivirals. I place all full face laser patients on a cephalosporin such as cephalexin 500 mg every 6 h. I begin the treatment the day before the procedure and continue it for the first week post-laser. The same regimen is used with antivirals with 500 mg of valacyclovir every 12 h beginning the day before surgery. There are no absolute studies that show either medication is a requisite but all doctors must blend evidence-based practices with legal precedents. I know surgeons who never use antibiotics with laser treatment and say their infection rate is no greater than when they do use them.
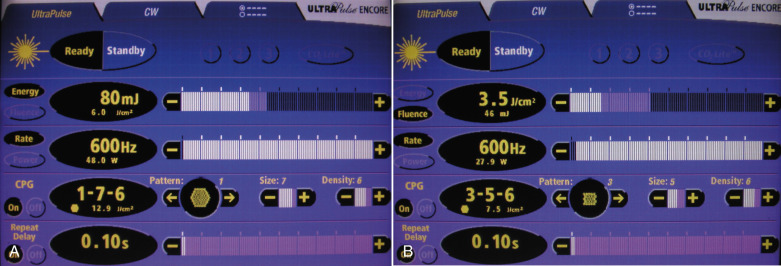
When discussing laser parameters, it is important for surgeons to understand the physics and nomenclature for laser therapy. Simply stated, fluence is the amount of energy received by a surface per unit area, which is usually expressed in joules per centimeter squared (J/cm 2 ). This can vary due to laser spot size and wattage of the laser. Density is the measurement of the amount of overlap from the computerized pattern generator. Fractional laser density is low and has no overlap, while traditional full coverage laser patterns have overlap of laser beam spots of 30% and beyond. Some lasers have a setting for hertz, which is a measure of cycles per second of the laser beam, or how fast they are generated. Passes indicate the number of times a given area of skin is treated over the top of the previous pass. A “3 pass” laser treatment would mean that a single pass was made over the entire region and repeated again for a second pass and again for a third pass. This would be analogous to painting a wall with three coats of paint. Combining these variables produces the wounding depth, thermal damage, healing, and results of the laser treatment. A high-fluence pass (7.5 J/cm 2 ) with a high density (30% overlap of laser beam spots) and 3 passes would be a very aggressive treatment, while a lighter treatment may be a single pass of a fluence of 3.5 J/cm 2 with a density of 1 (no overlap) ( Fig. 13.11 ). There are no standardized parameters from one laser to another but an understanding of fluence, density, and passes can be applied to all laser treatments for reproducible results. Increasing any of these parameters (while leaving the others the same) will result in deeper treatment. Expert laser clinicians can apply the physics of lasers with the clinical treatments and outcomes for safety and maximum result. Novice laser surgeons must remember that lasers are serious devices capable of drastic burns and scars.
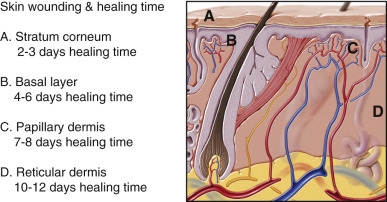
Laser treatment (or any resurfacing such as chemical peel or dermabrasion) is personalized for each patient based upon their age, amount of skin damage, pathology of the damaged skin, thickness and quality of skin, and many other parameters. In general, light to moderate skin damage requires superficial laser, while moderate to severe damage requires deeper treatment. The target and endpoint for each patient is variable. For minor pigmentation, a basal layer treatment may be adequate; for deeper pigment and fine lines and wrinkles, the skin wounding must extend into the papillary dermis; and for the deepest skin damage, the laser must extend into the reticular dermis. Deep dermal treatment can cross a danger line and if the treatment extends into the adnexa (hair follicles, sebaceous and sweat glands) permanent scarring can result. The laser surgeon must remember that he or she is creating a large-surface second degree burn of the entire face, which is about 5% of body surface area and it must be managed with great care.
The laser operator should have a firm understanding of the amount of skin damage of the each patient and the depth of wounding of the proposed treatment. Beginners should only begin with mild to moderate treatments and progress with experience. Although it is difficult to truly measure the penetration of the laser burn and related thermal damage, it can be generalized by understanding the tissue layers of the skin and relative depth of penetration of the specific laser. Most lasers can predictably remove 50–100 µm of skin in a single pass. The second pass may remove a similar amount of skin or have a little less penetration due to desiccation of the skin after the first laser pass. Also important and directly related to the depth of treatment is the time required for reepithelialization after laser treatment. A basal layer treatment will heal in 4–6 days, while a reticular dermal treatment will take up to 2 weeks to heal. Wounds that take longer than 2 weeks to reepithelialize may heal with full-thickness scarring. Fig. 13.12 shows tissue anatomy of the skin, as well as the time required for reepithelialization after laser treatment.
For the purposes of this text, CO 2 laser treatments will be classified into the following categories. Some of this nomenclature is specific for the Lumenis Encore CO 2 laser.
- •
Ultralight Fractional CO 2 LSR . This is also referred to as Active FX with the Lumenis platform and involves high-fluence, low-density fractional treatment. The Fraxel Repair platform is a 1550-nm Erbium laser source from another company (Solta Medical, Hayward, CA).
- •
Deep Fractional LSR . Also called “Deep FX” on the Lumenis platform, involves high-fluence, low-density, single-pass treatment with increased tissue penetration depths. The Fraxel Restore platform is used for similar applications and has a dual wavelength.
- •
Traditional (aggressive) CO 2 LSR . Also my nomenclature and involves full coverage, ablative, high-fluence, high-density, multipass treatment. This is, in my opinion, still the gold standard for facial resurfacing and scar improvement.
The above treatments are listed in increasing order of clinical result and recovery time. Whereas an ultralight CO 2 LSR may heal in 5 days, it produces minimal improvement; an aggressive, high-fluence, high-density, multipass CO 2 treatment can produce dramatic results but requires almost 2 weeks of recovery with another month of post-laser sequelae. Younger patients with few wrinkles and small pigmentary problems may benefit from a lighter (or fractional) laser, while older patients with significant photodamage, dyschromias, and wrinkles will require high-power aggressive treatment for rejuvenation. One of the keys to successful treatment is to couple the proper patients with the proper laser settings and communicate a realistic expectation of degree of improvement and recovery time.
Currently (and probably for eternity), there is an onslaught of laser promotion for increased results with decreased recovery. This is a good thing and is how cosmetic science progresses. The problem lies in the fact that laser companies and the media frequently distorts the actual results versus the recovery periods required. This is a very confusing time for novice laser surgeons, as so many of the currently available fractional lasers sound too good to be true. As laser manufacturer competition has become more competitive, many surgeons are offered lasers that have downtimes of several days and have results that are amazing. Unfortunately, often the expectations exceed the results. I have numerous colleagues who have purchased “miracle” lasers that purport maximum results with several days of downtime, only to be extremely disappointed. Some surgeons are even told that “you can’t hurt anyone with this laser,” which is a travesty. It takes years of experience to master LSR and every practitioner should devote significant study, preceptorships, and proctoring to learn the skill. Similar to chemical peeling, performing less aggressive procedures on a long series of patients is the best way to become competent and have reproducible and safe results.
Laser Safety
Laser treatment can be very hazardous to the surgeon, staff, and patient. Numerous potential hazards exist. Every office should have a laser safety officer, that is, a staff member that enforces and documents safety measures to protect the surgeon, patient, and staff. Any time that a laser is active, any interior windows in the operating room must be covered and a sign must be displayed on the door that a laser is in use and the specific wavelength named ( Fig. e13.1 ![]() ). This is protection for anyone that may gaze through the window or wander into the room when a wavelength is in use that can produce retinal damage.
). This is protection for anyone that may gaze through the window or wander into the room when a wavelength is in use that can produce retinal damage.
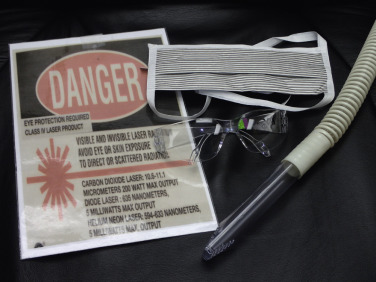
Eye protection is paramount for the surgeon, staff, and patient. The CO 2 laser technically does not require protective eye wear for the doctor and staff, as it is not a visible light output or one that can damage the retina from direct unprotected vision. Eye protection must still be used, however, in the event that the laser beam reflects off an object into someone’s eyes in the room. The reflected beam can produce the same incision or ablation of the cornea that it does on the skin. Remember, laser light bounces off shiny surfaces and for this reason, most stainless steel laser instrumentation and eye shields have a flat, dull finish.
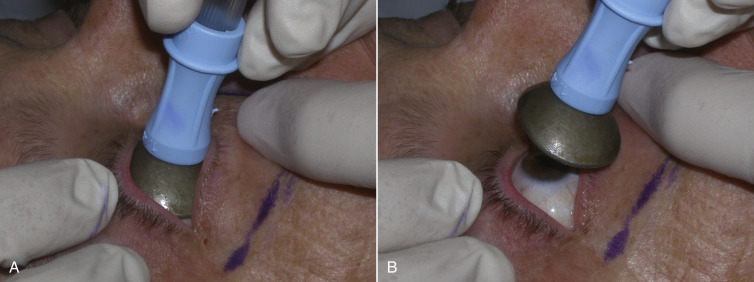
Placement of corneal shields is an absolute requisite when using lasers on the face, as serious eye damage has occurred by inadvertent laser contact ( Fig. 13.13 ). The placement of corneal shields is very simple. Several drops of commonly used local anesthesia (with or without epinephrine) are instilled in each eye and the stainless steel polished corneal shields are placed in the fornix of the lids, with suction cup holders ( Fig. 13.14 ). Dedicated topical ophthalmic anesthetic drops can be used as well. Although some surgeons lubricate the shields with an ophthalmic ointment, I have abandoned this, as it seemed to produce more irritation. At the end of the procedures, the shields are removed and the eyes are irrigated with saline solution. Some patients have larger or smaller palpebral apertures and this may require multiple size shields. In the event that swelling makes the removal of a shield difficult, a wall suction hose tip can better grip the shield for removal ( Fig. 13.15 ).


Vaporized particulate inhalants are another potential laser hazard and the smoke plume must be controlled. Everyone in the room must wear a facemask, and dedicated fine-pore laser masks are preferable. These masks are thicker, filter smaller particles, and have an extended area of coverage to protect the personnel from laser smoke plume. A dedicated smoke evacuator is also a necessity when using ablative lasers ( Fig. 13.16 ).
The CO 2 laser beam is also an ignition source and must not be used in the presence of confined oxygen, as operating room fires can occur. This is especially important when working around endotracheal tubes or nasal cannulas, as they can readily ignite ( Fig. e13.2 ![]() ). The situation becomes more critical if closed drapes are used around the head, which confines the oxygen. Besides the fire risk, the patient and their airway can be severely burned. Any flammable material such as paper or cloth drapes, hair, plastic etc. must also be kept out of the path of the laser beam. Patients should never have hair spray or hair gel on during ablative laser surgery. Some surgeons state that if a patient is prepped with Betadine (povidone iodine) that it should be removed with a wet gauze prior to lasering. The reason for this is that burning the dried iodine solution on the skin can release elemental iodine with the plume and that is worth considering.
). The situation becomes more critical if closed drapes are used around the head, which confines the oxygen. Besides the fire risk, the patient and their airway can be severely burned. Any flammable material such as paper or cloth drapes, hair, plastic etc. must also be kept out of the path of the laser beam. Patients should never have hair spray or hair gel on during ablative laser surgery. Some surgeons state that if a patient is prepped with Betadine (povidone iodine) that it should be removed with a wet gauze prior to lasering. The reason for this is that burning the dried iodine solution on the skin can release elemental iodine with the plume and that is worth considering.

CO 2 Laser Treatment Options
There is a multitude of lasers with a multitude of wavelengths available for cosmetic treatments. Some have been around for decades and many have come and gone. This chapter focuses on the laser treatments that I have performed in my practice. I have performed thousands of the various described traditional CO 2 laser treatments. Although I have two fractional lasers, this therapy is not a major part of my practice. Traditional full coverage, ablative LSR with intravenous (IV) sedation still remains the mainstay of my practice. The recovery is longer but the results are impressive and can always be seen in before and after pictures. Ultralight laser treatment is fine for removing superficial pigment but is much less effective for deep wrinkles and skin tightening to the degree available with traditional CO 2 LSR.
Ultralight CO 2 Fractional Laser Skin Resurfacing
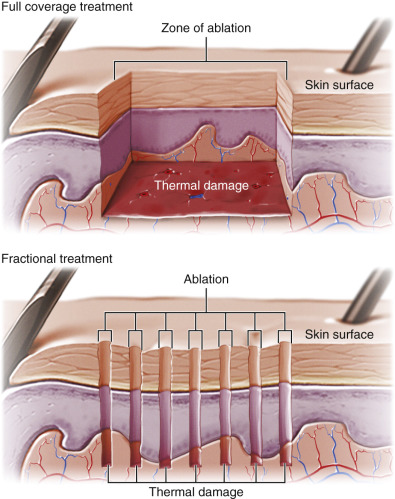
It is imperative to understand the difference between full coverage and fractional laser treatment. Full coverage treatment is traditional laser treatment where the computer pattern generator treats the entire skin surface with overlapping laser pulses ( Fig. 13.17 ). Fractional treatment, on the other hand, does not cover the entire skin surface but rather produces spaced laser spots in an orderly fashion. These ablated columns are separated by unlasered normal skin. Since the entire skin surface is not treated, reepithelialization and healing progress faster with fractional treatment. This can be explained to patients in a simplified fashion that full coverage treatment is like painting with a paint roller and fractional treatment is like painting polka dots. With the Lumenis laser platform, superficial fractional LSR is called “Active FX” and is performed on the face with a high fluence such as 100 J/cm 2 and a density of 2. This allows high power but no overlap, hence it is fractional. Fig. 13.18 shows the clinical appearance of full coverage and fractional laser treatment.

This level of fractional laser treatment is moderately effective for dyschromias and very fine lines and wrinkles. The treatment is beneficial for skin health and will produce a refreshed and smoother skin surface. Although a single CO 2 fractional treatment can produce benefit, multiple treatments are more effective and almost always required. I use this treatment rarely because most patients in my practice have greater levels of skin damage and/or expect more dramatic results. For patients that desire a mild to moderate improvement with a shorter downtime, this is an option but requires multiple treatments for maximum result.
As discussed previously, resurfacing the neck is a dangerous procedure that can produce severe complications. For this reason, I never use high-energy, high-density (traditional) laser treatment on the neck, but the Active FX superficial treatment has proven very safe ( Fig. 13.19 ). A single treatment does not produce significant results, but does produce a smoother feeling skin surface. Repeated fractional CO 2 laser neck treatments can produce mild to moderate improvement of dyschromias and photodamage. The neck will never respond to laser rejuvenation as well as the face, and scarring risk is high.

Deep Fractional Laser Skin Resurfacing
The Deep FX (Lumenis, Inc.) is a fractional, ablative CO 2 laser with a spot size of 0.12 mm, which is much smaller than a standard laser ( Fig. 13.20 ). Due to the small spot size and the ability to deliver high power (10–20 mJ), this laser penetrates much deeper into the skin. The ablation depth relates to the energy level, where a 10-mJ single pulse can penetrate 230 µm, a 20-mJ pulse can penetrate three-fourths of a millimeter. This burns deep into the dermis to a depth of 450 µm plus an additional 300 µm of lateral thermal damage for a total of 700 µm, which is well into the reticular dermis (the full coverage, ablative CO 2 laser penetrates 100–300 µm). Since this laser penetrates deeper, bleeding is common ( Fig. 13.21 ). After the Deep FX treatment, a single pass of Active FX treatment is usually performed, which cauterizes the bleeding and blends the treatment. The fractionated nature of the laser coupled with its depth of penetration separates deep fractional LSR from traditional LSR. The main drive for this type of treatment is significant clinical improvement of the skin with decreased healing time. The healing time with this type of resurfacing is shorter but to date, the degree of clinical improvement does not correlate with traditional full coverage, high-energy, multipass, ablative CO 2 LSR.

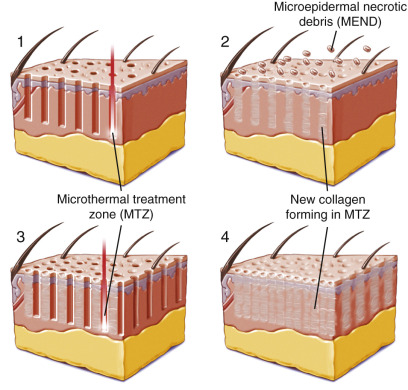
The Fraxel Dual Repair laser (Valeant Pharmaceuticals, Bridgewater, NJ) is a nonablative laser and has also become a popular option for reduced recovery LSR ( Fig. e13.3 ![]() ). This nonablative platform utilizes a 1550 nm Erbium-doped fiber laser combined with a 1927-nm wavelength that produces micro-column ablation. Solta Medical also produces a platform called Fraxel Repair, which is an ablative CO 2 laser. These localized columns of thermally denatured collagen stimulate collagen remodeling while leaving islands of intact dermal and epidermal cells, which in turn leads to speedy epithelial recovery, thereby minimizing downtime ( Fig. 13.22 ).
). This nonablative platform utilizes a 1550 nm Erbium-doped fiber laser combined with a 1927-nm wavelength that produces micro-column ablation. Solta Medical also produces a platform called Fraxel Repair, which is an ablative CO 2 laser. These localized columns of thermally denatured collagen stimulate collagen remodeling while leaving islands of intact dermal and epidermal cells, which in turn leads to speedy epithelial recovery, thereby minimizing downtime ( Fig. 13.22 ).

While fractional technology is an advance, these lasers have not achieved the gold standard results of conventional, aggressive, high-energy, multipass CO 2 LSR. To achieve significant results, the fractional laser treatments must be repeated 3–5 times. The decision to forgo a conventional CO 2 procedure with healing at 12 days for 3–5 treatments of fractional laser, which require 3–5 days of recovery each time is not a huge advantage in my mind.
There are many case reports in the literature of complications from fractional lasers. This laser, which was designed as a single-pass light treatment, has been pushed by many practitioners to use with multiple passes and higher settings to improve treatment results. This underlines the fact that there is no such thing as a “safe” laser.
“Traditional” CO 2 Laser Skin Resurfacing
A wordy but accurate description of a conventional LSR is: ablative, full coverage, multipass, high-energy, high-density CO 2 laser skin resurfacing. I call this the “traditional” LSR, as this was the initial format for laser treatment with the introduction of ultrapulsed CO 2 lasers. The CO 2 laser has been one of the greatest advances in cosmetic surgical science. It, for the first time, allowed precision ablation of skin at controlled and predictable depths. This changed the face (no pun intended) of cosmetic surgery and ushered in new technologies. The biggest advantage of the CO 2 laser is its ability to efface rhytids, remove dyschromias, tighten skin, and make new collagen. The biggest disadvantage is a formidable and extended recovery. In addition, largely due to the misuse of this laser in its early days, numerous complications have been associated with its use. Since 1996, I have used this laser as a mainstay for facial rejuvenation and scar treatment and, despite the blitz of “new” lasers and laser technology, it remains my primary and preferred skin resurfacing treatment.
Suitability of patients for traditional resurfacing runs the gamut of skin damage and age groups. There is no one single treatment with this technology, as the treatment is tailored by manipulating the energy and density of overlap. Some patients are treated with a single pass at a lower energy (3.0 J/cm 2 ), while others are treated with three or more passes with a fluence 7.5 J/cm 2 depending upon the degree of damage and skin type. I only perform aggressive LSR on Fitzpatrick I–III skin types and never use it on darker skin types (where I may use fractional laser). I have performed numerous full face laser cases and feel that it is a predictable treatment and I have taken numerous steps to mitigate the infamous CO 2 laser recovery, discussed later.
Traditional treatment can be extremely dramatic in the improvement of photodamage, skin wrinkling, and scars. Having said that, it is not a treatment applicable to every patient as the recovery is complex. The prospective patient must understand the actual procedure and recovery. The laser will remove the entire epidermis and extend to the dermis in aggressive (high-fluence and -density, multiple-pass) treatments. The patient must understand that they will have a second degree burn and a raw face for the first 7–10 days. They must further understand that into the second post-laser week their face will be very pink and the pinkness will resolve with time. Some patients may have erythema resolution in 2–3 weeks, while others may require 3–4 months. Although erythema lasting months is not the norm, the informed consent process must detail “exceptions to the rule,” as they can and will occur. This is less of a problem in females who can readily cover the erythema with makeup but more problematic for males. Newly regenerated epidermis is fragile and reactive and will frequently develop PIH. Regardless of how well this is explained in the pre-laser informed consent process, patients find this very disconcerting. The best means I have of preparing patients, is to use a series of YouTube videos that I recorded, which discuss treatment, post-laser care, and sequelae in depth. Having these laser instructions online has greatly simplified our communication and lowered the number of after-hours calls. In the consideration of patient selection, aggressive CO 2 LSR is not for timid or impatient patients. I actually tell my laser patients that they “will not like me for 5–6 days” but in the end, they will be very happy. I have had this treatment myself and can testify that the actual recovery process is not extremely painful but the swelling, oozing, and greasy face are unpleasant. All of this coupled with staying in the house for 10 days is what wears on the patient. Most patients say that it was not as bad as I made it sound, but I am always forthright when discussing recovery.
Explaining the need for touchup procedures is also important with any LSR procedure. The skin can only be safely treated to a given extent at a single treatment, and patients with severe wrinkling or scarring must understand that they will see improvement but may require additional treatments to obtain optimum results. This may include repeating the entire facial procedure or just re-treating the areas of deepest damage. It is not uncommon for me to perform a full face treatment and then 90 days later re-treat the perioral or periorbital regions or whatever areas that can be improved. All acne or scar patients must realize that numerous treatments are the norm and not the exception. So much media and corporate hype exists in terms of the degree of anticipated rejuvenation that patients may present with impossible expectations and must be educated on the reality. Under-selling a recovery or over-selling a result is an excellent way for a surgeon to lose patients and develop an undependable reputation. The time of year can also influence treatment. Laser and chemical peel patients must avoid direct sunlight for at least 1 month. In the summer, this is impossible for some patients and therefore they are not good hot weather candidates. Winter months (in locales that have them) are usually more preferable times for laser recovery. Sunlight also accelerates PIH and it is much harder to avoid the sun in the summer.
Considerable wound treatment is required in the first weeks of traditional LSR and unmotivated or noncompliant patients can severely complicate recovery. All of this must be covered in the LSR consent, including what the treatment is, what the patient will look like and for how long, how the patient’s compliance can improve the outcome, and how to avoid complications. The need for multiple treatment sessions must also be covered in the consent, as should lack of treatment guarantee and pigmentation complications.
For traditional CO 2 LSR, the preoperative checklist should include medical and anesthetic considerations, appropriate medications, skincare, healing products, and sun protection. Pre-laser photographs are taken of all patients without makeup and a skin scan is also performed. It is really important that the patient has purchased all of their post-laser skincare products before surgery and they and their caretaker understand how to use them. Patient wound care can greatly simplify or complicate recovery and result.
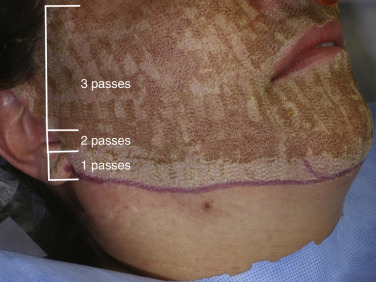
Immediately before the procedure, the transition zone or endpoint of the laser extension is marked at the inferior border of the mandible ( Fig. 13.23 ). It is important to blend the treated skin into the terminal treatment zone to avoid a visible demarcation above or below the jawline ( Fig. 13.24 ). Any regions of deeper wrinkles or scars are also marked with a surgical marker to alert the surgeon for more aggressive treatment. Similarly, any regions that need lighter treatment are also marked.

With the rare exception of superficial fractional treatment, I only perform laser resurfacing with IV sedation or general anesthesia. Some practitioners utilize facial blocks and oral sedatives, but a fully anesthetized patient makes for a faster procedure, and one that is much easier on both the patient and the surgeon. All the common laser safety checks are made and the corneal eye shields are inserted as described.
In terms of laser settings, novice surgeons must be careful when using “cookbook” settings published by laser companies or other operators. Although these may be reference points, they can vary dramatically from company to company and laser to laser. Settings are also influenced by such variables as power, spot size, degree of overlap, and pulse settings. In actuality, there is no substitute to hands-on training and surgeons should slowly and carefully progress from light laser treatments to the more aggressive treatments. The insight gained in the first-hand observation of intra- and post-laser treatment and healing is invaluable for safe and effective treatments. Always remember, just because some other surgeon uses a given group of settings on his or her patients it may not work in inexperienced hands and could be disastrous in terms of complications. Laser complications are a heavily litigated area of cosmetic facial surgery. With experience, laser surgeons can judge treatment endpoints of the appearance and response of the treated skin.
I do not treat aesthetic subunits without full face coverage, with the exception of the periorbital region, which, due to having thin skin and being recessed, does not stand out against unlasered skin. Some practitioners will routinely treat subunits and their patients are frequently left with white “mustaches” or nasolabial fold white lines from the change in texture and color when attempting to treat isolated aesthetic subunits. If I do have a request to treat significant perioral wrinkling and photodamage, I will treat this aggressively, but also treat the remainder of the face with appropriate settings to blend the entire treatment. If I treat a patient with a full face aggressive LSR and they return in 90 days for a touchup, I will, at the second treatment, laser isolated subunits such as the perioral region. This can be done because the initial full face procedure has homogenized the skin color and texture. With the exception of the periorbital region, this is my only indication to treat subunits and not the entire face. I will treat small scars or lesions as a subunit, but not traditional anatomic cosmetic units such as “just the cheeks” or “just the mouth or chin,” etc.
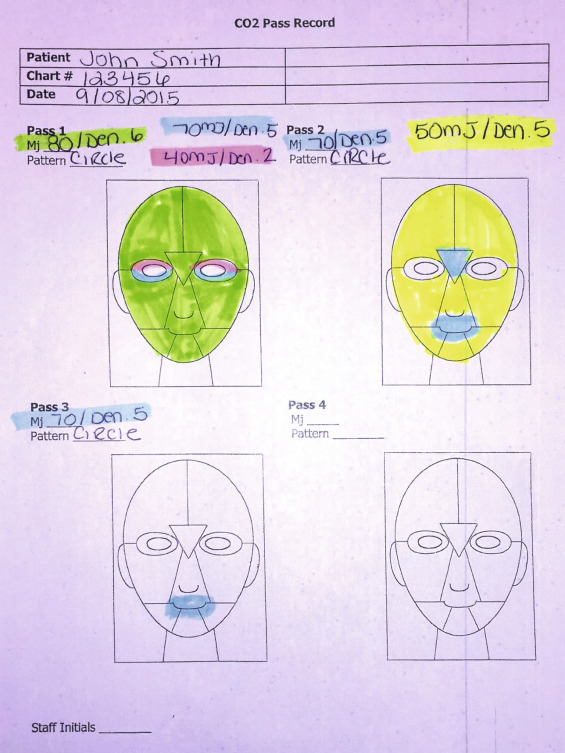
It is important to have a diagram of the face in the medical record and have the laser safety officer document the areas treated as the procedure progresses. This not only serves as part of the operative report, but prevents inadvertent under- or overtreatment. It is easy to lose track of the treated areas and the surgeon can mistakenly re-treat or undertreat a given area. It is helpful to develop a standardized treatment protocol and use it on all patients. An example would be doing the forehead first for a single pass, then going to the periorbital region, then to the cheeks, then the mouth, and finishing with the jawline. This is done for the single pass, and subsequent passes are made in the same order. This prevents making extra passes or forgetting to make an additional pass on an area. One of the laser team members should have the sole task of keeping track and recording the treated areas and making sure the intended treatments are made to all areas ( Fig. e13.4 ![]() ).
).
Laser Settings
It is impossible to list exact settings because of the vast variables of skin and laser parameters involved. Basic settings are published that are average for a given area, but should always be approached from the conservative side. With most lasers that employ computer pattern generators (CPG), the adjustable settings include power, density, pattern size, repeat rate, and number of passes. Each of these can produce more power in their own realm and much more when combined. For instance, a single pass of 50 J/cm 2 may not ablate the entire epidermis with a single firing of the CPG. Stacking the pulses, turning up the power, increasing the density or the repeat rate can all increase the thermal damage to that given area. As an example, with the Lumenis Encore laser for traditional full coverage ablative treatment, I begin with the following settings, depending upon the degree of damage: For full coverage (non-fractional) light treatment in the case of a 45-year-old female with minor wrinkles and moderate dyschromias, I would do a single pass of 3.5 J/cm 2 with a density of 6 (30% overlap). This would be done over the entire face including the upper and lower lids. This will ablate most of the epidermis and heal in 7 days. This treatment is similar to a medium-depth chemical peel. I have also used these settings with a single pass over forehead lift and facelift many times without any problems. If the patient has increased wrinkling (but not severe) or pigmentation, a second pass of the same settings could be performed over the entire face. When making the CPG passes, I prefer a large square or large circle pattern. It is important not to overlap or underlap the edges of the pattern, as this will be apparent as a lattice or checkerboard pattern during healing, and can be permanent ( Fig. 13.25 ). Lattice pattern is always important to avoid, especially in single-pass treatments. With multiple-pass treatments the second or third pass can fill in and blend the lattice, but in a single pass there is no blending.
As the previous settings were for minimal skin damage, the treatment parameters increase relative to the amount of elastosis, rhytidosis, and dyschromia. For the average patient, I generally perform 2–3 passes of a given setting. For a patient with moderate damage, 2 passes of 70 mJ with a density of 6 may be sufficient and would reepithelialize in about 10 days, with noticeable results. Often, a patient has increased damage in several areas such perioral, crow’s feet and glabella. These areas are marked preoperatively and may be lasered more aggressively than the rest of the face ( Fig. 13.26 ).

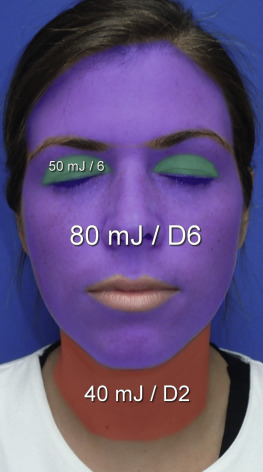
The vast majority of my LSR is on patients in their fifth and sixth decades with moderate to severe actinic damage with wrinkles and dyschromias. These patients are usually treated with 2–3 passes of high-fluence, high-density setting, and I may perform additional passes in the perioral region. The first pass (using the Lumenis Encore CO 2 laser) is routinely performed with 80 mJ and a density of 6. This excludes the upper lids, which are lasered at a lighter setting. The earlobes are routinely treated but the vermilion lips are not. The lower eyelid skin is treated with 2 passes of 80 mJ with a density of 6 in patients with significant dermatochalasis. In younger patients without significant eyelid skin changes, a single pass of 80 mJ and a density of 6 or 70 mJ and a density of 6 is used for a single pass will suffice. The upper lids when lasered are treated with a single pass of 50 mJ and a density of 5 or 6. Areas of other thin skin such as the temple and lateral canthal regions of females with very thin skin are also lasered at lower energy and/or density. As a reminder, all of the above settings are used with the Lumenis Encore CO 2 laser.
When lasering over deep rhytids it is helpful to stretch the skin so the laser beam can reach the base of the rhytids, otherwise the deeper portions will be missed. It is also important to extend the laser all the way to the hairlines to prevent noticeable demarcation.
In multipass LSR, the face is totally treated with a single pass before moving on to a second pass. This prevents pulse stacking, which is multiple firing of the laser over the same area, and allows the skin to cool before a second pass. Pulse stacking is never performed, as it does not allow the heat to dissipate and may cause deeper than intended tissue damage and result in overtreatment or scarring. In the evolution of laser treatment, the laser char was debrided after each pass ( Fig. 13.27 ). In a typical 3-pass treatment, the first laser pass is performed on the entire face, then the char is debrided with wet gauze until all the char is removed. A second pass is then performed and this char debrided, followed by a third pass, which is then debrided. The reasoning was that the char could serve as a heat sink and produce further thermal damage.

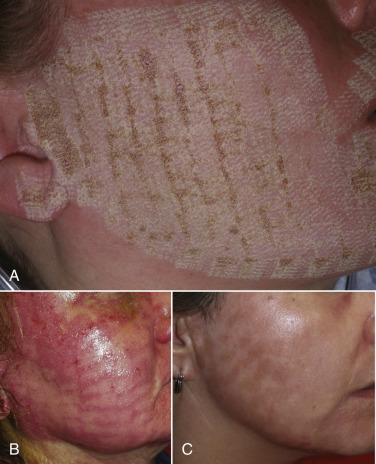
For the novice practitioner, successive debridement allows the judgment of clinical endpoints and is a good way to “learn” laser treatment, as the treated skin is continually visualized. Generally, laser treatment is halted when the skin reaches a chamois or champagne color. This is the endpoint of aggressive laser treatment and usually occurs after 3 passes but is variable ( Fig. 13.28 ). The treatment endpoint is difficult to judge without debriding the char.

For experienced operators, there are numerous advantages to not debride between passes. The development of LSR was intended to capitalize on the precise and predictable level of tissue ablation. Debriding the treated tissue with a moist gauze pad further injures the skin, adding mechanical trauma, and negates the precise ability to ablate tissue as originally intended with laser technology. This added trauma complicates recovery, increases post-laser pain and increases the duration of post-laser erythema.
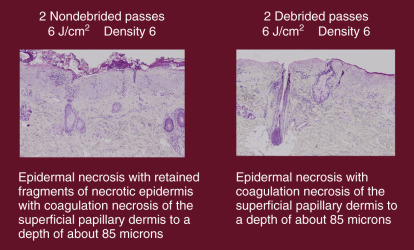
In 2008, I published the first human study showing that not debriding laser char between laser passes does not increase ablation depth or increase complications. This study involved split-face histologic examination after high-energy, high-density, and multipass CO 2 patients. One side was debrided after all passes and the other side was not debrided at all. These patients were followed clinically and histologically ( Figs. 13.29 , 13.30 ). The histologic analysis showed no difference in the ablation depth when debriding or not debriding. In addition, the undebrided eschar serves as a biologic dressing, which is more comfortable than denuded skin. Not abrading the raw skin with moist gauze also decreases postoperative discomfort and erythema. When the operator debrides after passes, the patient is essentially getting lasers plus dermabrasion, which increases the irritation. Not debriding also simplifies and shortens the laser procedure.

A summarization of my typical laser treatment is basically small, medium, and large in terms of treatment depth. The choice of small, medium, or large is mostly dependent on the amount of damage (wrinkles, dyschromias, and actinic damage) a patient has. For “small” laser treatment, I may perform fractional CO 2 treatment of a single pass. Most of my patients require a more aggressive treatment than this, however. For “medium” treatment, I may perform a single pass of lower power (40 mJ [3.0 J/cm 2 ]) with a density of 6, or possibly 2 passes. Still in the “medium” range, I may up the power to 70 mJ [5.3 J/cm 2 ] with a density of 5 and do 2 passes. For the “large” treatment, I most frequently perform 2–3 passes of 80 J/cm 2 [6 J/cm 2 ) with a density of 6 ( Fig. 13.31 ). Usually, 3 passes of this high power and density is the maximum I will do on the face and most frequently perform 2 passes unless the damage is severe. When I use this type of aggressive setting, I only do 2 passes on the lower lids and use less power on the upper lids. For severe perioral wrinkles, I may do a fourth or fifth pass. This level of treatment is reserved for very experienced laser operators. The above settings are those used with the Lumenis Encore platform.
When lasering the neck, I never use anything but a light fractional CO 2 laser such as Active FX for a single pass with a setting of 40 mJ and a density of 2 ( Fig. 13.32 ). The neck will never rejuvenate with the same result as facial skin for the reasons mentioned above. Pushing the envelope of neck treatment can be an invitation for disaster.

Lasering of Undermined Flaps
Laser resurfacing with simultaneous facelift is a procedure that I have performed hundreds of times without significant complication but it should only ever be attempted by surgeons with significant facelift and laser experience. The thin lipocutaneous facelift flap can easily be devitalized and drastic consequences can occur. When lasering facelift patients, I leave the LSR for the final step. Prior to lasering, the extent of undermining of the facelift flaps are marked ( Fig. 13.33 ). The central oval of the face is treated at normal settings with multiple passes of 80 mJ and a density of 6. The undermined lipocutaneous facelift flap is then carefully lasered (with great care not to overlap patterns) at 80 mJ but with a reduced density of 4 ( Fig. 13.34 ). This setting uses the same power but lowers the density. This can also be done by lowering the power and maintaining the density with a single pass of 60 mJ and a density of 6. The laser flap is never debrided. The CO 2 Lite setting of 3.5 J/cm 2 can also be safely used as a single pass over the undermined facelift flap. Again, this is not a procedure for novice facelift or laser surgeons. Fig. 13.35 shows a laser/facelift patient 2 weeks after the procedure.



I have been conducting a 15-year research project that I intend to publish, on the incidence of complications when performing facelift surgery with and without simultaneous LSR. The combination is valuable as the facelift surgery serves to restore a youthful jawline and neck while laser skin resurfacing serves to rejuvenate the entire facial skin. A facelift, while addressing skin quantity, does nothing for skin quality. A facelift makes a tighter face but does little to address rhytids (other than stretching them) and has no effect on actinic damage. Facelift surgery has been performed for almost a century and laser skin resurfacing procedures have been performed for several decades. Both of these procedures remain mainstays of comprehensive facial rejuvenation around the world. Both of these procedures have also undergone numerous permutations to decrease recovery time, hence, short-scar facelifts and fractional lasers. Although conservative procedures have become popular, I feel they are a compromise in the final result.
Two big questions have faced cosmetic facial surgeons for the past several decades (and decades prior to that with chemical peels):
- 1.
Can traditional facelift and traditional CO 2 be performed simultaneously?
- 2.
Is the combination safe, in terms of flap viability and repeatable outcomes?
The scientific literature has numerous articles validating the safety of simultaneous facelift and laser but also has articles against the practice. A preliminary literature review showed 14 articles supporting simultaneous laser and facelift and three articles saying it is unsafe. Regardless of what the literature or surgeon experience shows, another question that exists is “Does the simultaneous use of laser and facelift breach the standard of care and is this practice defendable in a lawsuit if flap necrosis or other complications ensue?” This is something that is really at the heart of the issue. Having opined as a defense expert on several facelift/laser malpractice suits, I can attest that there was no shortage of surgeons willing to testify for the plaintiff that simultaneous laser and facelift have no business in the same operative report. This can present a complex legal subject of what is more valid: the standard of care or the evidence-based literature?
Some surgeons prefer separate operations, one for facelift and a later operation for laser (or vice versa). The biggest problem with this involves a duplication of surgery, anesthesia, finances, and most importantly, recovery. Aggressive CO 2 laser recovery rivals 2 weeks, which is a similar recovery for a comprehensive facelift. It is a hard enough challenge for patients to take 2 weeks off for a procedure, let alone twice this.
Another relative advantage of the combined treatment is the fact that facelift patients have decreased sensory sensation in the immediate postoperative period, so laser pain is diminished.
The advantages of combined procedures are obvious but a relative disadvantage is the addition of the demanding recovery of an aggressive ablative laser procedure. A facelift as a sole procedure is a relatively straightforward recovery. A facelift with other procedures such as browlift, blepharoplasty, and facial implants obviously increases recovery time. Adding a laser to all of this significantly intensifies the recovery and post-surgical care, and some patients simply cannot tolerate this.
Procedure
At the time of writing, I have performed over 1000 consecutive facelifts over the past 15 years. Of these, 29% of the patients also had simultaneous full coverage, ablative, high-energy, high-density laser resurfacing. This included over 35 admitted cigarette smokers. All facelifts were standard anterior and posterior approaches with platysmaplasty and SMASectomy. The average distance of circumferential dissection of the flaps was 7–8 cm from the external auditory canal. At the end of the case (the laser is always performed last), the demarcation of the undermined and non-undermined areas were marked and treated as previously described.
In all cases, the Lumenis Encore Ultrapulse laser was used in a fully ablative manner with a computer pattern generator set at 80 mJ (6 J/cm 2 ) with a density of 6, and 600 Hz. In most cases, the central oval of the face was treated with 2–3 passes of laser and the perioral region was treated with 3–5 passes at the same settings. The skin surfaces were NOT debrided between passes.
The lasered area is coated with Vaniply ointment (Pharmaceutical Specialties, Inc.; www.psico.com ) and no facelift dressing is placed . The discontinuance of traditional facelift dressings was a gradual choice. As 30% of my facelifts had simultaneous laser resurfacing, the traditional bulky full facelift dressing was irritating the lasered skin. I began using smaller and smaller dressings until it became apparent that there was no detriment in eliminating the dressing totally. This has not increased the hematoma rate or produced any negative healing or recovery problems. It has been a great deletion that is appreciated by the surgeon, staff, and most of all, by the patients.
Out of the total group of over 1000 facelift patients, nine of patients experienced preauricular flap breakdown (1%), defined as a preauricular necrosis >1 cm 2 . Six of the patients with flap breakdown did not undergo simultaneous laser resurfacing (0.7%), while three patients did (0.35%). This is not statistically significant and the preliminary results show the combination of laser and facelift to be safe in experienced hands.
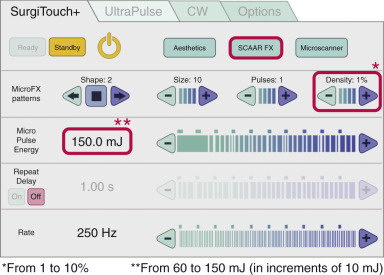
Ultra-Deep CO 2 Ablative Laser Treatment (SCAAR FX)
While most of the limelight in the laser research world had been directed in making lasers less invasive, ultra-deep laser treatment has also progressed. Lumenis has developed an ablative fractional laser platform called “SCAAR FX” (Synergistic Ablation and Coagulation for Advanced Resurfacing), which enables extremely deep treatment for hypertrophic and burn scars where conventional laser penetration is unable to penetrate ( Fig. 13.36 ). This technology not only penetrates up to 4 mm but it also produces significant coagulation ( Fig. 13.37 ). Some of the main problems with scars are aesthetic concerns, pain, and poor range of motion. The SCAAR FX treatment is being used to increase range of motion, improve pliability and texture, as well as to decrease pain and improve appearance. This is an exciting avenue of laser treatment and benefit.