Pistol grip deformity after slipped capital femoral epiphysis (SCFE) can cause anterior impingement leading to pain, cartilage and labral damage, and eventual osteoarthritis.1,2,8
 Realignment of the proximal femur, as well as restoration of the anterior head–neck offset, has been shown to improve hip clinical outcomes.7
Realignment of the proximal femur, as well as restoration of the anterior head–neck offset, has been shown to improve hip clinical outcomes.7
 This technique can be used to correct anterior impingement after an SCFE that has healed with residual posterior displacement.
This technique can be used to correct anterior impingement after an SCFE that has healed with residual posterior displacement.
 The first part of the procedure is a surgical hip dislocation approach with femoral head–neck osteoplasty.
The first part of the procedure is a surgical hip dislocation approach with femoral head–neck osteoplasty.
 If additional deformity correction is needed, the flexion intertrochanteric osteotomy is performed.
If additional deformity correction is needed, the flexion intertrochanteric osteotomy is performed.
PATHOGENESIS
 The true etiology of SCFE is unclear. However, because it occurs mainly in adolescent boys (80%), hormonal factors are thought to be involved.
The true etiology of SCFE is unclear. However, because it occurs mainly in adolescent boys (80%), hormonal factors are thought to be involved.
 Additionally, the orientation of the growth plate becomes more vertical in adolescents compared to the juvenile hip, leading to increased shear stress across the physis.
Additionally, the orientation of the growth plate becomes more vertical in adolescents compared to the juvenile hip, leading to increased shear stress across the physis.
 The transition from juvenile to adolescent is a period of rapid weight gain, leading to the stereotypical obese body habitus in the SCFE patient.
The transition from juvenile to adolescent is a period of rapid weight gain, leading to the stereotypical obese body habitus in the SCFE patient.
NATURAL HISTORY
 Undetected SCFEs can lead to hip arthrosis. Murray4 suggests that up to 40% of hips with degenerative arthritis have a “tilt deformity” or other deformities that may be due to an undetected subclinical SCFE or other developmental problems.
Undetected SCFEs can lead to hip arthrosis. Murray4 suggests that up to 40% of hips with degenerative arthritis have a “tilt deformity” or other deformities that may be due to an undetected subclinical SCFE or other developmental problems.
 A review by Aronson1 found that 15% to 20% of patients with SCFE had painful osteoarthritis by age 50 years. Additionally, 11% of patients with end-stage osteoarthritis had an SCFE.
A review by Aronson1 found that 15% to 20% of patients with SCFE had painful osteoarthritis by age 50 years. Additionally, 11% of patients with end-stage osteoarthritis had an SCFE.
PATIENT HISTORY AND PHYSICAL FINDINGS
 Patients will complain of insidious-onset groin or knee pain that may have previously been diagnosed as a sprain.
Patients will complain of insidious-onset groin or knee pain that may have previously been diagnosed as a sprain.
They may walk with a limp, but typically they walk with an externally rotated foot progression angle, which may indicate chronic SCFE or femoral retroversion.
Pain is elicited with hip flexion, adduction, and internal rotation stress (impingement test).
The physical examination should include flexion and internal rotation range-of-motion tests. Normal, physiologic hip flexion needed for activities of daily living is at least 90 degrees.
Patients with a chronic SCFE and anterior impingement will have less than 90 degrees of true hip flexion.
Patients with impingement secondary to SCFE will have less internal rotation in flexion than extension and may have a compensatory external rotation of the hip as it is flexed (obligate external rotation).
IMAGING AND OTHER DIAGNOSTIC STUDIES
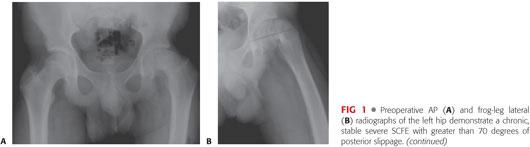
 Plain radiographs include an anteroposterior (AP) and frog-leg lateral views of the pelvis or the involved hip (FIG 1A,B).
Plain radiographs include an anteroposterior (AP) and frog-leg lateral views of the pelvis or the involved hip (FIG 1A,B).
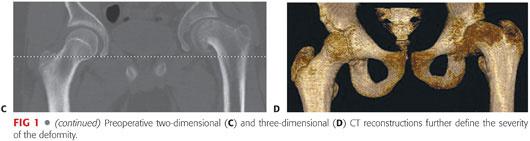
 Computed tomography (CT) scans with two- and three-dimensional reconstructions are helpful for preoperative planning (FIG 1C,D).
Computed tomography (CT) scans with two- and three-dimensional reconstructions are helpful for preoperative planning (FIG 1C,D).
DIFFERENTIAL DIAGNOSIS
 Femoral or acetabular retroversion
Femoral or acetabular retroversion
 Idiopathic femoroacetabular impingement
Idiopathic femoroacetabular impingement
NONOPERATIVE MANAGEMENT
 Nonoperative management includes cessation of aggravating activities and symptomatic treatment using nonsteroidal anti-inflammatories.
Nonoperative management includes cessation of aggravating activities and symptomatic treatment using nonsteroidal anti-inflammatories.
 Physical therapy to strengthen the hip musculature does not address the mechanical impingement associated with an SCFE.
Physical therapy to strengthen the hip musculature does not address the mechanical impingement associated with an SCFE.
 All SCFE should be stabilized surgically. Nonoperative management if for impingement symptoms.
All SCFE should be stabilized surgically. Nonoperative management if for impingement symptoms.
SURGICAL MANAGEMENT
 A chronic slip may be pinned in situ to prevent continued slippage. Remodeling of the SCFE deformity has been described in long-term follow-up studies.
A chronic slip may be pinned in situ to prevent continued slippage. Remodeling of the SCFE deformity has been described in long-term follow-up studies.
 Corrective osteotomies have been described through the femoral neck at the growth plate (cuneiform), at the base of the femoral neck, or intertrochantic or subtrochanteric.6
Corrective osteotomies have been described through the femoral neck at the growth plate (cuneiform), at the base of the femoral neck, or intertrochantic or subtrochanteric.6
Preoperative Planning
 The anterior head–shaft angle is measured on the AP pelvis radiograph on both the affected and normal sides. The difference is the amount of varus deformity on the slip side that can be addressed with a valgus-producing intertrochanteric osteotomy (FIG 2A).
The anterior head–shaft angle is measured on the AP pelvis radiograph on both the affected and normal sides. The difference is the amount of varus deformity on the slip side that can be addressed with a valgus-producing intertrochanteric osteotomy (FIG 2A).
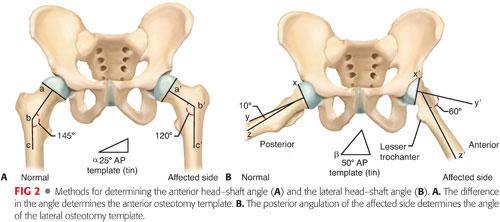
 The lateral head–shaft angle is measured on the frog-leg lateral view in a manner similar to that used on the AP view. The difference is the amount of posterior deformity present that is corrected with a flexion-producing intertrochanteric osteotomy (FIG 2B).
The lateral head–shaft angle is measured on the frog-leg lateral view in a manner similar to that used on the AP view. The difference is the amount of posterior deformity present that is corrected with a flexion-producing intertrochanteric osteotomy (FIG 2B).
Positioning
 Because the first part of the procedure is done through a surgical hip dislocation, the patient is placed in the full lateral position secured on a pegboard, as shown in Chapter 13, Figure 3. A flat-top cushion placed beneath the operative side is helpful to stabilize the leg during the approach.
Because the first part of the procedure is done through a surgical hip dislocation, the patient is placed in the full lateral position secured on a pegboard, as shown in Chapter 13, Figure 3. A flat-top cushion placed beneath the operative side is helpful to stabilize the leg during the approach.
A hip drape with a sterile side bag is used, which will capture the leg during the dislocation maneuver.
Approach
 The incision from the surgical hip dislocation is extended slightly distal, along the lateral aspect of the thigh, in line with the femoral shaft.
The incision from the surgical hip dislocation is extended slightly distal, along the lateral aspect of the thigh, in line with the femoral shaft.
 The lateral approach to the proximal third of the femur is required for the intertrochanteric osteotomy.
The lateral approach to the proximal third of the femur is required for the intertrochanteric osteotomy.
TECHNIQUES
 Approach to Proximal Femur
Approach to Proximal Femur
The longitudinal incision from the surgical hip dislocation can be extended distally, in line with the lateral shaft of the femur (TECH FIG 1A).
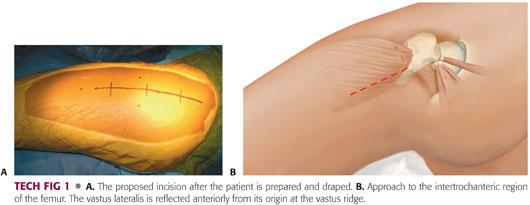
The vastus lateralis, supplied by the femoral nerve, is reflected anteriorly from the vastus ridge distally (TECH FIG 1B).
Several perforating vessels from the profunda femoris artery to the vastus lateralis should be identified and coagulated before they are avulsed by blunt dissection.
The anterolateral aspect of the femoral shaft is then exposed subperiosteally, and the lesser trochanter is identified.
 Planning the Osteotomy
Planning the Osteotomy
A 2-0 Kirschner wire is placed just above the level of the lesser trochanter, beginning in the lateral cortex of the proximal femur. This is placed parallel to the floor in the axial plane and perpendicular to the shaft of the femur in the coronal plane. This is the reference for the level of the osteotomy.
A second Kirschner wire is placed 3 cm proximal to the first. This is placed parallel to the first guidewire in the axial plane. In the coronal plane, the Kirschner wire is placed with an appropriate amount of valgus, determined from the anterior head–shaft angle difference on preoperative radiographs. In the Imhauser technique, addition of a valgus osteotomy is not necessary, hence, a pure flexion osteotomy is performed. This will act as the guidewire for the seating chisel for the blade plate.
 Creating the Slot for the Blade Plate
Creating the Slot for the Blade Plate
The seating chisel is directed parallel to the most proximal guide pin with the appropriate amount of flexion, as determined on the frog-leg lateral head–shaft angle difference.
A slot for the blade plate should now be made in the trochanteric fragment to allow for anatomic fixation of the trochanter after the osteotomy.
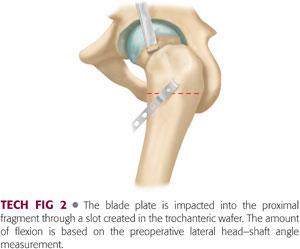
The blade plate chisel is placed into the proximal fragment after preparation of the trochanteric flip fragment and before cutting the intertrochanteric osteotomy (TECH FIG 2).
 Osteotomy
Osteotomy
Before osteotomy, a rotational reference mark is made at the level of the osteotomy on both the proximal and distal fragments.
Using an oscillating saw, the proximal femur is cut using the distal Kirschner wire as a guide. The cut should be made perpendicular to the shaft of the femur.
 Blade Plate Placement
Blade Plate Placement
The seating chisel is removed and the blade plate is impacted into the proximal fragment.
The osteotomy is provisionally reduced and held with a Verbrugge clamp.
Often, the distal fragment will need to be internally rotated to match the hip rotation of the normal side.
After confirming reduction using an image intensifier, the plate is fixed to the shaft of the femur in standard fashion (TECH FIG 3).

 Closure
Closure
The vastus lateralis fascia is closed with 2-0 absorbable running suture.
The iliotibial band is closed using a running no. 1 absorbable suture.
Skin is closed in routine fashion.
PEARLS AND PITFALLS | |
Indications |
|
| |
Osteotomy planning |
|
Seating chisel removal |
|
Reduction of osteotomy |
|
Nonunion |
|






POSTOPERATIVE CARE
 The hip is held flexed and in neutral rotation by placing two pillows under the leg and one under the greater trochanter.
The hip is held flexed and in neutral rotation by placing two pillows under the leg and one under the greater trochanter.
 The patient is placed in a continuous passive motion machine for 6 hours a day, set from 30 to 80 degrees of flexion.
The patient is placed in a continuous passive motion machine for 6 hours a day, set from 30 to 80 degrees of flexion.
 Prophylaxis for deep venous thrombosis is individualized; however, all patients should be started on mechanical compression devices immediately.
Prophylaxis for deep venous thrombosis is individualized; however, all patients should be started on mechanical compression devices immediately.
 After the epidural is removed, out-of-bed ambulation is permitted with one-sixth body weight partial weight bearing.
After the epidural is removed, out-of-bed ambulation is permitted with one-sixth body weight partial weight bearing.
 Range-of-motion exercises are started, but care is taken to protect the greater trochanter osteotomy by limiting adduction to midline and avoiding resisted abduction exercises for 6 weeks.
Range-of-motion exercises are started, but care is taken to protect the greater trochanter osteotomy by limiting adduction to midline and avoiding resisted abduction exercises for 6 weeks.
 AP and true lateral hip radiographs are obtained to evaluate healing of the osteotomy (FIG 3A,B).
AP and true lateral hip radiographs are obtained to evaluate healing of the osteotomy (FIG 3A,B).
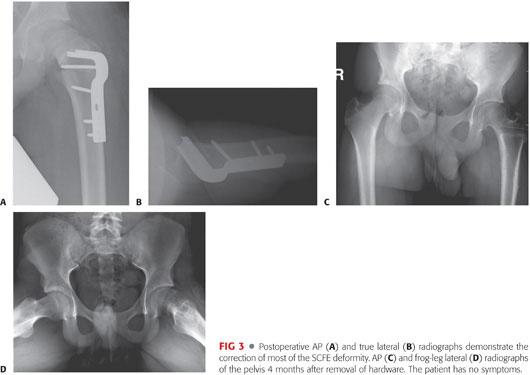
 Prominent hardware may be removed after 6 months if radiographic evidence of a healed osteotomy is seen (FIG 3C,D).
Prominent hardware may be removed after 6 months if radiographic evidence of a healed osteotomy is seen (FIG 3C,D).
OUTCOMES
 In Southwick’s original article,6 where he treated the deformity with a proximal femoral osteotomy without surgical hip dislocation, out of 28 hips (26 patients) with at least 5 years of follow-up, 21 were rated as excellent, 5 as good, and 2 as fair.
In Southwick’s original article,6 where he treated the deformity with a proximal femoral osteotomy without surgical hip dislocation, out of 28 hips (26 patients) with at least 5 years of follow-up, 21 were rated as excellent, 5 as good, and 2 as fair.
 In patients who had both osteoplasty and an intertrochanteric osteotomy, Western Ontario and McMaster Universities (WOMAC) pain and function scores improved in four of six patients.7
In patients who had both osteoplasty and an intertrochanteric osteotomy, Western Ontario and McMaster Universities (WOMAC) pain and function scores improved in four of six patients.7
 Internal rotation in flexion improved from −20 to +10 degrees.7
Internal rotation in flexion improved from −20 to +10 degrees.7
 Long-term results of flexion osteotomy for SCFE shows 55% to 77% good to excellent results at ~20 year follow-up.3,5
Long-term results of flexion osteotomy for SCFE shows 55% to 77% good to excellent results at ~20 year follow-up.3,5
COMPLICATIONS
 Avascular necrosis of the femoral head can occur if care is not taken to follow the technique and to preserve the retinacular vessels.
Avascular necrosis of the femoral head can occur if care is not taken to follow the technique and to preserve the retinacular vessels.
 Nonunion of the greater trochanteric osteotomy or the intertrochanteric osteotomy
Nonunion of the greater trochanteric osteotomy or the intertrochanteric osteotomy
 Sciatic or femoral nerve neurapraxia
Sciatic or femoral nerve neurapraxia
 Heterotopic ossification
Heterotopic ossification
REFERENCES
1. Aronson J. Osteoarthritis of the young adult hip: etiology and treatment. Instr Course Lect 1986;35:119–128.
2. Goodman DA, Feighan JE, Smith AD, et al. Subclinical slipped capital femoral epiphysis: relationship to arthrosis of the hip. J Bone Joint Surg Am 1997;79(10):1489–1497.
3. Kartenbender K, Cordier W, Katthagen BD. Long-term follow-up study after corrective Imhäuser osteotomy for severe slipped capital femoral epiphysis. J Pediatr Ortho 2000;20:749–756.
4. Murray RO. The aetiology of primary osteoarthrosis of the hip. Br J Radiol 1965;38:810–824.
5. Schai PA, Exner GU, Hänsch O. Prevention of secondary coxarthrosis in slipped capital femoral epiphysis: a long-term follow-up study after corrective intertrochanteric osteotomy. J Pediatr Orthop B 1996;5:135–143.
6. Southwick WO. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J Bone Joint Surg Am 1987;49(5):807–835.
7. Spencer S, Millis M, Kim Y. Early results of treatment for hip impingement syndrome in slipped capital femoral epiphysis and pistol grip deformity of the femoral head-neck junction using the surgical dislocation technique. J Pediatr Orthop 2006;26:281–285.
8. Wenger DR, Kishan S, Pring ME. Impingement and childhood hip disease. J Pediatr Orthop B 2006;15:233–243.
< div class='tao-gold-member'>



