Key points
- •
Intense pulsed light (IPL) is a non-laser light source that can be used for multiple applications.
- •
IPL treatments require knowledge of the absorption spectra of the targeted chromophores.
- •
IPL treatments can have treatment associated complications.
- •
IPL results can be optimized when combined with other non-invasive cosmetic treatments.
Introduction
Intense pulsed light (IPL), non-laser induced selective photothermolysis has become an accepted method of treating a wide gamut of vascular and pigmented lesions, photodamage, acne, as well as for the treatment of unwanted hair. These devices differ from true lasers in that they contain a powerful flashlamp instead of laser medium. This non-coherent, polychromatic light source can be ‘tuned’ to provide a variety of wavelengths, fluences and pulse durations. IPL technology delivers non-coherent light in the 420–1200 nm range. The light is delivered either as a single pulse or in divided synchronized millisecond pulses separated by short thermal relaxation intervals for protection of epidermal melanin. The light is focused by a reflector and transmitted through a set of filters that determine its spectral characteristics. With IPLs, a variety of parameters must be chosen. These include the spectrum of delivered wavelengths as determined by cutoff filters; number of delivered pulses; pulse duration in milliseconds; delay between pulses in milliseconds; and delivered fluence. The cutoff filters are utilized to tailor the spectrum of light to the skin type and absorbing substance (chromophore). The filter cuts off the emitted light, so that only wavelengths longer than the utilized filter value pass to the treated hair and skin. A 560 nm filter, allowing emitted wavelengths longer than 560 nm might be used to treat vascular lesions; a 615 nm filter, allowing wavelengths greater than 615 nm to be emitted might be used for some patients with unwanted hair. The light is usually applied to the skin through a rectangular light guide. Both cool gel and a variety of bracketed cooling devices have been utilized to cool the skin.
Newer systems are a significant improvement on earlier systems. Accurate calibration of the light source in current systems prevents changes of fluence with source degradation. Bulb life has been lengthened with some manufacturers offering unlimited pulses from their handpieces. Some manufacturers have different handpieces corresponding to different cutoff filters while others provided one handpiece with interchangeable filters. Variable spot sizes are often an option at this time. Degree by degree integrated cooling is also available allowing more flexibility and safety of treatments. Current systems are significantly faster than their predecessors making the systems more useful for large area hair removal.
IPL systems are similar to their laser cousins in that their use is also based on the principle of selective photothermolysis. IPLs feature large spot sizes that enable treatment of vascular abnormalities covering broad areas. Another potential advantage of IPL is the delivery of light energy over longer pulse durations, leading to more uniform heating and coagulation throughout the vessel in its entirety. A disadvantage to traditional IPL sources is the lack of selectivity. Consequently, complications may arise from epidermal melanin absorption within the emitted spectrum, particularly if effective epidermal cooling is not utilized. IPL sources have been described to be effective in the treatment of a variety of vascular conditions, including facial telangiectasia, poikiloderma of Civatte, superficial hemangiomas, and port wine stains (PWS).
We are often asked which laser or energy device should be bought first in clinical practice. An IPL device often makes the most sense for an initial purchase due to the wide variety of clinical conditions which may be treated with this device. There are a number of manufacturers that make excellent intense pulsed light devices. Newer and more technologically advanced devices have integral cooling large spot sizes, calibrated bulbs and fast recycling times.
Clinical studies
Intense pulsed light has also been used to treat PWS. The first report of thermocoagulation of PWS by polychromatic light was by Muhlbauer et al in 1976. In another study, a PDL-resistant PWS completely resolved after treatment with an IPL device while another study of 37 patients treated with IPL showed a clearance of pink and red PWS, and lightening in purple PWS. Direct comparison of an IPL with a PDL source in a study of 32 patients showed that overall, the response rate was better with the PDL (Strempel 1996). However, it was noteworthy that six of the 32 patients had a better response with the IPL. The potential role of IPL for treating PDL-resistant PWS is confirmed by a study showing responses in seven out of 15 patients previously resistant to PDL, with six patients showing between 75% and 100% improvement (Bjerring 2003).
Intense pulsed light source
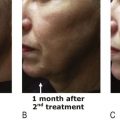
Several investigators have shown successful rejuvenation of photodamaged skin after IPL treatment. In general, shorter cut-off filters are used to treat both pigmented and vascular lesions. Bitter ( ) showed improvement in wrinkling, skin coarseness, irregular pigmentation, pore size, and telangiectasia in the majority of 49 patients treated with a series of IPL treatments. In a retrospective review of 80 patients with skin phototypes I-IV, Weiss and colleagues reported improvement on various signs of photoaging, including telangiectasias and mottled pigmentation of the face, neck, and chest, after a series of IPL treatments ( ). Not only is substantial clinical improvement of dyspigmentation and telangiectasia associated with cutaneous photodamage seen after IPL treatment, but neocollagenesis and dermal collagen remodeling can also be noted. Despite this, improvement in rhytides following IPL treatment has been more modest. The effect on dermal collagen is thought to be induced by heat diffusion from the vasculature with subsequent release of inflammatory mediators stimulated by vessel heating.
Gold published the first significant series of patients seeking hair removal with IPL ( ). He evaluated hair removal efficacy in 31 subjects (three men, 27 women, one transsexual). Patients ranged in age from 14–74 years. The majority of treated individuals were between 30 and 50 years of age. A total of 37 treated sites were evaluated. All sites were treated one time and evaluated 2, 4, 8 and 12 weeks after treatment. Although a variety of anatomic sites were treated, the most common areas were the neck (27%), lip (22%) and chin (19%).
Hair clearance was analyzed by placing responses into four quadrants: 0–25% clearance; 25–50% clearance; 50–75% clearance; and 75–100% clearance. Approximately one-third of the treated patients showed no clearance immediately after treatment. The remaining individuals were divided into the other three groups. Approximately one-fifth of the group was in the top two quadrants. At 12 weeks, the top two quadrants included 70% of the population. Since the authors only followed patients for 12 weeks, there could be no claim of long-term hair removal. In addition, patients were treated only once. It would be expected that the results would be improved after multiple treatments. Weiss et al expanded the aforementioned evaluation of the IPL’s hair removal efficacy. The authors looked at not only the 3 month results after one treatment, but also hair removal efficacy 6 months after two treatments ( ).
Twenty-eight sites on 23 subjects, with Fitzpatrick skin types I–III, were enrolled in a study using a single IPL treatment. They were followed for 3 months. Another 56 sites on 48 subjects, with Fitzpatrick skin types I–V, were treated twice, with 1-month intervals between the two treatments. These individuals were followed for 6 months. Anatomic sites included in the double treatment protocol were facial regions (chin, submental, neck, lip, ear, cheek and preauricular locations) and non-facial regions (back, bikini, thigh, shoulder, abdomen, and forearm).
At the first visit, immediate post-treatment mean hair clearance of 16% was recorded. This improved to 56% at weeks 2 and 4, 54% at week 8, with a final 63% reduction at 12 weeks. These findings, suggestive of effective temporary hair removal, were consistent with those seen by Gold. Of greater significance were the findings in the second study. In the double treatment protocol, immediate post-treatment clearance of 64% was achieved. At week 8, a 42% hair reduction was noted. At 6 months, hair reduction was found to be 33%. In addition, many residual hairs were reduced in diameter. It is observations such as these that emphasize the importance in looking beyond simple hair counts in determining hair removal efficacy.
Finally, in our own center, a study was recently conducted to compare the efficacy of two laser and two IPL systems for hair removal: 755 nm alexandrite, intense pulsed light with a red filter, intense pulsed with a yellow filter and an 810 nm diode laser were all evaluated. A significant decrease in hair counts (∼50%) and hair coverage (∼55%) did not statistically differ between the four modalities, with a follow-up period of up to 6 months.
Patient selection
Patient selection for intense pulsed light treatments is as important as the device and settings utilized. For instance, treating a type 3 patient who has received recent sun exposure is likely to show a high degree of post treatment hyperpigmentation as well as patient dissatisfaction. Treating a patient who has rhytids (which ideally require dermal fillers or toxins) with the goal of correcting these issues with an IPL is also destined to fail. Thus, the primary qualification for good outcomes is reasonable patient selection. Among the variables to consider are: patient skin type, ability to comply with treatment regimen, realistic expectations, and ability to pay for the amount of treatments needed to obtain a benefit.
The universal standard for patient skin typing is the Fitzpatrick skin type scale. ( Tables 5.1–5.3 , Box 5.1 ) This scale provides an accurate initial assessment of skin type based upon genetic disposition, sun exposure, and tanning habits. This scale should be considered as a tool and not the answer to safe IPL treatments. In addition to the Fitzpatrick scale, the clinician should also perform a visual assessment of the patient’s actual skin color in the treatment area in comparison to less sun exposed areas. Patients are often negligent in admitting their activities, therefore, it is of the utmost importance to include questions about spray tan, tanning beds, tanning creams, photo-sensitizing medications and outdoor activities prior to treatment. Educating the patient about the benefits and risks of skin color in relation to the procedure and outcome leads to an improved client/clinician relationship.
| GENETIC DISPOSITION | |||||
|---|---|---|---|---|---|
| Score | 0 | 1 | 2 | 3 | 4 |
| What are the color of your eyes? | Light blue, gray, green | Blue, gray or green | Blue | Dark brown | Brownish black |
| What is the natural color of your hair? | Sandy red | Blond | Chestnut/Dark Blond | Dark Brown | Black |
| What is the color of your skin (non exposed areas)? | Reddish | Very pale | Pale with beige tint | Light brown | Dark brown |
| Do you have freckles on unexposed areas? | Many | Several | Few | Incidental | None |
| Total score for genetic disposition: _____ | |||||
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


