Key points
- •
Low level laser therapy (LLLT) has been used for more than 40 years.
- •
LLLT appears to promote hair regrowth in males and females with androgenic alopecia.
- •
LLLT has been used with success for accelerating the wound healing process, pain management, and inflammation.
- •
Case studies indicate that LLLT promotes hair growth in patients with alopecia areata.
- •
LLLT is safe for use in patients.
Introduction
Laser technology ranks as one of the most significant scientific discoveries of our time. Lasers have also captured the public imagination in a way that correlates the use of a laser as high-tech and an advanced solution. It is only natural that this technology, in the form of low level laser therapy (LLLT), should be applied to hair loss therapies. This chapter will review the history of LLLT, relevant data and studies, a comparison of existing devices, indications and uses, proposed mechanism of action, and where studies need to be performed.
History of lasers
In 1916, Albert Einstein laid the foundation for the invention of the laser and its predecessor, the maser, in a ground breaking rederivation of Max Plank’s Law of radiation based on the concepts of spontaneous and induced emission. The laser was proposed in the late 1950s and the first laser was demonstrated in 1960. Since that time laser research has produced a variety of improved and specialized laser types and has found applications in the field including science, industry, medicine and consumer electronics.
During the last 10–15 years the use of lasers in medicine has grown rapidly and found applications such as tattoo removal, treatment of vascular and pigmented lesions, scars, skin rejuvenation and hair removal. These lasers are also called hard or surgical lasers (deliver heat and energy) and their power is measured in watts (W). Cold or soft laser therapy is athermic or non-heat-producing and delivers just energy. It is also known as low level laser therapy (LLLT) and delivers its power in the range of milliwatts (mW = a thousandth of a watt). The first reports on the biological effects of the low level laser therapy appeared more than 40 years ago. Since then, many reports have been made.
The term ‘soft laser’ was originally used to differentiate therapeutic lasers from ‘hard lasers’. Different names then emerged, such as: biostimulating laser, low reactive-level laser, low intensity-level laser, photobiostimulation laser and photobiomodulation laser. The history of LLLT started in 1965 when American physicians used high power densities with low level laser therapy to destroy cancer cells. Later on, Mester’s group at the Semmelweiss hospital in Budapest published in Orvosi Heitlap 1966, the first scientific report of the stimulatory effects of non-thermal ruby laser light (694 nm) on the skin of rats. In the following years, articles were published on the effects of laser on wound healing, pain management, skin blood flow, bone regeneration, hair growth, liposuction and wound healing after hair restoration surgery, etc.
LLLT has monochromatic and coherent (synchronicity) light sources, it does not raise the body temperature above 36°C and its range is 500–1100 nm (visible to near infrared region of the spectrum). LED (light emitting diode) is not a true laser and should not be confused with laser. The first commercial therapeutic LLLT lasers appeared in the late 1970s. They featured a HeNe (helium neon) laser with fiber-optic cable. Output power ranged from 0.5–2 mW. GaAs (gallium arsenide) lasers (1–4 mW) were developed in the early 1980s. InGaA1P were developed as tools for laser therapy in mid 1990s ( Box 13.1 ).
| 1916 | Einstein’s theories on spontaneous and induced emissions. |
| 1950s | Lasers first proposed. |
| 1960 | First laser demonstration. |
| 1968 | First impact on hair growth noted. |
| 1970s | First therapeutic lasers introduced HeNe. |
| 1984 | First impact on hair growth in alopecia areata noted. |
| 1987 | First impact on hair regrowth in androgenetic alopecia and alopecia areta noted with HeNe laser. |
| 2003 | Initial studies on LLLT lasers and hair loss. |
| 2007 | FDA clearance on first LLLT laser for hair loss. |
It is important to mention that too low a dose of LLLT has no or an insufficient effect. Too high a dose is also less effective, or has no effect at all. It is critical to find the best settings for each device to obtain the best results. In the following sections you will find information about LLLT’s effect on hair growth including the proposed mechanisms of action, wave lengths, dose and different devices (hand held and hood), etc.
Mechanism of action
As previously reported, LLLT has been in existence for approximately forty years. Current uses for LLLT therapy center around three main areas of medicine: 1) wound healing (tissue repair, prevention of tissue death); 2) relief of inflammation in chronic disease and injuries); 3) relief of neurogenic pain and some neurological problems. Recent findings and published studies show LLLT effective in musculoskeletal and joint pain, neurologic damage and hair growth. The proposed pathways to explain the mechanisms of LLLT should ideally be applicable to all these conditions. However, there are no defined, absolute mechanisms of action that are available. There are many generally-accepted, detailed and comprehensive theories that seem to provide answers. We will present the more widely accepted theories and hypotheses regarding the action spectra, with emphasis on hair growth lasers.
General mechanism of action
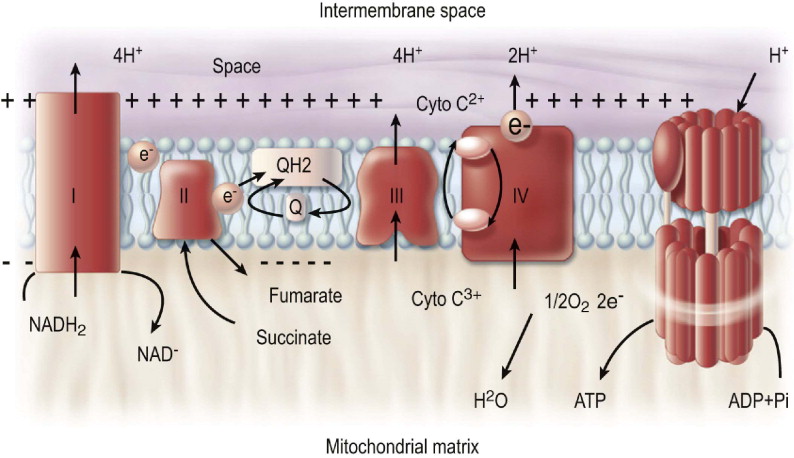
There are numerous theories and hypotheses on the mechanisms of action for LLLT. The general action spectra of LLLT was first theorized in 1989. M. Hamblin and T. Demidova indicate ‘The basic principle of this accepted theory states that the mechanism of action is based on the absorption of monochromatic visible and NIR (near infra-red) radiation by components of the cellular respiratory chain’ and the mitochondria plays a key role in this aspect. The inner mitochondrial membrane contains five complexes and the interaction between these components ends with the formation of the ATP synthase complex (carrier of cellular energy) ( Figure 13.1 ).
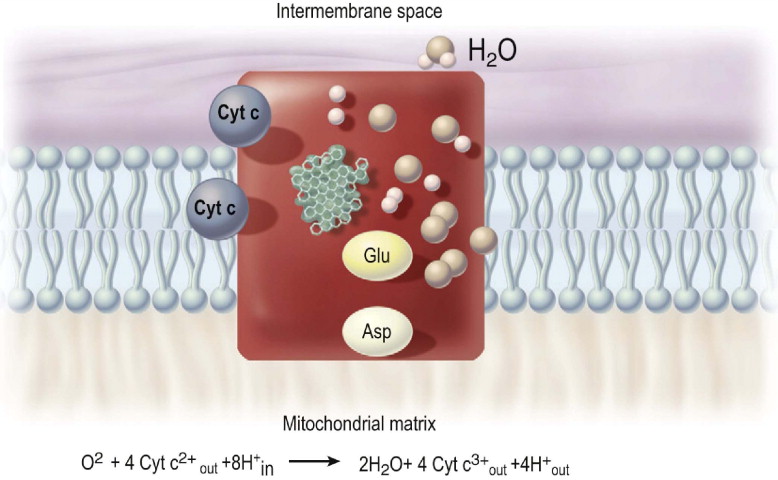
Absorption data recorded for cytochrome c oxidase in various states were shown to resemble the action spectra for biological responses to light. This led to the theory that cytochrome c oxidase is the primary photoacceptor for the red–NIR range in mammalian cells ( Figure 13.2 ). T. Karu’s group mentioned the generalized action spectrum for LLLT effects in cells, animals and patients. They gave the wavelengths ranges for four peaks in the LLLT spectrum: 1) 613.5–623.5 nm; 2) 667.5–683.7 nm; 3) 750.7–772.3 nm and 4) 812.5–846 nm.
Other theories on mechanism of action
There are other generalized theories regarding the mechanism that include the following actions:
Bioluminescence theory: DNA replication emits light at 630 nm (He–Ne). Photic stimulation may accelerate DNA replication.
Cellular oscillation theory: laser beam carries electromagnetic oscillations of definite frequency. When reaching tissue, these ‘swing and excite’ single cells, intensifying biochemical processes. Eventually the cell resonates and begins to emit light similar to the laser.
Biological field theory: connections between organs/tissues are not limited to humoral and nervous control alone. The resonance effect of LLLT restores normal energetic status of the organism.
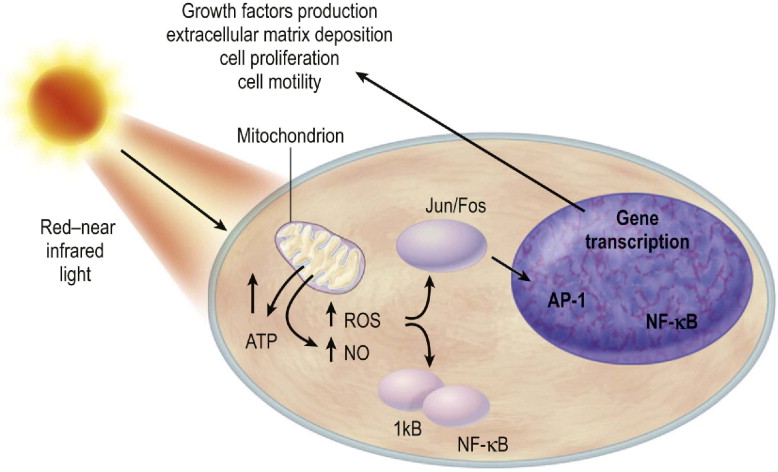
Cell signaling theory: M. Hamblin and T. Demidova suggested that LLLT produces a shift in overall cell redox potential in the direction of greater oxidation. Different cells at a range of growth conditions have distinct redox states causing the results of LLLT to vary. Cells being initially at a more reduced state have high potential to respond to LLLT, while cells at the optimal redox state respond weakly ( Figure 13.3 ).
Other possible theories regarding the mechanism of action include:
Adenosine diphosphate (ADP) absorbs the laser energy and is converted to adenosine triphosphate (ATP). ATP is the carrier of cellular energy. Increased levels of ATP provide the necessary cellular energy for the hair follicle to produce a healthier hair and potentially overcome the negative effects of DHT.
Vascularization: LLLT increases blood flow and circulation in the scalp. An increase in blood may deliver the essential nutrients to the hair follicle.
LLLT and hair growth
When laser therapy became more widespread for medical conditions ranging from wound healing, reduction of inflammation and pain alleviation, there were reports that these therapies also produced hair growth. While LLLT (in various forms) has been available for hair growth for approximately 20 years, no studies were available until recently to prove safety and efficacy. The only FDA-cleared (1/07) LLLT device for hair growth is the Hairmax LaserComb.
Uses of low level laser therapy
LLLT has been used for the treatment of many medical and rehabilitative conditions. Unlike hard lasers that are used to ablate, cauterize, coagulate, or remove tissue, soft lasers work with cellular and tissue effects to reduce inflammation, pain and increase blood flow. For years, LLLT has been used in Canada, Europe, and Asia and recently in the USA for the treatment of various neurological, chiropractic, dental and dermatologic disorders. In 2002, the FDA issued the first 510K for soft or cold devices in the primary treatment of carpal tunnel syndrome. Most recently, in 2007, the FDA also cleared the first device for hair growth.
LLLT has been used in different medical and dental indications: from a (asthma) to Z (herpes zoster). In this section, we only will talk primarily about the most frequent uses: wound healing, pain management and reduction of inflammation and the limited data on LLLT in hair loss.
Wound healing
LLLT may produce some important effects in the wound healing process:
- •
Enhance leukocyte infiltration.
- •
Increase macrophage activity.
- •
Increase neovascularization.
- •
Increase fibroblast and keratinocyte proliferation.
- •
Early epithelization.
- •
Increment of the growth factors.
- •
Enhanced cell proliferation and differentiation.
- •
Greater healed wound tensile strength.
- •
Stimulate vascular endothelial growth factor (VEGF).
In some studies the laser also showed bone repair including trabecular bone growth along with collagen matrix organization. NASA also has done some projects in wound healing and laser. They demonstrated that wavelengths between 670 and 880 nm at total energy levels of 4–8 J/cm 2 applied at power densities of 50 mW/cm 2 are optimal parameters. Mester and colleagues pioneered human studies of LLLT. In 1975, they reported that irradiation with a ruby laser resulted in healing of chronic soft tissue ulcers; the author examined more than 1000 cases.
In 1991, Lundeburg and colleagues compared the HeNe laser vs placebo in the treatment of 46 venous leg ulcers and found no statistically significant difference. In 2000, Simunovic and colleagues assessed the efficacy of LLLT on wound healing in 74 patients following different type of injuries who had surgical procedures prior to LLLT. The investigators concluded that LLLT accelerated wound healing and functional recovery which led to early return to work, training and sports competition compared to the control group of patients, and therefore a subsequent cost benefit. In 2002, Schindl et al used the HeNe (632.8 nm) laser or sham for improvement in skin microcirculation in patients with diabetic microangiopathy. The results showed a significant increase in skin circulation due to athermic laser irradiation in patients with diabetic microangiopathy.
In 2007, Perez-Meza and colleagues evaluated the use of LLLT in the recipient area following hair transplant surgery. They compared the laser hood 670 nm (InGaAl) vs LED; 16 patients were included and four laser sessions were given. They concluded that the LLLT accelerates the wound healing process after hair transplant surgery reducing the redness, edema and crust formation in the recipient area vs LED. Further multi-center studies with more patients are needed to reproduce this conclusion. In 2007, Andrews and colleagues included ten patients in their study and demonstrated positive effects of the hand held laser (MicroLight ML830®) vs placebo for reducing pain, discomfort and tightness of the donor area following hair transplant surgery. Again, additional multi-center studies are needed to see if these results are reproducible.
Pain management
The application of soft or cold laser to myofascial syndromes is very common and wide spread. Jan Tuner and Lars Hode concluded that laser therapy on chronic pain conditions can increase pain level initially; however, this reaction is absent when treating acute injuries – acute injuries can actually receive higher doses than chronic cases without side effects. The LLLT may produce pain reduction with the combination of the following biologic events:
- •
Increase in β-endorphins.
- •
Blocked depolarization of C-fiber afferent nerves.
- •
Increased nitric oxide production.
- •
Increase nerve cell action potential.
- •
Axonal sprouting.
In 2000, Simunovic confirmed the positive effect of laser therapy in sports injuries in a double-blind multicenter study using a combination of GaAlAs and HeNe laser. Danish studies by Axelsen in 1993 found no effect on ankle sprain, Achilles tendinitis, or medial tibial stress syndrome. In 2000, Oshiro selected six Japanese sumo wrestlers and treated their symptoms. Laser therapy resulted in alleviation of their symptoms and an increase in their performance and win–lose record. Simunovic made a comparison between LLLT, transcutaneous electro-neural stimulation, visible incoherent polarized (VIP) light and placebo in the treatment of lateral epicondylitis on 120 patients. The results showed that the highest percentage of pain relief was achieved in patients treated with LLLT. LLLT also has demonstrated positive effects for the treatment of fibromyalgias, osteoarthritis, tendinopathies, temporomandibular disorders, tennis and golfer’s elbow.
A study was done in Michigan, USA in the GM plant where Anderson et al evaluated the effects of LLLT on carpal tunnel syndrome (CTS). The study included 119 patients; half received sham laser and half laser therapy; both groups received physical therapy. The results showed a statistically significant treatment effect in the laser group vs the placebo group. Dentists and oral surgeons have applied laser irradiation with success to painful and superficial conditions ranging from gingivitis and aphthous ulcers to temporomandibular pain and superficial wounds.
Inflammation
Injured cells and tissues have greater affinity for LLLT after injury. In 2008, Aimbire et al studied the effect of 660 nm laser on mRNA levels of neutrophils as anti-apoptotic factors in induced lung inflammation. They concluded that LLLT reduced the levels of anti-apoptoses in inflamed mice lung neutrophils. Albertini and colleagues concluded that both 660 and 684 nm red wavelengths of LLLT are effective in reducing edema formation and inflammatory cell migration. In summary, LLLT has no serious side-effects. It is easy to use, safe and has worked well in some areas where traditional therapies have had little or no effect. The use of low level laser devices requires education on the diversity of wavelengths, powers, dosages, treatment techniques, etc. Many times negative results are related to inadequate settings and improper use of the laser devices. These aspects must be further evaluated in future research studies.
Hair loss scientific studies
The level of interest in the use of LLLT in hair loss has grown substantially since 2003. This interest has generated a few new studies designed to examine the mechanisms of action, achievable results, optimal treatment approach, etc. However, currently there is little information about the use of LLLT for hair regrowth in androgenetic alopecia in men and women. Some of the available studies will be summarized.
In 1968, E. Mester reported hair growth secondary to the stimulatory effects of non-thermal ruby laser light (694 nm) vs the control group in the skin of mice. In 1984, Mario Trelles found hair regrowth in patients with alopecia areata following the use of LLLT; he used the HeNe laser. In 1987, Cisneros & Marti reported hair regrowth of patients with androgenetic alopecia and alopecia areata with the use of HeNe laser. In 2005, Roy Geronimus et al published an in vitro study: LED photomodulation induced hair growth stimulation. They concluded that photomodulation using visible light can alter the expression of genes associated with stimulation of hair growth and that the effect is dependent upon treatment parameters. Waiz et al in 2006 noted hair regrowth with the use of pulsed infrared diode laser (904 nm) for the therapy of resistant patches of alopecia areata. They found 94% success vs 6% with no response.
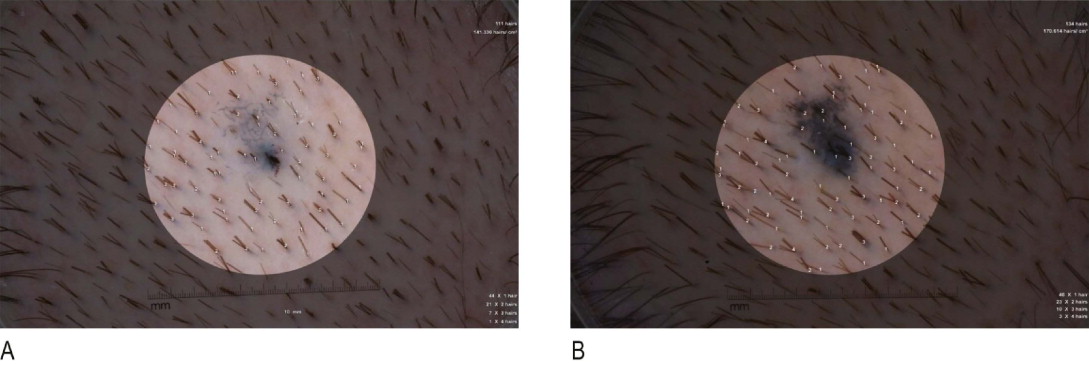
There are three recent studies about hair loss and LLLT. The first study from 2004–2005 was a 26 week, double blind, multicenter, randomized and placebo control study of 123 patients, 30–60 years old. In this study, I. Cantor and colleagues studied the effects of the HairMax LaserComb® on hair growth in males. Norwood class 2A–5 were included. HairMax Lasercomb® (3 times per week on non-consecutive days for 26 weeks) vs placebo (same period of time) was used for the study. The device was used 10–15 min each time. Global and macrophotography pictures were taken at baseline, 8, 16 and 26 weeks. The results showed that the laser group patients had a mean increase of 18.8 hairs/cm 2 vs a mean decrease of 10.6 hairs/cm 2 in patients using the placebo device. 93.9% of patients using the laser device experienced some increase in hair density. 11% of the patients of the laser group had minor adverse effects (tingling sensation in the scalp, pruritus of the scalp) vs 7.3% of the placebo group. The authors concluded that the HairMax LaserComb® was effective in the promotion of hair growth in males with androgenetic alopecia. The results also demonstrated that the LaserComb® is safe in these subjects ( Figure 13.4 ).
Related posts:
 CO 2laser applications: new fractional and traditional CO 2laser resurfacing and CO 2laser blepharoplasty
CO 2laser applications: new fractional and traditional CO 2laser resurfacing and CO 2laser blepharoplasty
 Aging skin: intrinsic aging and chronic photoaging
Aging skin: intrinsic aging and chronic photoaging
 Laser hair removal
Laser hair removal
 Advances in light-emitting diodes (LED) technology and therapy
Advances in light-emitting diodes (LED) technology and therapy
 Clinical photography for laser and light-based therapies
Clinical photography for laser and light-based therapies
 Non-invasive body contouring
Non-invasive body contouring
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


