Key points
- •
Science of energy induced skin tightening.
- •
Description of radiofrequency effects.
- •
Description of light devices used.
- •
How to manage outcomes and expectations.
- •
Future technology.
Introduction
The skin, like all organs, undergoes a natural, chronological aging process. The process of premature and pathologic aging is commonly known as photoaging or dermatoheliosis. This is mainly caused by exposure to ultraviolet radiation but depends on other factors such as skin quality, cumulative exposure to the sun, and the additive result of other environmental factors, such as tobacco smoke. As we age, the skin becomes thinner with a decrease in subcutaneous fat as well as a reduction in the size and metabolic rate of fibroblasts. Along with this decrease in the rate of collagen synthesis, the amount of elastin in the skin decreases. This results in production of disorganized and defective collagen.
The effects of dermal heating are well recognized to include modification of collagen structure and stimulation of neocollagenesis. These changes can help improve the appearance of fine rhytids and skin that has begun to lose its elasticity. Dermal heating may be achieved directly via ablative laser skin resurfacing or indirectly through an intact epidermis via a process variably referred to as ‘non-ablative skin resurfacing’, ‘subsurface resurfacing’, and others.
While surgical interventions produce the most dramatic results, many patients are reluctant to invest the time and financial commitment in addition to accepting the perioperative risks of such procedures. This has sparked a trend in non-surgical facial rejuvenation. Laser ablative skin resurfacing was the first modality to gain widespread acceptance, delivering reproducible and consistent results for facial rhytids and photoaging. This continues to be the gold standard to which new non-ablative interventions are compared. However, ablative resurfacing techniques require significant patient downtime and prolonged post-operative care. This eventually led to the next generation of minimally invasive facial rejuvenating procedures including non-ablative lasers, light sources such as 1320 nm Nd:YAG and 1450 nm diode, and intense pulse light.
Although these therapies satisfy the desire for less recovery time and potentially fewer risks, they require multiple treatments and therefore longer time to achieve the desired results. This resulted in a drive to develop a new market for non-invasive skin rejuvenation that achieves dermal tightening with no epidermal destruction. Currently, available devices that heat the deeper dermis utilize radiofrequency energy alone, radiofrequency energy plus infrared laser energy, near- and mid-infrared pulsed light devices, and intense ultrasound energy.
In contrast to light energy, which generates heat in targeted chromophores, electrical energy produces an electric current that generates heat through the resistance in the dermis and subcutaneous tissues. This can be advantageous for selective deep dermal heating, as surface tissue proteins do not impede the movement of electrons. Radiofrequency (RF) energy heats tissue by creating electric fields between two electrodes thus causing molecules to rotate or move. In the case of a monopolar electrode the charge changes rapidly (as much as 6 million times per sec) from positive to negative, alternately attracting and repelling electrons and charged ions. This induces rotation of the polarized molecules and the resistance to this movement creates heat. Bipolar electrodes function by passing current between two electrodes positioned relatively near one another. In passing between the electrodes the electrical energy flows through the skin, thus heating it as described above.
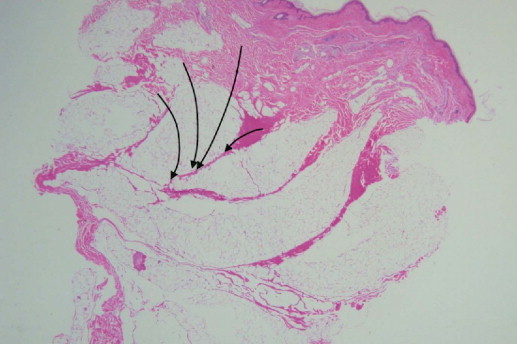
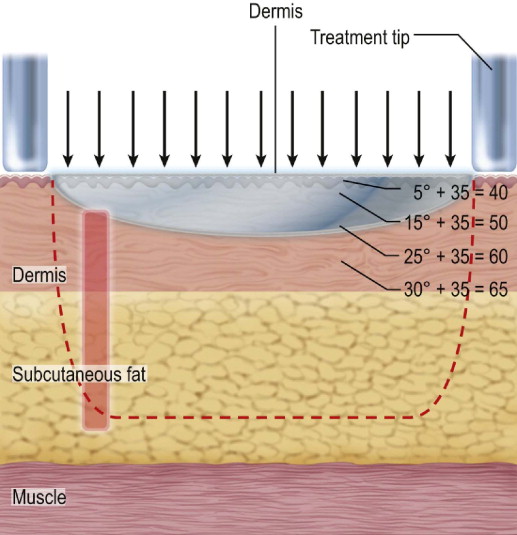
This thermal effect is based on the formula: Energy ( J ) = I 2 × R × T ( I = current, R = impedance of tissue, and T = time of application). Thus, the size of the treatment tip and the conductive properties of the tissues being treated determine the depth and degree of thermal injury. Resistance varies with the nature of the tissue (e.g., skin vs fat), temperature, and water content (e.g., infiltration with tumescent solution). This thermal energy causes partial collagen denaturation at the level of the deep dermis, leaving the epidermal layer without significant injury. In addition, it has been shown that the fibrous septae deep to the dermis in the subcutaneous fat demonstrate conductive properties similar to that of the dermis, resulting in selective heating and denaturation at this deeper level as well ( Figure 6.1 ). Together, these effects are responsible for the overall contour changes observed with this treatment modality.
The results of thermal modification of the dermal collagen and shortening of the fibrous septae extending from the dermis into the subcutaneous tissues are demonstrated in both immediate and long-term effects on the collagen framework. Initially, the denaturation of the collagen fibril occurs, and this is thought to be responsible for immediate collagen contraction. The subsequent healing response in the dermis leads to neocollagenesis with an increase in the amount of both the elastin and collagen fibers in these deep tissues over the months to follow. This replaces the collagen previously lost as a result of environmental exposures and the aging process.
In addition, the use of RF technology has recently been combined with various other treatment modalities, and newer nonablative treatment technologies are currently being tested. For instance, bipolar RF energy has been coupled with light energy in a technique referred to as ELOS, an acronym for el ectro- o ptical s ynergy. According to this theory, by combining light and RF, lower energies of each would be required than if either modality were used alone. RF has also been coupled with vacuum suction to induce a conformational change in dermal collagen with subsequent skin tightening. Infrared light energy and the use of intense ultrasound have also been used to produce dermal heating. Studies with this these various techniques have demonstrated clinically comparable results to RF therapy and will also be mentioned in this chapter.
Patient selection / indications
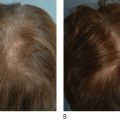
As for any cosmetic procedure, appropriate patient selection is critical to achieving successful end results. Unlike other treatment modalities, radiofrequency energy can be used in all Fitzpatrick sun-reactive skin types. The ideal patient for dermal heating therapy is one with early signs of aging, with no significant rhytids or structural ptosis. Best outcomes are likely to be achieved in patients in their third through fifth decades with early signs of skin laxity. This technology has also shown promise in patients with moderate to severe acne vulgaris using the same techniques employed for use in facial rhytids. It is also important to note that RF therapy does not adversely affect hair growth. Further indications for therapy are being tested throughout the entire body including the trunk and extremities.
There are a minimal number of absolute and relative contraindications the practitioner should keep in mind when evaluating a patient for non-ablative skin rejuvenation. Absolute contraindications include patients with active dermatological, collagen–vascular, or autoimmune disorders. Patients within 6 months of treatment with isotretinoin and immunosuppressed patients should also be excluded. Final absolute contraindications include treatment in areas of prior radiation therapy or overlying metal implants, braces, or hardware. In addition, there are a number of relative contraindications to consider. RF should not be used, or used only after medical clearance, in patients with pacemakers or defibrillators, as they must be deactivated during treatment sessions. Patients with extreme skin redundancy and obese patients are not likely to have dramatic results. The use of RF in pregnancy has not been studied in the literature, however, we feel this practice is best avoided.
Current available devices
Monopolar RF (Thermage ® , ThermaCool ™ )
Thermage, Inc. (Hayward, CA) developed a monopolar RF delivery system that included a unique capacitive coupling device that permitted uniform energy distribution across the entire electrode surface with subsequent volumetric tissue heating. The ThermaCool™ device delivers RF energy with a maximum fluence of 225 J/cm 2 , though the upper limit for facial skin without coagulation or burning at the electrode–skin interface is 140 J. The tissue is heated in a uniform fashion with peak temperatures centered approximately 2–3 mm beneath the surface. Tissues are heated to 55–75°C which is the critical temperature for collagen denaturation ( Figure 6.2 ).
A feature unique to the Thermage® device is the cooling system integrated into the handpiece. Upon activation of the device, cryogen spray is used to internally cool the electrode prior to use (precooling). The cryogen continues to be delivered throughout (parallel cooling) and after (post cooling) the energy delivery. After the tip comes into contact with the skin, coolant is sprayed on the back surface of the electrode, drawing heat out of the surface of the skin and generating a thermal gradient. The simultaneous delivery of cryogen within the treatment tip allows the device to provide deep volumetric heating of tissue without damaging the epidermis.
The depth of penetration of the RF field as well as time to achieve this is determined by the design of the treatment tip. The first tip released with this system took a total of 6 s for a complete cycle but a recently released model completes the cycle in only 1.9 s, making it possible to treat large areas more effectively. Also, in order to produce favorable clinical changes in most anatomic regions, the central zone of the thermal gradient needs to be established approximately 2.5 mm below the skin’s surface. However, studies using RF therapy in the areas of thin skin, such as the eyelids, have shown delivery of heat to this depth to be potentially dangerous. A ‘shallow’ treatment tip, delivering maximal heating to approximately 1.2 mm below the skin’s surface was designed. There are now treatment tips of various sizes, ranging from 0.25 cm 2 to 3 cm 2 , as well as various depths of thermal gradients.
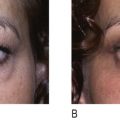
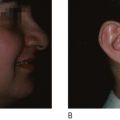
Non-ablative RF treatment was approved for periorbital skin rejuvenation by the United States Food and Drug Administration (USFDA) in November 2002. The first US study performed with Thermage® was a multicenter study in which patients underwent treatment of the periorbital region. Fitzpatrick wrinkle score was improved by at least one point in 83% of treated areas. Eyebrow elevation was also observed in early trials with RF therapy, ranging from 0.5–4.3 mm of elevation at the midpupillary line ( Figure 6.3 ). However, overall patient satisfaction was low due to the use of treatment algorithms using high energy levels and relatively few treatment spots which was poorly tolerated by the patient. Complications such as pain and subcutaneous fat atrophy, for which severe cases required fat grafting, were not uncommon. Patient dissatisfaction ultimately led to the development of larger, faster, more shallow treatment tips. The contemporary algorithm for treatment with RF energy employs these larger device tips with more passes at lower energy levels. These changes have demonstrated conformational changes in a greater percentage of dermal collagen fibrils with fewer complications and improved patient tolerance. Results have been shown to occur gradually with progressive improvement taking up to 12 weeks to fully manifest.