Abstract
The common diseases discussed in this chapter are characterized by discrete, small, erythematous papules that do not become confluent. Most of these disorders are pruritic, some markedly so. As a result, the papules are often crusted secondary to excoriation. Papules are common primary lesions found in numerous skin diseases, including acne, eczematous diseases (e.g., atopic dermatitis), and the scaling disorders (e.g., psoriasis). However, in these diseases, other features are present that allow for their characterization. For example, comedones and pustules accompany papules in acne, eczematous papules coalesce into plaques in atopic dermatitis, and plaques as well as papules located on extensor surfaces are present in psoriasis. The diseases in this chapter feature individual papules as the predominant finding or primary lesion ( Table 11.1 ). History and physical examination often establish the diagnosis but a biopsy, when needed, confirms the clinical suspicion.
Insect Bite Reactions
- 1.
Immediate hives after insult suggest the diagnosis
- 2.
Develop only in people who are allergic
- 3.
Insect stings, not insect bites, are a common cause of anaphylaxis
| Frequency (%) a | Etiology | History | Physical Examination | Differential Diagnosis | Laboratory Test | |
|---|---|---|---|---|---|---|
| Insect bite reactions | 0.7 | Stinging and biting arthropods | Insect often not seen by patient | Papules with central puncta, and often grouped Asymmetric distribution | Urticaria Impetigo Mucha–Habermann disease | – |
| Keratosis pilaris | Not known | Unknown | Bothersome rough bumps | Follicular, monomorphic papules Extensor arms and thighs and facial cheeks | Acne Lichen nitidus Lichen spinulosus | – |
| Lichen planus | 0.6 | Unknown | – | Purple, polygonal flat-topped papules with Wickham’s striae Can be generalized: wrists, ankles, and mucous membranes favored | Lupus erythematosus Lichen planus-like drug eruption Graft-versus-host disease | Biopsy |
| Miliaria | 0.1 | Sweat duct occlusion | Fever or occlusion of affected skin | Numerous small papules Trunk, especially back, usually affected | Contact dermatitis Folliculitis Candidiasis | Biopsy (not usually necessary) |
| Scabies | 1.5 | Mite | Other close contacts often affected | Burrows (when found) diagnostic Generalized distribution sparing head Genitalia often affected | Essential dermatitis | Scraping |
a Percentage of new dermatology patients with this diagnosis seen in the Hershey Medical Center Dermatology Clinic, Hershey, PA.
Definition
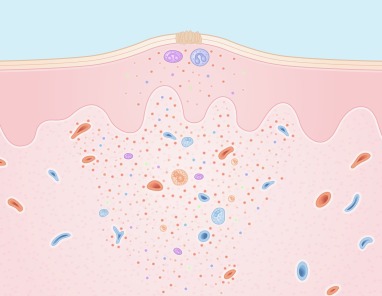
Insect bites, stings, and infestations produce local inflammatory reactions ( Fig. 11.1 ) in response to injected foreign chemicals and protein. Acute skin reactions appear as hives or papular urticaria, and more chronic reactions appear as inflammatory papules. Insects that sting (usually when threatened) include bees, wasps, and fire ants. Insects that bite (usually out of hunger) include mosquitoes, fleas, flies, bedbugs, and lice. Spiders, ticks, and chiggers are other arthropods that sometimes attack human skin.

Incidence
Most insect bites are recognized as such and are not brought to a physician’s attention. Anaphylactic reactions occur in 0.5% to 1.5% of stings. In the United States, yellow jackets are the leading cause of allergic insect sting reactions. In southern United States, fire ants are the leading cause of these reactions.
Insect bites and stings are primarily a seasonal phenomenon.
History
When someone is stung by an insect, the insult is usually remembered because the sting induces immediate pain. This is not always the case for biting insects; some delay may occur between the actual bite and the itching that follows. If the physical examination suggests insect bites (even when the patient is unaware of having been bitten), the history should be pursued carefully for possible exposures. For indoor exposure, fleas are common offenders. We inquire not only about pets currently living in the dwelling but also about whether pets recently occupied the premises. If a house had been occupied previously by flea-infested pets, the abandoned hungry fleas may form a welcoming party for the newly arrived human guests. We also ask about pets in homes visited by the patient. Spiders are sometimes responsible for indoor bites; their presence requires a careful search of the home. Bedbugs are becoming an increasingly recognized household insect that likes to bite in groups of three, commonly referred to as ‘breakfast, lunch, and dinner’ ( Fig. 11.2 ). Bedbugs often infest bats and birds and then hide in cracks and crevices, attacking the susceptible, sleeping victim in early morning hours. Infestations with head lice often occur epidemically in school children, so a history of affected playmates should be sought and the school nurse consulted.
“Indoor” insects:
- 1.
Fleas
- 2.
Spiders
- 3.
Bedbugs
- 4.
Lice

Contrary to some misconceptions, it is not necessary for other persons dwelling in the same household to be affected. For insect bite reactions, two factors are required: a biting insect and a host who is allergic to the bite. Not all people are sensitive, and not all people attract insects equally.
Papules and, in highly allergic individuals, bullae occur only in people who are allergic and who attract the insects ( Fig. 11.3 ).

Physical Examination
The reaction to a sting is usually an immediate hive, often with a central punctum, that resolves within a few hours. Large local reactions, manifesting as extensive erythema and swelling at the bite site, resolve after several days. Of the stinging insects, only the honeybee leaves behind its stinger, which on close inspection appears as a sharp barb projecting from the skin. If found, this stinger should be removed gently to prevent release of additional venom from the attached venom sack. Fire ants produce multiple itching hives, which quickly progress to painful papulovesicles and pustules. The bite of a recluse spider is unique in that it produces a severe local necrotic reaction with ulceration ( Fig. 11.4 ). Although the bite may be “quiet,” the reaction that ensues over the following days is not. Chiggers favor the legs and areas of tight-fitting clothing where they produce inflammatory papules and vesicles, and occasionally even bullae ( Fig. 11.5 ). Ticks painlessly burrow their heads in the skin, and pubic lice (pediculosis pubis) attach to hair; both can be visualized macroscopically. Head lice (pediculosis capitis) may be difficult to find but should be suspected in the presence of itching of the scalp, particularly the occiput or peripheral scalp ( Fig. 11.6 ). The eggs (nits) are most often found and appear as small, 2- to 3-mm, oval, translucent concretions affixed to hair shafts. Similar findings occur in body lice (pediculosis corporis) and pubic lice (crabs, pediculosis pubis).



Physicians are most often consulted for insect bites that produce itching papules. These typically are grouped and asymmetric. Flea bites frequently occur in streaks of three: “breakfast, lunch, and dinner.” Sometimes, a central punctum can be identified in the papule; this is diagnostic. If the offending insects remain in the environment, new lesions will continue to appear. Occasionally, only excoriations are found.
Differential Diagnosis
For patients with urticarial reactions, other causes of urticaria (see Chapter 16 ) may be considered. When the hive has a central punctum, however, its cause is an insect bite. Other foreign bodies can induce pruritic papules in the skin. Fiberglass is an example. This diagnosis can be suggested by the history, and confirmed by the presence of refractile material in the epidermis on biopsy or skin scraping. Delusions of parasitosis is a severe, chronic medical condition characterized by crusted papules and scars from “skin picking.” Patients suffer from a false, fixed belief that “bugs are under my skin.” Diagnosis and treatment require psychiatric evaluation and treatment ( Fig. 11.7 ) . Dermatitis herpetiformis (see Chapter 10 ) is in the differential diagnosis, particularly when only excoriations are found. Excoriation may also lead to secondary infection and a diagnosis of impetigo (see Chapter 12 ). An uncommon idiopathic disorder, pityriasis lichenoides, presents with scattered necrotic papules and vesicles that can resemble insect bites but are usually more generalized and symmetric. A skin biopsy helps to distinguish pityriasis lichenoides disease from an insect bite reaction (see later in this chapter).
- ●
Urticaria
- ●
Delusions of parasitosis
- ●
Dermatitis herpetiformis
- ●
Pityriasis lichenoides

Laboratory and Biopsy
The diagnosis is usually made clinically. Skin testing with commercial venom kits can be performed by an allergist. A biopsy, if performed, shows a wedge-shaped superficial and deep cellular infiltrate, so dense that it may be mistaken for malignant lymphoma. An insect bite is suggested by virtue of a mixed inflammatory cell infiltrate, which includes numerous eosinophils ( Fig. 11.8 ).
Therapy
The primary therapy is to remove the offending insect from the environment of the patient, or vice versa. Insects that are attached to the skin can be gently removed with tweezers (e.g., ticks) or killed chemically (e.g., lice) with agents such as permethrin creme rinse (Nix). For lice, fomite transmission is proven as adult lice can live away from human host for 3 days and nits can live for 10 days. Most lice treatments are pediculicidal, but not ovicidal, and require a retreatment in 7 to 10 days. For fleas, not only must the pet be treated, but also the house must be professionally fumigated. Insect repellent containing diethyltoluamide (DEET) remains a safe and effective deterrent to insect bites, especially ticks, with lowest effective dose of approximately 30%. Permethrin application to clothing also repels ticks, agents responsible for Lyme disease (see Chapter 16 ) and Rocky Mountain spotted fever. Colognes, perfumes, and scented hair sprays can attract insects and should be avoided in sensitive individuals.
Successful treatment of flea bites includes fumigation of the home.
Treatment of the inflammatory reaction of the skin is symptomatic. Topical steroids, systemic antihistamines, and occasionally systemic steroids may be helpful in relieving the itching.
Initial
Separation of host from insect
- ●
Lice: topical permethrin
- ●
Fleas: house fumigation
- ●
Bedbugs: house fumigation
- ●
Ticks: DEET repellent and permethrin on clothing
Symptomatic therapy for itching:
- ●
Topical steroids (e.g. clobetasol 0.05% cream b.i.d. × 2 weeks)
- ●
Antihistamines
Alternative
- ●
Lice: topical benzyl alcohol and malathion
- ●
Symptomatic therapy for itching: systemic steroids
- ●
EpiPen for highly allergic individuals
Course and Complications
In highly sensitive individuals, stings can produce serious anaphylactic reactions, mediated through immunoglobulin E, that occasionally result in death. Patients with anaphylactic reactions require prompt therapy with epinephrine, antihistamines, and, often, systemic steroids. Patients with severe reactions are likely to have severe reactions to future stings. Subsequent “desensitization” immunotherapy is frequently indicated for future prophylaxis. Immunotherapy is not necessary, however, in most children with urticarial reactions, even when these reactions are severe and generalized, as long as symptoms are confined to the skin. It is advisable, however, for such patients to have injectable epinephrine (Ana-Kit, EpiPen) readily available, especially when picnicking, hiking, or camping.
Most insect bite reactions resolve spontaneously and uneventfully. Secondary infection may occur, particularly when the patient has been scratching excessively. Scratching and infection can lead to scarring. A persistent local reaction to the bite of an infected deer tick is a characteristic finding in Lyme disease and is called erythema migrans (see Chapter 16 ).
Pathogenesis
Most insect bite reactions are the result of host allergy to injected secretions, including venoms (from stinging insects) and enzymes. Histamine, acetylcholine, and other vasoactive chemicals have also been isolated from the venom of stinging insects, and these, too, may play a role in the immediate reaction. However, the primary mechanism for insect bite reactions is allergic. The degree of host allergy determines the intensity of the reaction, which ranges from none to severe. As exemplified by erythema migrans , cutaneous reactions to insect bites may also be caused by microorganisms transmitted by the bite.
Keratosis Pilaris
- 1.
Involves extensor arms and thighs and face
- 2.
Follicular papules
- 3.
Appearance is bothersome
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


